IJCRR - 13(6), March, 2021
Pages: 93-95
Date of Publication: 20-Mar-2021
Print Article
Download XML Download PDF
A Novel Quality Improvement Approach to Improving Physical Healthcare Monitoring in an Acute Mental Health Unit
Author: Rasan Burhan, Thron Miah, Raza Butt
Category: Healthcare
Abstract:Introduction: Quality Improvement is an integral part of health service delivery and is one of the foundations of clinical govern�ance. This is a system whereby organisations improve the quality of the services they provide whilst protecting high standards to ensure that an environment of excellence in clinical care. Objective: This quality improvement project focused on Parity of Esteem \? the need to provide high-quality care from both a physical and mental health perspective. Methods: The project was implemented into an acute psychiatric inpatient ward and involved creating a tool to facilitate and streamline the focus on this; combined with methods to raise awareness in the ward. The objective was to improve the recording of physical healthcare parameters and follow through with the required interventions for patients under our care. Result: Signifi�cant improvements in the recording of health parameters and the follow-through of evidence-based guidelines for the patient population. Nine out of ten cardiometabolic health parameters saw an improvement in recording and they all showed improve�ment in follow-through of interventions. Conclusion: Mental health trusts should look into ways of streamlining their recording and interventions of guidelines by creat�ing simple to use, easy to follow tools that all staff are aware of and follow in the course of their work.
Keywords: Clinical Guidelines, Healthcare, Progress, Patient-centered care, Multimorbidity
Full Text:
Introduction
Parity of Esteem is the principle whereby physical health is given equivocal importance to mental health - due to the inextricable link between them. The relationship between physical and mental health is such that poor mental health leads to poor physical health, and vice versa. This principle was embedded into the Health and Social Care Act 2012.1 This came in response to the finding that patients in mental health services often have high morbidity and mortality rates concerning their physical health outcomes, and steps must be taken to address this.2 It was deemed of such high priority and concern that it was highlighted as one of the 13 National Indicators under the clinical quality and transformational indicators goals for 2017-2019: The need to improve physical healthcare to reduce premature mortality in people with serious mental illnesses.3
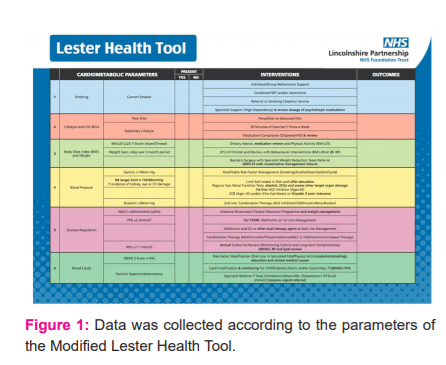
The Lester Health Tool was developed in 2014 to combat this, and consists of recording a series of cardiometabolic parameters for patients, and applying relevant associated interventions.4However, despite the extensive evidence base incorporated into the tool, it was often difficult for staff to use (due to time and system constraints).
To address this, the authors developed a Modified Lester Health Tool to achieve the same desired effect; in a simple and user-friendly mat. The Modified Lester Health Tool involved simplifying the categorisation of the cardiometabolic parameters into an easy to follow checklist. The interventions were also simplified for each domain (diabetes, obesity, hypertension and lipid modification) according to guidelines set out by the National Institute for Health and Care Excellence.
MATERIALS AND METHODS
Initial data were collected from a population sample of 18 patients at an acute mental health inpatient unit. Data were collected according to the parameters of the Modified Lester Health Tool (Figure 1), which was utilised in every ward round (Figure 2). Data were extracted from the Silverlink database.5
The Modified Lester Health Tool was subsequently introduced to the inpatient unit after a roundtable discussion with medical and nursing staff – leading to all key stakeholders buying into the implementation of the tool.
All members of staff on the ward were trained in how to optimally utilise the tool - executing the relevant interventions as guided. This involved staff teaching on the adapted tool embedded into the trusts Information technology (IT) system. Teaching sessions were given as one-on-one and group tutorials to staff on the ward – at various time-points. These include during times before and after the ward round - as well as during free periods for staff. Large posters were also put up across the ward to remind patients and staff of the tool - and the importance of its implementation. It was emphasised to staff that it’s not just important to screen but to also intervene.
Data was recollected 6 months following the implementation of the initial data set with a population sample of 15 patients.
Results
The study found that before the implementation of the health tool, there was minimal recording of patients cardiometabolic parameters within the inpatient unit. It was found that even where parameters were recorded, there were no active interventions on those parameters - when they would have triggered an intervention as per the National Institute of Health and Care Excellence (NICE) Guidance.
However, following the implementation of the Modified Lester Health Tool, there was a significant increase in the percentage of patients who had their cardiometabolic parameters recorded. Additionally, when these cardiometabolic parameters triggered the need for an intervention as per NICE Guidance, the Modified Lester Health Tool would prompt the clinicians to consider one of the NICE recommended interventions, which would be acted upon.
Quantitative data from the study showed the following improvements in recording parameters:
Smoking 78% to 100%. Diet 78% to 87%. Lifestyle 39% to 60%. Weight change 27% to 80%. BP remained at 100%. HbA1c 28% to 93%. Fasting Plasma Glucose 0% to 93%. Random Plasma Glucose 56% to 100%. Lipid profile 11% to 80%.
Follow through parameters showed improvement across the board:
Smoking 78% to 100%. Diet 30% to 87%. Lifestyle 0% to 60%. BMI 19% to 80%. Weight change 27% to 80%. Blood pressure 19% to 100%. HbA1c 28% to 93%. Fasting Plasma Glucose 0% to 93%. Random Plasma Glucose 56% to 100%. Lipid Profile 11% to 100%.
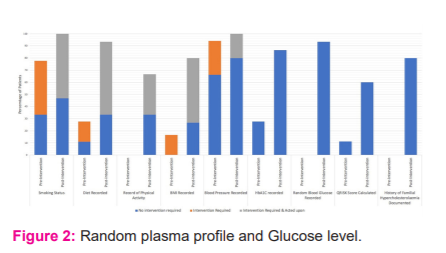
As shown here in Figure 2, nine out of ten parameters saw an improvement in the recording on the re-assessment and all ten parameters showed an improvement in the follow-through in the re-assessment.
Patients’ clinical characteristics in the ward were varied. Several patients were in relatively good physical health whilst others had systemic co-morbidities. There was also qualitative data observed from the study with patients beginning to ask questions about the calorie content of foods, and enquiring about how to be referred to for smoking cessation. Additionally, they were making very positive affirmations about wanting to improve their diet, improving their lifestyle and losing weight. This led to a positive atmosphere across the ward with an increased focus on developing and maintaining good health.
Discussion
The success of this quality improvement came about as a result of regular training for all staff, raising awareness of the project through the use of posters and accountability of staff via the tool - if parameters triggered were not being followed through. This involved a collective endeavour from all staff involved and patients – fostering initiative and proactivity. There were nevertheless some limitations noted in the project. For example, we had a minority of patients declining smoking cessation. To improve further we could look to developing integrated education programmes (videos and interactive sessions) on the ward to increase awareness regarding the dangers of smoking. Furthermore, the acute unit within which the design of the study was conducted was a female inpatient unit - hence it would be worthwhile expanding this to mixed-wards and male-only wards as well. We envision this would have equally positive outcomes.
To continue going forward, we should look to ensure training is provided at regular intervals and staff are updated with the latest statistics at regular meetings. This would help to ensure that the high-standards demonstrated are maintained going forward. This quality improvement project was a success and demonstrated the importance of developing interventions as a result of initial findings - as well as the importance of effective data collection. The project demonstrated a novel way to improve the morbidity and mortality of patients under our care - by effectively focusing on physical health parameters and treating these with equivocal importance to co-existing mental health diagnoses.
Funding
Funded by HC-UK for Presentation to NHS Quality Improvement Staff from trusts across the United Kingdom at the Annual Summit.
The Graphics team at the trust were commissioned by Lincolnshire Partnership NHS Foundation Trust to design and print posters as per the prototype.
Author Contributions:
Rasan Burhan: Project Lead
Thron Miah: Project Team
Raza Butt: Project Team
Ethics approval and consent to participate:
Approval obtained from QI/Audit Team at Institution
Competing interests:
No competing interests from any author
Acknowledgements:
With thanks to Dr KuganandaParanthaman (Medicine) and Dr BeenaRajkumar (Consultant Psychiatrist) for helping facilitate effective implementation of the project. With also extend our gratitude to all nursing and allied healthcare staff at the trust for co-operation with the project.
References:
1) Department of Health. GOV.UK. United Kingdom: Health and Social Care Act 2012 Fact Sheets; [updated April 2012; cited August 24 2020]. Available from: www.gov.uk/government/publications/health-and-social-care-act-2012-fact-sheets.
2) NHS England. NHS.UK. United Kingdom: Parity of Esteem (Valuing Mental Health Equally With Physical Health); [updated November 2013; cited August 24 2020]. Available from: www.england.nhs.UK/mentalhealth/parity.
3) NHS England. NHS.UK. United Kingdom: Commissioning for Quality and Innovation; [updated November 2016; cited August 24 2020]. Available from: www.england.nhs.uk/nhs-standard-contract/cquin/cquin-17-19.
4) Royal College of Psychiatrists. RCPsych.ac.uk. United Kingdom: Lester Adaptation of the Cardiometabolic Health Resource; [updated June 2014; cited August 2020]. Available from: www.rcpsych.ac.uk/docs/default-source/improving-care/ccqi/national-clinical-audits/ncap-library/ncap-e-version-nice-endorsed-lester-uk-adaptation.pdf
5) Patient Administration System [Computer Software]. Version 1.0. United Kingdom: Silverlink Software Limited; 2013.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





