IJCRR - 13(6), March, 2021
Pages: 72-76
Date of Publication: 20-Mar-2021
Print Article
Download XML Download PDF
An Evaluation of Best Corrected Visual Outcome (BCVA) after Nd-YAG Laser Posterior Capsulotomy in Patients of Posterior Capsular Opacification (PCO): A Prospective, Single Centre, Observational Study
Author: Nishant V Shah, Rajendra Choudhary, Meet Mashru
Category: Healthcare
Abstract:Introduction: Amongst multiple methods to treat thickened posterior capsular opacities occurring after cataract surgery, the Nd YAG (neodymium-doped yttrium aluminium garnet) Laser is preferred because it is non-invasive and it is an OPD basis proce�dure considering the comfort of the patients. Objective: The present study was carried out to measure the effectiveness of the Nd YAG laser in terms of Best Corrected Visual Outcome. Methods: A detailed ocular, systemic, family history was taken. The patient was asked about the record of their cataract surgery and all the details regarding the type of the surgery, preoperative evaluation was recorded by Snellen's chart, refractive status by auto-refractometer and subjective testing. Capsulotomy was done using VISUALS YAG IIIlaser of Zeiss company. The patient was followed up with the same evaluation procedure immediately post-laser within 1 hour, 1st-day post-laser, at 1 week, at 1 month. Results: Preprocedural visual acuity was impaired in 56 out of the 97 patients presented with visual acuity of 6/18. There was the visual improvement in all the patients as seen at the final follow-up after one month of the procedure. Conclusion: Nd YAG lasers provide a safe, simple, rapid relatively non-invasive and cost-effective treatment modality of poste�rior capsular opacification. More availability of Nd YAG lasers should be made in developing countries where posterior capsular opacity is the most common vision disturbing problem.
Keywords: Posterior Capsular Opacity (PCO), Posterior Capsulotomy, Nd-YAG Laser
Full Text:
Introduction
Secondary cataract, also known as posterior capsular opacification (PCO), is the most common complication after cataract surgery, resulting from migration and proliferation of residual epithelial cells onto the central posterior capsule, leading to decreased visual function, and ultimately decreased visual acuity.
Posterior capsular opacification of initially clear posterior capsule occurs frequently in patients after extracapsular cataract extraction of senile cataracts. Although the time of opacification is highly variable, PCO occurs in somewhere between 25% & 43% of patients by 5 years after cataract surgery.1 In adult patients, the usual time from surgery to visually significant opacification varies from few months to years and the rate of opacification declines with increasing age, while in younger age groups almost 100% opacification occurs within two years after surgery.2
Amongst multiple methods to treat thickened posterior capsule including capsulotomy with a knife, the Nd YAG laser is preferred because it is non-invasive and it is an OPD basis procedure considering the comfort of the patients.3 The Neodymium Yttrium Aluminium Garnet (Nd: YAG) laser with the wavelength of 1064nm as a pulsed instrument that acts by the formation of plasma at its focus point inducing an expansion of the tissue. 4 Patient enjoys instant and rapid improvement in the best-corrected visual acuity after the procedure as the procedure helps in clearing the visual axis completely. This improvement in vision is maintained as it is unless any other comorbidities of the eye or the complications of the procedure occur in due period.
In our study, we have used Nd: YAG laser for posterior capsulotomy as the technique is rapid, relatively safe and provides controlled opening of the posterior capsule. The instrument is easy to handle and the technique is simple, effective and has abolished many complications of the surgical methods. The vision was assessed by Snellen’s chart for distance visual acuity and for near visual acuity Jaegger’s charts are utilized.
MaterialS and Methods
This prospective, observational study was carried out with the primary objective to evaluate the Best Corrected Visual Outcome (BVCA) after Nd-YAG Laser Posterior Capsulotomy in Patients of Posterior Capsular Opacification in the ophthalmology department of GMERS Hospital, Gandhinagar, Gujarat for the total duration of two years between October-2017 to September-2019.
After obtaining the approval from the Institutional Ethics Committee (IEC) Dated 18/01/2017 with No. GMERS/MCG/IEC/02/2017, patients of either gender and above 18 years of age having a history of more than 6 months of previous cataract surgery and Intraocular Pressure (IOP) of <21 mm Hg with visual acuity <6/12 with Snellen’s chart having significant posterior capsular opacification were included in the study. Impaired Visual Acuity was defined as a decrease in best-corrected visual acuity post-operatively by three Snellen’s line or two- or less-line loss with symptoms of visual disturbance in carrying out daily work or skilled work. Patients of Posterior Capsular Opacity (PCO) unlikely to be benefited satisfactorily due to the presence of co-morbidities like Vitreous Opacities, Corneal Opacities, Retinal pathology accounting for the loss of vision, Co-existing Pseudo-exfoliation, Uveitis associated collagen vascular disorders, glaucoma, glaucoma suspect or ocular hypertension etc and history of previous intraocular surgery other than cataract surgery were excluded from the study. Patients age below 18 years, unable to fixate adequately for the procedure or not willing to give consent were not considered for participation in the study.
A detailed ocular, systemic, family history was taken. Patient were asked about the record of their cataract surgery and all the details regarding the type of the surgery, preoperative evaluation was recorded. Also, the immediate postoperative details were assessed and recorded. Pre-laser visual acuity by Snellen’s chart, refractive status by auto-refractometer and subjective testing were recorded. The patient was followed up with the same evaluation procedure immediately post-laser within 1 hour, 1st-day post-laser, at 1 week, at 1 month. BVCAwas measured by Snellen’s chart for distant vision. The patient was instructed to read the letters on the Snellen’s chart from a distance of 6 meters and the BCVA for distance vision was noted. Similarly, BCVA for near vision was recorded by using Jaeger’s chart for near vision. For refractive status, Auto-refractometer findings were recorded. Refractive status by subjective testing was assessed and recorded.
Capsulotomy was done using VISULAS YAG III laser of Zeiss company. Patients were informed about the procedure and written informed consent was taken. The eye undergoing procedure was dilated with eye drops Tropicamide 0.8% + Phenylephrine 5.0%. The procedure was performed in a dark room for better visualization of the opacification. The patient was properly positioned and instructed to fix the distant target with the fellow eye. Laser capsulotomy was started using minimal energy (0.8 mJ initially and increased as per the need). Shots of laser to be placed across the tension lines and openings to be created starting from 12’o clock position and moving towards 6’o clock position as per the need.
Post-laser topical antibiotics and steroid eye drops (Ofloxacin and Dexamethasone) were started four times a day for seven days to counteract post-laser infection and inflammation. Anti-glaucoma medication (Timolol maleate) was started if IOP> 21 mm Hg or increase in IOP by 5 mm Hg or more was recorded anytime during follow up.
Results
In our study, out of the 97 patients, 56 were female and the remaining 41 were male. The most common involvement was in the 61-70 years age group, while 87 out of the 97 patients were aged between 51 and 80 years.
The study showed right eye dominance with 52 right eye involvement compared to 45 left eye involvement. On Retrospective inquiries into the patient’s pseudophakia status, it was found the greatest number of patients had undergone Manual Small Incision Cataract surgery. (Table-1) Out of 97 patients, the most common type of PCO was Capsular Fibrosis, seen in 56 patients, with Elschnig’s pearls seen in 35 and Soemmerring’s ring seen in 6 patients.
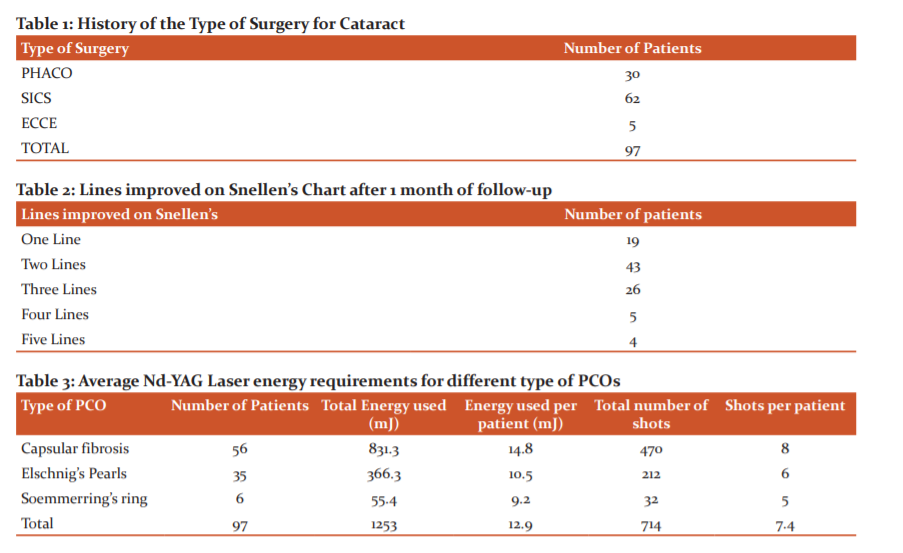
Visual acuity was recorded in all patients, pre and post-laser (Figures1 and 2). Preprocedural visual acuity was impaired in 56 out of the 97 patients presented with visual acuity of 6/18. Total energy used was 1253mJ with 714 shots with average energy per patient was 12.9 mJ and average shots 7.4 per patients approximately. Total energy and number of shots required per case were more in capsular fibrosis type than the other two types of PCO.
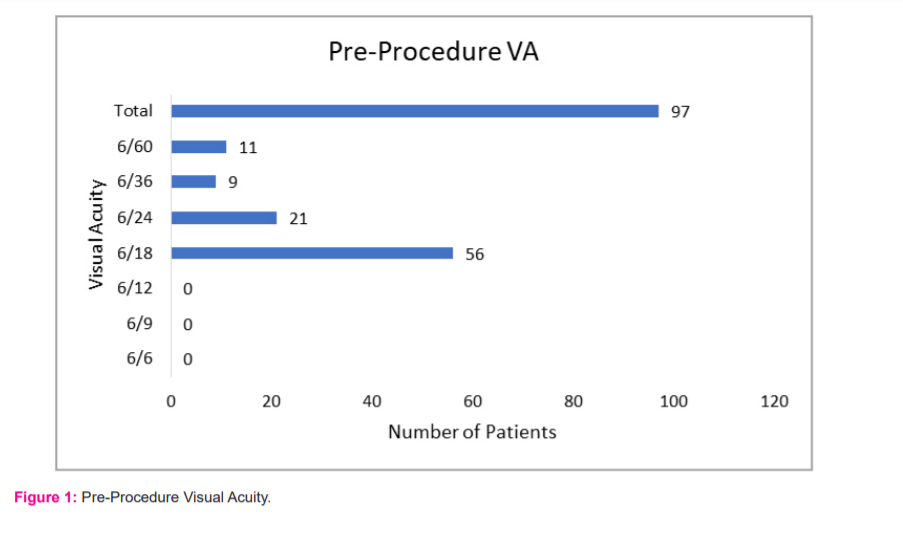
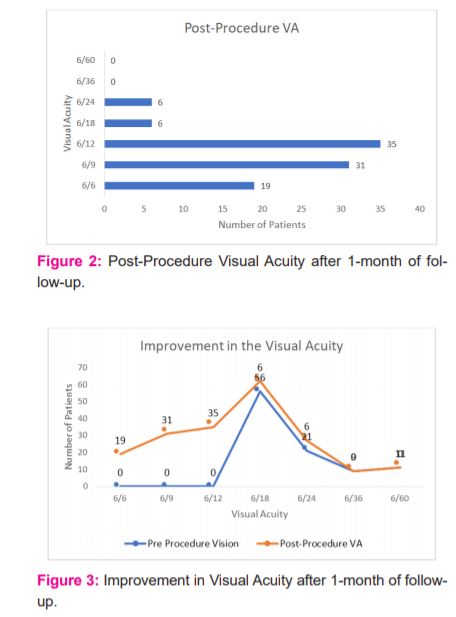
In 4 patients, visual acuity at 1-month post-laser improved by 5 Snellen’s lines. In 5 patients, visual acuity at 1-month post-laser improved by 4 Snellen’s lines. In 26 patients, visual acuity at 1-month post-laser improved by 3 Snellen’s lines. In 43 patients, the visual acuity at 1-month post-laser improved by 2 lines. In 19 patients, the visual acuity could be improved only 1 Snellen’s line. (Table-2) The most common post-procedural visual acuity on the final follow-up after 1 month was 6/12. There was the visual improvement in all the patients as seen after the final follow-up, after one month of the procedure (Figure 3).
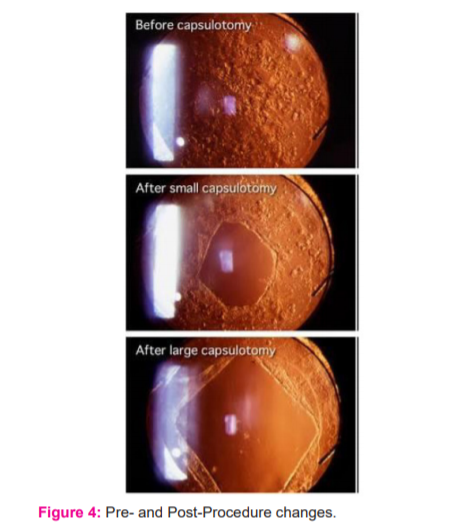
The actual changes seen at pre-and post-procedure of Nd-YAG Laser capsulotomy and the machine used in our study is depicted in Figures 4 and 5.
Discussion
Posterior capsular opacity is the most commonly reported vision – disturbing sequelae of modern cataract extraction. It is a condition with multifactorial aetiology, which is visually disabling after the good early postoperative vision. Visually significant posterior capsular opacity is decided based on visual disability that it gives rise to and the actual opacity observed, rather than relying on any morphological description only.
Incidences of posterior capsular opacity in different methods of cataract surgery were different. Also, the grades and the period for the patient to undergo laser capsulotomy after cataract surgery was different. Visual acuity improved in all, cases after Nd YAG capsulotomy. Comparing the parameters of pre and post laser measurements, there was a very significant difference.
This compares with studies conducted by others. Magno et al.showed similar results with visual acuity, contrast sensitivity curve and glare sensitivity curve in a study conducted by them in August 1997. 5 A similar study conducted by residents of Veterans Administration Hospital in April 2000 has results comparing favourably with our study. 6 A similar study in September 2002 showed similar results.
The Nd: YAG laser capsulotomy has fewer and less dramatic complications, is non-invasive, is simple and cost-effective when compared to the surgical discussion and is thus far superior to the surgical method as a treatment of posterior capsular opacity. The use of Nd: YAG laser in posterior capsulotomy has acquired its special place in ophthalmologists’ armamentarium in his endeavour to give satisfying visual status to the patients with cataracts.
Conclusion
Our study shows, Nd YAG lasers provides a safe, simple, rapid relatively non-invasive and cost-effective modality of posterior capsular opacification, so we suggest its usage and all-time availability in developing countries where posterior capsular opacity is the most common vision disturbing problem.
Acknowledgements: The authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: Nil
Conflict of Interest: None
Individual Author’s Contribution:
Dr. Nishant Shah: Study Design, Protocol Preparation, Procuring Permissions, Study Conduct, Study Follow-ups.
Dr Meet Mashru: Study Design, Study Conduct, Study Follow-ups
Dr Rajendra Choudhary: Study Design, Study Monitoring, Preparation of Manuscript and Manuscript Submission.
References:
-
Sundelin K, Sjöstrand J. Posterior capsule opacification 5 years after extracapsular cataract extraction. J Cataract Refract Surg 1999;25(2):246-250.
-
Raj SM, Vasavada AR, Johar SR, Vasavada VA. Post-operative capsular opacification: a review. Int J Biomed Sci 2007;3(4):237-250.
-
Aron-Rosa D, Aron JJ, Griesemann M, Thyzel R. Use of the neodymium-YAG laser to open the posterior capsule after lens implant surgery: a preliminary report. Am Intra-Ocul Implant Soc J 1980;6(4):352-354.
-
Wayne F.March: Ophthalmic Lasers: A Second Generation, The University of Michigan 1990, Slack Publisher, ISBN 1556420579.
-
Magno BV, Datiles MB, Lasa MS, Fajardo MR, Caruso RC, Kaiser-Kupfer MI. Evaluation of visual function following neodymium: YAG laser posterior capsulotomy. Ophthalmology 1997;104(8):1287-1293.
Skolnick KA, Perlman JI, Long DM, Kernan JM. Neodymium: YAG laser posterior capsulotomies performed by residents at a Veterans Administration Hospital. J Cataract Refract Surg 2000;26(4):597-601.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





