IJCRR - 8(2), January, 2016
Pages: 84-90
Date of Publication: 22-Jan-2016
Print Article
Download XML Download PDF
A COMPARITIVE STUDY BETWEEN VAGINAL HYSTERECTOMY AND LAPAROSCOPICALLY ASSISTED VAGINAL HYSTERECTOMY
Author: Kavitha G., Renukadevi B., Rathna Ramamurthi, Rajarajeshwari S.
Category: Healthcare
Abstract:Introduction: Hysterectomy is the second most common surgical procedure performed by an Obstetrician and gynecologist next to Cesarean section. It can be performed by various methods, depending upon the pathology in the uterus, size of the uterus and the skill of the surgeon. Though there are a lot of advances in laparoscopic surgeries, most of the senior gynecologists feel that the laparoscopic hysterectomy have to replace abdominal hysterectomies but not vaginal hysterectomy and when ever feasible vaginal hysterectomy should be the method of choice for most cases of benign gynecological disease requiring hysterectomy. Objectives: The objective of the study is to compare the surgical and immediate post operative outcome for vaginal hysterectomy (VH) with those of laparoscopic assisted vaginal hysterectomy (LAVH). Methodology: This was a retrospective comparative study conducted among 200 patients who underwent vaginal hysterectomy/ (VH) laparoscopic assisted vaginal hysterectomy (LAVH) for various indication in the department of obstetrics and gynecology of Velammal medical college hospital and research centre from august 2012 to august 2015 (over period of 3yrs). The data were collected from medical records of the patient. The patients were divided into two groups of 100 each. Patients who underwent vaginal hysterectomy were grouped as VH and patients who underwent laparoscopic assisted vaginal hysterectomy were grouped as LAVH. The data was collected in terms of age, parity, history of previous surgeries, indications for surgery, operative time, and blood loss during surgery, intra-operative complication, post-operative complication and duration of hospital stay. The results were statistically analyzed with SPSS 16.0 version. Results: The baseline characteristics of both groups were similar. The mean operative time for the VH group was 90 minutes and 148 minutes for LAVH group (p=0.00). The mean blood loss for VH group was 152ml and 66ml for LAVH group (p=0.00). The incidence of vault hematoma was significantly more in the VH group and paralytic ileus was significantly higher in LAVH group. There was no significant difference between both groups in the incidence of hemorrhage, visceral injury and post operative pyrexia. Conclusion: Vaginal hysterectomy should be the preferred route of hysterectomy for benign conditions of the uterus whenever feasible, as it is associated with shorter operative time and early disappearance of post-operative pain.
Keywords: Vaginal hysterectomy, Laparoscopic assisted vaginal hysterectomy, Operative time, Post-operative pyrexia, Vault- hematoma, Paralytic ileus
Full Text:
INTRODUCTION
In a country like India, were resources are limited, women generally refuse medical management and conservative surgical management for most of the benign uterine pathology, so hysterectomy has become one of the most commonly performed gynecological operation. Up to 20% of women undergo hysterectomy by the age of 601. Most common reasons for performing hysterectomies are fibroid uterus, menstrual irregularities, endometrial hyperplasia, cervical dysplasia, genital malignancies, endometriosis, adenomyosis and genital prolapse.
Traditionally uterus has been removed by either the abdominal or vaginal route. Nowadays, we distinguish three different surgical approaches to hysterectomy: vaginal, abdominal, and laparoscopic. There is no universal agreement among gynecologist about the optimal route of hysterectomy for various uterine pathologies. Origin of Vaginal hysterectomy dates back to the ancient times. There is reference that vaginal hysterectomy was performed by Themison of Athens in 50 BC2 . The first authenticated vaginal hysterectomy was performed by the Italian anatomist Berengario da Carpi of bologna in 15073 .
The first planned vaginal hysterectomy for non prolapse uterus with entry into the peritoneal cavity was done for cervical cancer in 1822 by Santer of Baden3 . The most common cited contraindication to vaginal hysterectomy is uterine size, nulliparity and uterine descent, need for oophorectomy and previous abdominopelvic surgery and extrauterine disease. The first vaginal hysterectomy with laparoscopic assistance was described in 1984. The true role of laparoscopy in facilitating vaginal hysterectomy was to convert cases that could be done only by abdominal route to a laparoscopically assisted vaginal hysterectomy. Laparoscopic assistance during vaginal hysterectomy not only provides visualization of the real anatomic picture in the abdominal cavity, but allows the surgeon to perform correction of the associated pathology and some steps of the hysterectomy itself, thus reducing the operative risk of this, to a certain degree, ‘blind intervention. Kovac4 has described a scoring system which involves grading of uterus, length of infundibulopelvic ligament, presence of adnexal adhesion, status of cul-de-sac, and degree of endometriosis.
Patients with scores of 10 or less were considered as candidates for vaginal hysterectomy; those with 11- 19 were candidates for laparoscopic surgery to reduce their scores to less than 10. ACOG established some guidelines for the route of hysterectomy by staging that the choice depends on the patient’s anatomy, surgeons’ experience, and that vaginal hysterectomy is usually performed in women with mobile uterus not larger than 12 weeks gestation, especially if there is uterine descent. The purpose of this study was to compare laparoscopic assisted vaginal hysterectomy versus vaginal hysterectomy in terms of surgery time, total blood loss, post operative stay in hospital, intra operative and post operative complication.
MATERIAL AND METHODS This was a retrospective comparative study done among 200 women who underwent laparoscopic assisted vaginal hyster ectomy or vaginal hysterectomy for various indications in the department of obstetrics and gynecology of Velammal medical college hospital and research institute. The study was conducted over a period of 3yrs from August 2012 to August 2015.
Method of Collection of data The data of the patients were obtained from hospital medical records. The first 100 cases of laparoscopic assisted vaginal hysterectomy were compared with the cases of first 100 cases of vaginal hysterectomy among women who met the eligibility criteria, done during the study period. The patients were matched for pathological diagnosis, age, parity, size of uterus between laparoscopic assisted vaginal hysterectomy and vaginal hysterectomy group. Group VH was designated for patients who underwent vaginal hysterectomy and LAVH was designated for patients who underwent laparoscopic assisted vaginal hysterectomy. Medical records of the patients were reviewed; factors examined included demographic details, indication for surgery, and history of previous surgeries, intra operative details, post operative recovery and complication.
Inclusion Criteria Women who underwent vaginal hysterectomy or laparoscopic assisted vaginal hysterectomy for Fibroid uterus, Adenomyosis, AUB, Cervical dysplasia and Postmenopausal bleeding and with size of uterus measuring less than or equal to16 weeks size were included in the study.
Exclusion criteria Women who underwent vaginal hysterectomy or laparoscopic assisted vaginal hysterectomy for Malignancies of cervix, endometrium, ovary and size of uterus measuring more than from the study 16 weeks were excluded from the study.
Operative procedure A standardized procedure for vaginal hysterectomy was followed. The procedure started with a circumferential incision all along the uterine cervix, followed by anterior and posterior colpotomies. The cardinal and uterosacral ligaments were clamped, cut and ligated on both the sides. Then the bilateral uterine vessels were clamped, cut and ligated, followed by the clamping, cutting and ligation of cornual structures. Finally the vaginal cuff closure was done. Laparoscopic assisted vaginal hysterectomy were started by introducing a 10mm trocar and canula supraumbilically to hold the camera. Two 5mm trocar and canula were inserted into the lower abdomen. Bilateral round ligaments, the fallopian tubes and ovarian ligaments were electrocoagulated and cut. The vesicouterine fold of peritoneum was opened using monopolar hook and rest of the procedure were accom- plished by vaginal route.
At the end of procedure the peritoneal cavity was inspected laparoscopically for hemostasis. The size of the uterus was measured in weeks of pregnancy. The operative time was calculated from the first incision to end of wound closure. The blood loss was estimated by calculating the blood volume in the suction apparatus and by weighing the swabs. Major and minor intra operative complication and post operative complications like hemorrhage requiring transfusion or re-operation, visceral injury to bladder, bowel or ureter, conversion to laparotomy, fever ( >380 c in two consecutive occasions more than or equal to four hours apart after 24 hrs of surgery), paralytic ileus and vault hematoma. Day of disappearance of pain was the post operative day when the patient needed no analgesics.
The patients were discharged from the hospital when they were pain free, able to tolerate normal diet, apyrexic and ambulant. The collected data was analysed with SPSS 16.0 version. The descriptive statistics, frequency analysis, percentage analysis were used for categorical variables and the mean and standard deviation was used for continuous variables. To find the significant difference between the bivariate samples in Independent groups (VH and LAVH) unpaired sample t-test was used. To find the significance in categorical data ChiSquare test was used. In both the above statistical tools the probability value P<0.05 is taken as significant (S).
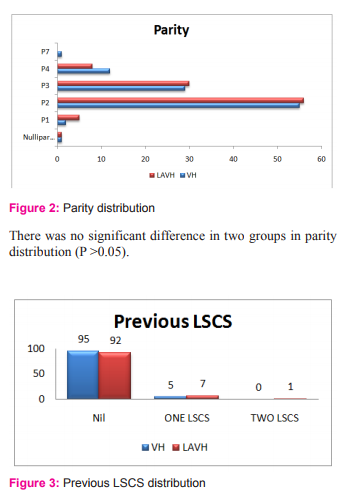
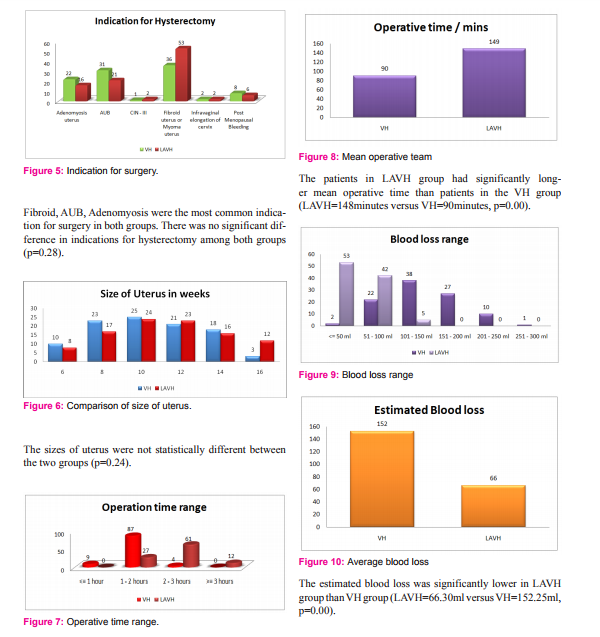
RESULTS There was no significant difference between both groups in age distribution (p=0.44), parity (p=0.68), number of cases with previous cesarean section (p=0.50) and indication for hysterectomy (p=0.28).
Baseline characteristics
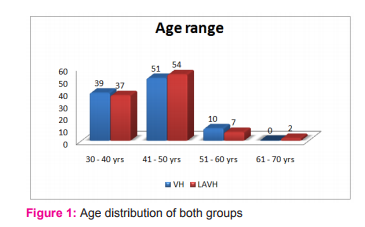
The mean age of patients in VH was 42.79yrs and 43.6yrs in LAVH group. There was no significant difference in two groups in age distribution (P >0.05).
There was no significant difference in two groups in the distribution of previous LSCS cases (P >0.05).

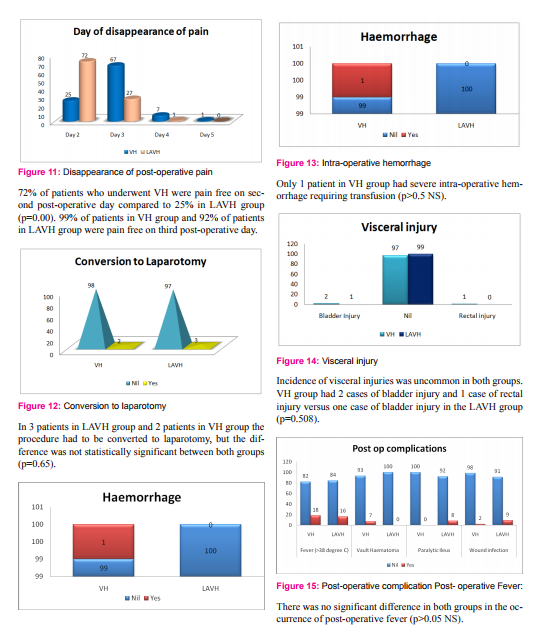
Vault hematoma: 7 cases of vault hematoma were seen in VH group against 0 cases in LAVH group (P < 0.05)
Paralytic ileus: 8 cases of paralytic ileus in LAVH group against 0 cases in VH group (p< 0.05).
Wound infection: There were 2 cases of vault infection in VH group and 9 cases of port site infection in LAVH group (p<0.05).
DISCUSSION
Laparoscopic hysterectomy has never been indicated for hysterectomy if the surgery is feasible by vaginal route. Laparoscopic assisted vaginal hysterectomy is a useful adjunct to vaginal hysterectomy for lysis of extensive adhesion and sometimes for concomitant surgery for adnexal pathology. A recent Cochrane review of surgical approach to hysterectomy for benign gynecological disease, involving 3643 women in 27 trials, concluded that the vaginal approach is preferred to the abdominal approach. When vaginal hysterectomy is not possible, laparoscopic hysterectomy may avoid the need for an approach by laparotomy. The purpose of our study was to compare the surgical and immediate post-operative outcome for vaginal hysterectomy with those for laparoscopically assisted vaginal hysterectomy. In our study there was homogeneity among demographic characteristics with regards to their age, parity, indications for surgery and uterine size. The most common indication for surgery in our study was fibroid uterus (44.5%), AUB (26%), Adenomyosis (19%), similar findings were found in a study by Shretha et al4 in which fibroids contributed to 53%, Adenomyosis (20%) and DUB (13.3%) of cases of hysterectomy. In literature, several studies report that operation time is longer with LAVH than VH6-12, 17. Even in our study the mean operating time was significantly shorter with VH than with LAVH (P=0.00).
This might be because the surgeries were performed by assistant professors who were well experienced in performing VH, but were comparatively less experienced in performing LAVH, and as we know the learning curve of VH is very short compared to laparoscopic surgery. In our study LAVH group had less blood loss compared with VH (P=0.00), similar to that observed by Summit et al13 (100-1000ml in VH versus 25-100ml in LAVH) and Aniuliene R et al14, but unlike to that observed by Ottosen C et al, Doucette et al, Riberio SC et al7, 5, 9 that blood loss was less in VH. Intra-operative complication (visceral injury and hemorrhage) rates did not significantly differ between both groups in a study by Abdelmonem A et al15. The incidence of vault hematoma was significantly more in VH group than LAVH group in our study; this may be because during laparoscopic approach hemostasis is checked at the end of the procedure16. In our study the incidence of paralytic ileus was significantly high in the LAVH group, probably due to the prolonged procedure time and bowel handling.
CONCLUSION
Vaginal hysterectomy can be considered as a preferable route of hysterectomy for uterine sizes less than 16weeks because it involves shorter operative time, earlier disappearance of post-operative pain and lesser incidence of paralytic ileus and wound infection. LAVH can be considered as a better approach to larger uterus in view of easier approach to upper pedicle, better visualization of adnexal pathology, lesser blood loss and lower incidence of vault hematoma.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Ethics committee approval: Obtained Informed consent: Obtained from each patient Source of funding: None Conflicts of interest: None
References:
1. Royal college of Obstetricians and Gynaecologists. National Evidence - based Clinical Guidelines. The management of menorrhagia in secondary care. London, Engl: RCOG Press, January 1999.
2. Sutton C. Past, Present and Future of hysterectomy. J Minim Invasive Gynecol. 2010 Jul- Aug; 17(4):421-35.
3. Baskett TF. Hysterectomy: evolution and trends. Best Pract Res Clin Obstet Gynaecol. 2005;19:295-305.
4. Kovac SR. Guidelines to determine the route of hysterectomy. Obstet Gynecol 1995 Jan;85(1):18–23.
5. Shrestha R, Yu LH. Comparison between laparoscopic hysterectomy and abdominal hysterectomy. NJOG. 2014JanJun;17(1):26-8.
6. Ottosen C, Lingman A, Ottosen L. Three mehods for hysterectomy: a randomized, prospective study of short term outcome. BJOG. 2000;107(11):1380-5.
7. Doucette RC, Sharp HT, Alder SC. Challenging generally accepted contraindication to vaginal hysterectomy. Am J Obstet Gynecol. 2001Jun;184(7):1386-9.
8. Ribeiro SC, Ribeiro RM, Santos NC, Pinotti JA. A randomized study of total abdominal, vaginal and laparoscopic hysterectomy. Int J Gynaecol Obstet. 2003 Oct;83(1):37-43.
9. Garry R, Fountain J, Mason S, Hawe J, Napp V, Abbot J, et al. The evaluate study; two parallel randomized trial, one comparing laparoscopic with abdominal hysterectomy, the other comparing laparoscopic with vaginal hysterectomy. BMJ. 2004 Jan 17;328(7432):129.
10. Cook JR, O’Shea RT, Seman EI. Laparovaginal hysterectomy: a decade of evolution. Aust N Z J Obstet Gynaecol. 2004 Apr;44(2):111-6.
11. Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2006 Apr 19;(2):CD003677.
12. Richardson RE, Bournas N, Magos AL. Is laparoscopic hysterectomy a waste of time Lancet. 1995 Jan7;345(8941):36-41
13. Summit RL Jr, Stovall TG, Steege JF, Lipscomb GH. A multicenter randomized comparison of laparoscopically assisted vaginal hysterectomy and abdominal hysterectomy in abdominal hysterectomy candidates. Obstet Gynecol. 1998 Sep;92(3):321- 6.
14. Aniuliene R, Varzgaliene L, Varzgalis M. A comparative analysis of hysterectomies. (Article in Lithuanian). Medicina (Kaunas). 2007;43(2):118-24.
15. Abdelmonem A, Wilson H, Pasic R. Observational comparison of abdominal, vaginal and laparoscopic hysterectomy as performed at a university teaching hospital. J Reprod Med. 2006 Dec;51(12):945-54
16. Karl Olah. Vaginal hysterectomy in the absence of prolapse. The obstetrician and Gynaecologist. 2005 Oct; 7:233-40.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





