IJCRR - 13(6), March, 2021
Pages: 33-35
Date of Publication: 20-Mar-2021
Print Article
Download XML Download PDF
Clinical Profile of Upper Gastrointestinal Endoscopy Patients in a Tertiary Healthcare Facility: Cross-Sectional Research
Author: Rajesh Kothari, Sanjay Agrawal, Vineeta Kothari
Category: Healthcare
Abstract:Introduction: Upper gastro-intestinal haemorrhage is a common and potentially life-threatening gastrointestinal emergency with a wide range of clinical severity, ranging from insignificant bleeds to catastrophic exsanguinating haemorrhage, described as haemorrhage derived from a source proximal to the Treitz ligament. Objectives: Clinical profile of upper gastrointestinal endoscopy patients in a tertiary healthcare facility. Methods: This was a cross-sectional analysis carried out over two years at a tertiary health care centre with an Upper Gastro�Intestinal Endoscopy clinic. There were 252 patients referred for the procedure during this time. Upper gastrointestinal endos�copy with all aseptic precautions and normal procedures, all patients underwent USG after written and clarified consent, were entered into excel sheets and analyzed by SSPSS (Statistical Package for Social Sciences). Results: In our study, we found that patients had a mean age of 11.42 \? 6.22 years. The range was from 1-60 Yrs. The majority of patients were females or 52 per cent, and 48 per cent were males. Hematemesis under investigation was the most common provisional diagnosis - 22 %, followed by mass per abdomen at 16 %. In 25 % of cases, the most common USG findings were Coarse Ecotexture of Hepatic followed in 18 % by Diffuse Parenchymal Hepatic. Conclusion: From our study, it can be concluded that Hematemesis under study followed by Mass per abdomen was the most common provisional diagnosis. Coarse Ecotexture of Hepatic accompanied by Diffuse Parenchymal Hepatic modifications were the most common USG findings.
Keywords: Upper gastrointestinal endoscopy, Upper gastro-intestinal haemorrhage, USG-Abdomen
Full Text:
INTRODUCTION
Upper gastrointestinal haemorrhage is a common and potentially life-threatening gastrointestinal emergency, described as a haemorrhage derived from a source proximal to the Treitz ligament, with a broad range of clinical severity, ranging from insignificant bleeds to catastrophic exsanguinating haemorrhage, and is associated with significant morbidity and mortality.1,2 The frequency of upper gastrointestinal bleeding varies from a population of 50 to 150/100,000 each year and time trend analyses indicate that aged people represent a growing proportion of those with acute upper gastrointestinal bleeding. As many as 70% of acute upper gastrointestinal bleeding episodes occur in patients older than 60 years, and the incidence is likely to increase with age due to the increased intake in elderly patients of non-steroidal anti-inflammatory drugs (NSAIDs), which trigger ulcerogenic.3,4 Approximately two-thirds of all patients who have gastrointestinal bleeding in the emergency department have upper gastrointestinal bleeding as the trigger. As both have different treatment procedures and prognosis, patients can be divided as having either variceal or non-variceal causes of upper gastrointestinal haemorrhage.5 The first involves lesions due to portal hypertension, including gastroesophageal varices and portal hypertensive gastropathy; the second includes lesions found in the general population (peptic ulcer, erosive gastritis, esophagitis of reflux, Mallory-Weiss syndrome, tumours, etc.).6
MATERIALS AND METHODS
This was a cross-sectional analysis carried out over two years at the tertiary health care centre referred for Upper gastro-intestinal Endoscopy. 256 patients were referred for the procedure during this time. They were subjected to upper gastro-intestinal endoscopy with all aseptic precautions and normal procedures after written and explained consent. Both patients underwent USG & the findings were entered and evaluated by SPSS in excel sheets (Statistical Package for Social Sciences).
RESULTS
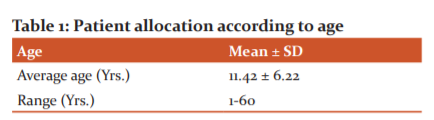
The patients had a mean age of 11.42 ± 6.22 years. The range was from 1-60 Yrs. (The Min-Max)
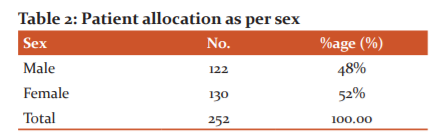
The majority of the patients were 52 % female and 48 % male.
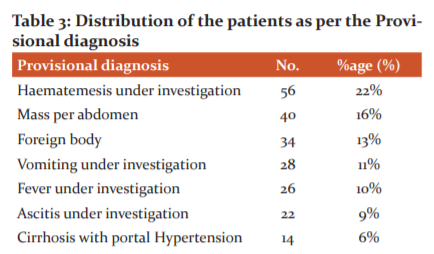
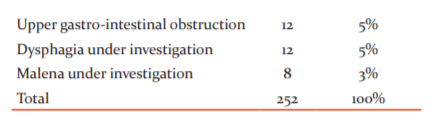
Hematemesis under investigation was the most common provisional diagnosis (56), accompanied by abdominal mass (40), foreign body (34), vomiting under investigation (28), fever under investigation (26), ascitis under investigation (22), cirrhosis with hypertension portal (14), upper gastrointestinal obstruction (12), dysphagia under investigation (12) and malena under investigation (12) (8).
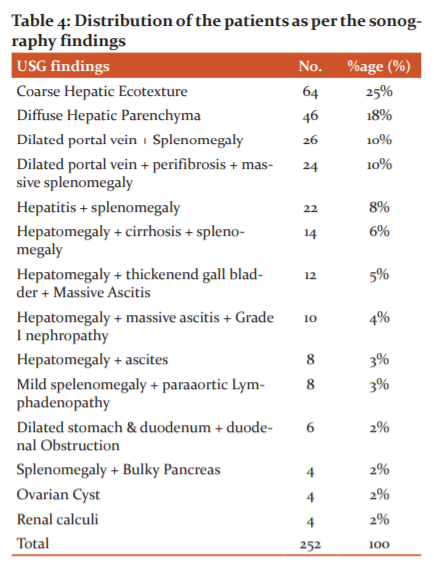
Coarse echotexture of the liver (64), diffuse liver parenchyma (46), dilated portal vein with splenomegaly (26), dilated portal vein with per fibrosis, massive splenomegaly (24), hepatitis with splenomegaly (22), hepatomegaly with cirrhosis of the liver with splenomegaly (14), hepatomegaly with thickening of the gall bladder with massive ascites (12), hepatomegaly with coarse echotechymia (14), hepatomegaly with thickening of the gall bladder with massive ascites (12), hepatomegaly with coarse echotechymia (12) were the most common USG findings.
DISCUSSION
A common reason for doctor consultations and hospital admissions is gastrointestinal haemorrhage.7-9 Endoscopy has been identified as the first-line diagnostic tool in upper Gastro-intestinal haemorrhage, and many therapeutic modalities have been created. Nuclear scintigraphy, mesenteric angiography and colonoscopy are methods of diagnosing lower Gastro-intestinal haemorrhage, however, a single standard procedure has not been developed since each has inherent advantages and disadvantages.10-11 In the diagnosis of inflammatory bowel disease, ischaemic colitis, bacterial colitis and malignant bowel tumours, and other bowel diseases, the sono-morphological presence of bowel wall thickening in patients with acute or chronic gut disorders has recently been assessed for its importance.12 A non-invasive and repeatable imaging analysis that can be done effectively without bowel planning is trans-abdominal ultrasonography.13-15 In our analysis we have shown the average age of the patients was 11.42 ± 6.22 Yrs. The range was from 1-60 Yrs. (The Min-Max). The majority of the patients were 52 % female and 48 %, male. Hematemesis under investigation was the most common provisional diagnosis (22 %), followed by mass per abdomen (16 %), foreign body (13 %), vomiting under investigation (11 %), fever under investigation (10 %), ascites under investigation (9 %), hypertension portal cirrhosis (6 %), upper gastrointestinal obstruction (5 %), dysphagia and dysphagia (3 %). Coarse liver eco texture (25 %), diffuse liver parenchyma (18 %), dilated portal vein with splenomegaly (10 %), dilated portal vein with per fibrosis, massive splenomegaly (10 %), hepatitis with splenomegaly (9 %), hepatomegaly with splenomegaly liver cirrhosis (6 %), hepatomegaly with splenomegaly (6 %), hepatomegaly with M gall bladder thickening(2 %), were the most common USG findings.
CONCLUSION
From our study, it can be concluded that Hematemesis under study followed by Mass per abdomen was the most common provisional diagnosis. Coarse Ecotexture of Hepatic accompanied by Diffuse Parenchymal Hepatic modifications were the most common USG findings. For diagnosis and treatment of patients, this sonographic examination along with clinical results is useful. Aggressive public education and close monitoring of patients who are found to have alcohol-related liver disorders are recommended. If life expectancy rises, caution should be taken for older adults and patients with comorbid conditions, leading to high mortality from GI bleeding.
Acknowledgement: The author acknowledges the immense help received from the scholars whose articles are cited and included in references to this manuscript. The author is also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of Interest: Nil
Source of Funding: Nil
References:
1. Rockall T, Logan RF, Devlin HB, Northfield TC. Selection of patients for early discharge or outpatient care after acute upper gastrointestinal haemorrhage. National audit of acute upper gastrointestinal haemorrhage. Lancet 1996;347:1138–1140.
2. Ghosh S, Watts D, Kinnear M. Management of gastrointestinal haemorrhage. Postgrad Med J. 2002;78(915):4–14.
3. Thomopoulos K, Vagenas KA, Vagianos CE, Margaritis VG, Blikas AP, Katsakoulis EC, et al. Changes in aetiology and clinical outcome of acute upper gastrointestinal haemorrhage during the last 15 years. Eur J Gastroenterol Hepatol 2004;16:177–82.
4. Van Leerdam ME, Vreeburg EM, Rauws EAJ, Geraedts AAM, Tijssen JGP, Reitsma JB, et al. Acute upper GI haemorrhage: Did anything change? Time trend analysis of incidence and outcome of acute upper GI haemorrhage between 1993/1994 and 2000. Am J Gastroenterol 2003;98:1494–1499.
5. Rockall T, Logan RF, Devlin HB, Northfield TC. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ 1995;311:222–226.
6. Srygley F, Gerardo CJ, Tran T, Fisher DA. Does this patient have a severe upper gastrointestinal bleed? JAMA 2012;307:1072–1079.
7. Ginn J, Ducharme J. Recurrent haemorrhage in acute upper gastrointestinal haemorrhage: Transfusion confusion. CJEM 2001;3:193–198.
8. Wardehoff D, Gros H. Endoscopic haemostasis by injection therapy in high-risk patients. Endoscopy 1982; 14: 196–9.
9. Sugawa C, Fujita Y, Ikeda T, Walt AJ. Endoscopic haemostasis of haemorrhage of the upper gastrointestinal tract by local injection of 98% dehydrated ethanol. Surg Gynecol Obstet 1986;162:159–163.
10. Panes J, Viver J, Forné M, Garcia-Olivares E, Marco C, Garau J. Controlled trial of endoscopic sclerosis in haemorrhage peptic ulcers. Lancet 1987;ii:1292–1294.
11. Shorvan P, Leung JW, Cotton PB. Preliminary clinical experience with the heat probe at endoscopy in acute upper gastrointestinal haemorrhage. Gastrointest Endosc 1985;31:364–366.
12. Zackerman G, Prakash C. Acute lower intestinal haemorrhage. I. Clinical presentation and diagnosis. Gastrointest Endosc 1998;48:606–617
13. Gostout CJ. The role of endoscopy in managing acute lower gastrointestinal haemorrhage. N Engl J Med 2000;342:125–127
14. Lim J, Ko YT, Lee DH, Lim JW, Kim TH. Sonography of inflammatory bowel disease: findings and value in the differential diagnosis. AJR Am J Roentgenol 1994;163:343–347
15. Kunihiro K, Hata J, Haruma K, Manabe N, Tanaka S, Chayama K. Sonographic detection of longitudinal ulcers in Crohn disease. Scand J Gastroenterol 2004;39:322–326.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





