IJCRR - 13(6), March, 2021
Pages: 56-59
Date of Publication: 20-Mar-2021
Print Article
Download XML Download PDF
A Modified Approach in Fistula in ano by Interception of Fistula Tract and Ksharsutra (IFTAK) Method: A Case Study
Author: Prafulla Fadanvis, Amruta Tembhurnikar, Shubhada Guru, Poonam Madan, Anagha Hirapure, Swarupa Chakole
Category: Healthcare
Abstract:Introduction: Fistula in ano is a notorious disease to treat. Despite having recent technological advances Ksharsutra treatment is still useful. However, a few problems like pain, itching, discomfort at the anal region encountered during Ksharsutra treatment needs to be addressed. IFTAK (Interception of fistulous tract with the application of Kshara Sutra) is Interception of fistulous tract with the application of Ksharsutra. IFTAK technique is introduced by Dr. Manoranjan Sahu from Banaras Hindu University, in which the fistula tract is intercepted just outside sphincter muscles and Ksharsutra is inserted in it. Case: A 45 year male patient of grade III trans sphincteric fistula was treated with IFTAK method. Results and Conclusion: It was found more useful than the conventional Ksharsutra method as it reduced the duration of treat�ment. Associated complaints like itching, burning at the anal region during Ksharsutra were decreased.
Keywords: Problems of Ksharsutra, Fistula, Interception of fistulous tract with the application of Kshara Sutra
Full Text:
Introduction
Fistula-in-and is an inflammatory disease that forms a tract in the anal region with a primary internal opening in the anal canal and a secondary external opening on the perianal skin. It is an abnormal connection between two epithelized surfaces lined with granulation tissue. The main pathology lies in cryptoglandular infection in the intersphincteric region. Even after several advancements in fistula treatment, failures are quite high.1 It has been considered a notorious disease to treat due to its recurrence and incontinence. The chances of recurrence in different types of anal fistulae range between 7% and 50%.2 Ksharsutra is the most widely used treatment for fistula in and in India. Success rate and non-recurrence are surely appreciable but weekly sittings and pain during changing of Ksharsutra make it difficult for the patient to pursue the treatment.3 Also, the discomfort of Ksharsutra being in situ is significant to disturb the daily routine of the patient. Cutting and simultaneous healing of the fistula is time-consuming which depends on the length and type of fistula tract. So discomfort, irritation, itching, burning at the anal region persist during the treatment. Hence a new approach was mandatory.4,5
IFTAK is the Interception of the fistulous tract with an application of Ksharsutra. IFTAK technique is the procedure introduced by Dr. Manoranjan Sahu from Banaras Hindu University, Varanasi. This technique is also called a BHU technique for fistula-in-ano.4 This technique is mostly used for treating the complex fistula with a high recurrence rate.5 A fistula case treated with IFTAK method is discussed here.3,4
Case Study
A 45 male patient came to Shalya Tantra OPD of DMAMCHRC with complaints of pain at the perianal region on the left side of the buttock. The patient had a history of perianal abscess, blood mixed pus discharge from the right side of the buttock for 18 months which was treated conservatively by a physician. The patient presented with pain and swelling in the left perianal region for 15 days.
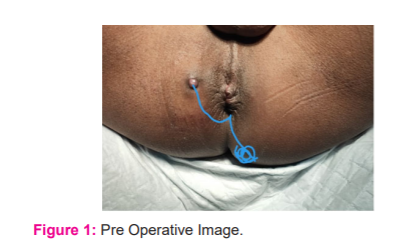
On examination, the patient was normotensive, non-diabetic without any other systemic disease. On local inspection in the lithotomy position, there was swelling, redness at 5 o’clock position on perianal region 6 cm away from the anal opening. There was also an opening on the perianal region at 10 o'clock 4 cm from the anal verge (Figure 1). On Palpation at 5 o’clock local temperature was raised with significant tenderness and induration. Induration was going radially towards the anal canal. Mild mucopurulent discharge from 10 o’clock skin opening was observed. On Per rectum examination a dimple was felt in the anal canal below the anorectal ring.
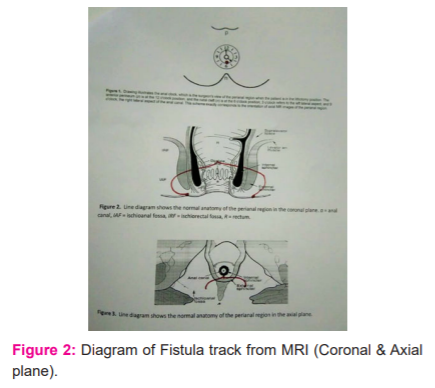
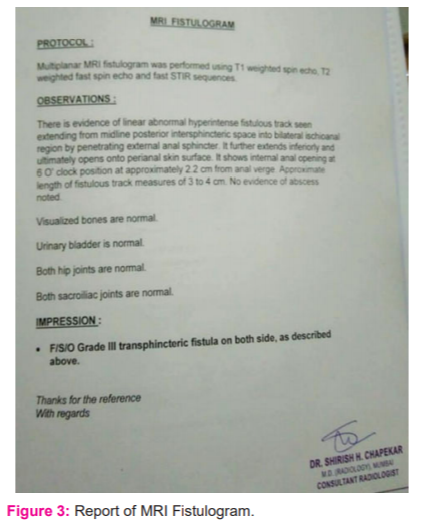
The patient had given a history of recurrent abscess and purulent discharge from the 10 o’clock opening. After history taking and physical examination diagnosis of fistula-in-and was confirmed. MRI Fistula (dated 25/01/2020) reported, Grade III transphincteric fistula on both side of the perianal region with the internal opening at 6 o’clock 2.2cm in the anal canal (Figures 2, 3)
After all preoperative investigations, the patient was posted for surgery under spinal anaesthesia.
In lithotomy position painting, draping and isolation of part were done. A small incision was taken on induration at 5 o’clock. The mild haemo-purulent collection was drained. The solution of Hydrogen peroxide and povidone-iodine was injected in the new opening at 5 o’clock and also old 10 o’clock openings. The solution was coming from the same internal opening at the 6 o'clock position. So intra-operative patency test findings were consistent with MRI fistula. The fistula tract with the anterior external opening at 10 o’clock was probed and found internal opening posteriorly at 6 o’clock. So the course of the tract was curvilinear. Probing from the posterior opening at 5 o’clock was going radially at the same internal opening in the anal canal.
With probe inside posterior fistula tract, a small incision was made at 6 o’clock just outside sphincter muscles approximately 2 cm from the anal verge. The incision was deepened with microtip artery forceps to expose the probed fistula tract. As both the tracts were transphincteric, the exposed fistula tract was intercepted by an incision on it just outside the sphincter complex. The probe was inserted from the new opening at 6 o’clock, guided out from the internal opening. The thread was inserted along with the probe. Anterior fistula tract was curetted, probed and guided out from the new external opening at 6 o’clock along with thread. The thread was also inserted in the posterior fistula tract from 5 o’clock to the external opening at 6 o’clock after curettage. All External openings were widened for proper drainage of secretions from the fistula. All the tracts were irrigated with H2O2 and povidone-iodine solution. The dressing is done with gauze packing. (Figures 4, 5) Postoperatively the patient was treated with IV antibiotics, anti-inflammatory, IV fluids and other appropriate medicine. The patient was discharged the next day.

Ksharsutra was inserted in the primary tract at the 6 o’clock position on the third day after subsiding surgical oedema. The other two tracts with the external opening at 10 and 5 o’clock were irrigated with Triphala Kwath and Jatyadi Tail. Plain threads in these two secondary tracts were kept for drainage for 1 week and then removed. Secondary tracts healed in the next 16 days (total 22 days after surgery). Ksharsutra in primary fistula was changed weekly for 4 more weeks to cut through (total of 5 weeks of treatment Figure 6).
During treatment, the patient was advised Saptavinshati Guggul 250 mg 2 tabs thrice a day. Gandhak Rasayan 250 mg 2 tabs thrice a day.

Discussion
Even after the success rate in the fistula, Ksharsutra causes irritation and pain till it is in situ. Unit cutting time for conventional Snuhi Ksharsutra is averagely 7days /cm.6 Duration of complete cut-through of fistula tract depends on length and type of fistula i.e. more time in transphicteric fistula. In this case, the fistula was transphincteric with two tracts anterior and posterior. The conventional method would have taken more than 8 weeks to cut and heal.7,8 In the IFTAK method fistula tract is intercepted just outside the sphincter muscles and Ksharsutra is inserted in it.4,5 In this patient also IFTAK was performed, rest of the track was corrected, widened and a seton was kept for drainage in both tracts which was removed after 1 week. Both tracts healed secondarily with minimal scarring. By this method length of the fistula tract was decreased with the new external opening at the point of interception, which ultimately reduced the duration of treatment to just 5 weeks.6-8 Main aim of Ksharsutra treatment is to deal with the cryptoglandular infection in an inter-sphincteric plane. By the IFTAK method also the main pathology is treated. Due to the decrease in duration of Ksharsutra treatment, associated discomfort like itching, burning at the anal region, pain during changing of Ksharsutra also decreased. So the patient gets back to disease-free condition sooner.
Conclusion
Interception of the fistula tract and Ksharsutra is useful than the conventional Ksharsutra method as it reduces the duration of Ksharsutra treatment. Associated complaints like itching, burning at the anal region during Ksharsutra are decreased. The use of this method will be helpful to attract more patient for Ksharsutra treatment.
Conflict of interest: Nil
Source of funding: Nil
References:
-
Emile S. Recurrent anal fistulas: When, why, and how to manage? World J Clin Cases 2020;8(9):1586-1591.
-
Bakhtawar N. Factors Increasing the Risk of Recurrence in Fistula-in-ano. Cureus 2019;11(3):e4200.
-
Dutta G, Bain J, Ray AK, Dey S, Das N, Das B. Comparing Ksharasutra (Ayurvedic Seton) and open fistulotomy in the management of fistula-in-ano. J Nat Sci Biol Med. 2015;6(2):406–410.
-
Sahu M. A manual on Fistula in ano and Kshara Sutra therapy published by NRC Dept. of Shalyatantra, IMS, BHU, First edition 2015.
-
Choudhary P. Interceptive less invasive Ksharsutra therapy in transphincteric fistula in ano. World J Pharma Res 2015;4:1641-1649.
-
Gupta R. Comparative Study Of The Effect Of Modified Kshar Sutra With That Of Standard Ksharsutra In The Treatment Of Fistula In Ano. IAMJ 2014;2(5):125-129.
-
Lamtur Y. entero-cutaneous fistula in an operated case of total abdominal hysterectomy: A rare case report. J Crit Rev2020;7(8):1085-1088.
-
Chandak S. Traumatic low fistula-in-ano. J Datta Meghe Inst Med Sci Univ 2019;14(3):256-257.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





