IJCRR - 13(6), March, 2021
Pages: 27-32
Date of Publication: 20-Mar-2021
Print Article
Download XML Download PDF
Knowledge, Attitude and Practice Study Among Rural Antenatal Women Regarding Anaemia, Iron Rich Diet and Iron Supplement
Author: Archana Dhok, Ajay Meshram, Lata Kanyal Butola, Ruchir Khare
Category: Healthcare
Abstract:Introduction: Anaemia is one of the most common nutritional deficiency disorders affecting pregnant women; During pregnancy, the need for iron for mother and fetus gradually increases and will reach its highest level at the end of pregnancy. There should be awareness of anaemia among antenatal women and association of knowledge, attitude and practice of nutrition during pregnancy and taking iron-rich food. Objective: To assess the knowledge, attitude and practice regarding iron-rich diet and iron supplement to prevent anaemia in pregnancy in women of the rural region. Methods: The present study comprised 100 Second Trimester Pregnant Women. Pregnant women in the second trimester at�tending Gynecology and Obstetrics OPD of AVBRH, Sawangi Wardha. Data was gathered by using a structured and pretested questionnaire which asked questions on nutrition in pregnancy, anaemia and associated factors. It has three parts: Knowledge, Attitudes and Practices. Results: The knowledge level of subjects was significantly correlated with their Haemoglobin levels. There was a significant positive correlation between the Attitude scores of subjects and Haemoglobin levels.No significant positive correlation was found between Practice Scores of Subjects and Haemoglobin levels. Conclusion: Present study concludes that the studied pregnant women had good knowledge and positive attitudes but poor practice toward prevention and the prevalence of iron deficiency anaemia. To address the issue of anaemia, the health service sector needs to incorporate health promotion strategies that will positively impact the attitude and practice levels of the popula�tion.
Keywords: Pregnancy, Anaemia, Nutrition, Haemoglobin level
Full Text:
INTRODUCTION
During Pregnancy maternal nutrition and lifestyle significantly influence the health of mother and child. Maternal nutrition during conception and pregnancy influences the growth and development of the fetus and results in a healthy baby. It is usually assumed that a balanced diet is necessary for all human beings for the proper function of the body system. This indicates that nutrition is a fundamental pillar for human beings, for the health and proper development of the human being.1 It is believed that during pregnancy, it is necessary to have a properly balanced diet to make sure sufficient energy intake without the utilization of the mother’s tissues for adequate growth of the fetus to maintain pregnancy.2
Iron demand is higher in Pregnancy due to physiological changes for the development and growth of the placenta and fetus. Despite increased iron requirements, pregnancy is a period of increased risk of anaemia, which is higher than that of a non-pregnant state.3-5 According to WHO, the definition of anaemia is “a condition in which the number of red blood cells (RBCs) or their oxygen-carrying capacity is inadequate to meet the physiologic demands in the body, in which the haemoglobin level may vary by age, sex, altitude, smoking, and pregnancy status”. Anaemia in pregnancy is identified by the WHO as haemoglobin (Hb) level less than 11g/dl and is divided into three levels in terms of severity; Mild anaemia (Hb level, 9 -10.9g/dl), Moderate anaemia (Hb level, 7-8.9g/dl), and Severe anaemia (Hb level 7-4.5 g/dl).6
Anaemia is one of the most common nutritional deficiency disorders affecting pregnant women; the prevalence in developed countries is 14%, in developing countries 51%, and in India, it varies from 65% to 75%. (Feb 15, 2018) World Health Organization (WHO)/World Health Statistics data shows that 40.1% of pregnant women worldwide were anaemic in 2016.7
Anaemia is an indicator of nutritional status, which can significantly contribute to various newborn disorders like birth defects, preterm labour, and low birth weight, which can lead to a global public health problem. Nutritional iron deficiency anaemia (IDA) is the commonest (90%) cause of anaemia in pregnancy. Good nutrition is the best way to prevent iron deficiency anaemia in pregnancy as medication has its side effects. Awareness refers to the knowledge or perception of a situation or fact.8,9
Iron is essential for Fetal and placental development and to expand maternal red cell mass. The requirement of Iron in pregnancy is 27 mg/day compared to 18 mg/day in a non-pregnant state.10 If before conception, the iron levels of a woman is adequate, the physiological changes in pregnancy like cessation of menstruation, increased intestinal absorption and mobilization of reserves, would be sufficient to cover the increased demand in pregnancy. However, epidemiological data indicate that about 41.8% of pregnant women worldwide are anaemic before pregnancy and at least half of this anaemia burden is thought to be due to iron deficiency.11 In 2012 a Cochrane systematic reviewed that women taking daily iron supplements were less likely to have low birth weight babies compared to controls (RR 0.81). Thus daily iron supplementation reduced the risk of maternal anaemia at term by 70% and iron deficiency at term by 57%.12 The recent WHO guidelines recommend daily oral iron supplementation with 30-60 mg of elemental iron as part of antenatal care to reduce the risk of low birth weight, maternal anaemia and iron deficiency .13
During pregnancy, the need for iron for mother and fetus gradually increases and will reach its highest level at the end of pregnancy. The reason for this high demand is mother’s blood volume increases up to about 35%, fetus growth, placenta and other mother tissues increase the need for iron up to three to five times in the second and third trimesters. In situations of the low level of storage, this high demand could not be provided even by a diet enriched in iron and can only be partially compensated by an increase in iron absorption.14
Iron deficiency anaemia is a leading cause of maternal morbidity and mortality, prenatal infant loss; physical and cognitive losses in developing countries.15 Women with Iron deficiency anaemia are prone to an increased chance of preeclampsia and postpartum haemorrhage, and even a minimal blood loss during birth cannot be tolerated. Iron deficiency anaemia is also associated with a higher incidence of low-birth weight ,preterm birth, pre-maturity, stillbirth, and neonatal death.16 Lack of awareness is the major factor to reach millennium development goal, as the awareness of anaemia among pregnant women is only 72%. It is estimated that iron deficiency and other micronutrients are the main causes of anaemia among women of reproductive age.17 Many pregnant women suffer from a combination of malnutrition, poor weight gain and other micronutrient deficiencies, as well as infections like HIV and malaria which may lead to anaemia 18
Even though anaemia has been identified as a global public health problem for several years, no rapid progress has been observed, and that the prevalence of the disease is still high globally.19 Although there are various methods for treatment and prevention of maternal anaemia, there are still many pregnant women affected by and the contributing factors for the persistence of high incidences are not known.20 It is, therefore, very important to work out a method for the reduction and control of anaemia in women. This study focuses on the prevalence of awareness of anaemia among antenatal women and the association of knowledge, attitude and practice of nutrition during pregnancy and taking iron-rich food. Assessing nutrition-related knowledge, attitudes and practices offer an opportunity to better understand a given situation by providing insights into the social, psychological and behavioural determinants of nutritional status. Thus one of the most effective steps to reduce the prevalence of anaemia during pregnancy is health promotion through various interventions or programmes.
Studies that access and analyse people’s nutrition-related knowledge, attitudes and practices (KAP) are a useful method for gaining such an insight into peoples’ determinants of their dietary habits. It also helps for evaluating people’s nutrition-related knowledge, attitudes and practices. In the context of nutrition-related projects or programmes, a situation analysis describes the type and magnitude of nutrition issues and identifies possible causes of the nutritional problems observed. The findings of a situation analysis will help in planning a nutrition intervention aimed at alleviating the nutrition problems identified.
This study can contribute to a situation analysis by helping determine the existing knowledge, attitudes and practices relating to nutrition, which identifies nutrition education priorities.
MATERIALS AND METHODS
The present study comprised 100 Second Trimester Pregnant Women after taking proper consent from them. Pregnant women in the second trimester attending Gynecology and Obstetrics OPD of AVBRH, Sawangi Wardha are included in the study. The pilot study has been done on ten patient and found that majority of them came to ANC investigation in the early second trimester. In First-trimester iron supplementation is not given so their practice about the iron supplement in the form of tablets cannot be assessed. This study was intended to compare the haemoglobin level at the end of the third trimester after giving health promotion through various interventions or programmes depending on the result of the study. It could not be possible in the current scenario of the covid-19 pandemic as a patient was lost to follow up. Data was gathered by using a structured and pretested questionnaire which asked questions on nutrition in pregnancy, anaemia and associated factors. It has three parts as per FAO Guidelines - Macias and Glasauer 10
-
Knowledge
-
Attitudes
-
Practices
Sample Size: N=100
Inclusion criteria: Second-trimester pregnant women, Gravida status both Primigravida and multigravida.
Statistical Analysis
The data obtained was analyzed statically by computing median (Range).
Karl Pearson analysis was used to access the significance of correlation and calculate the p-value. The results were considered statistically significant p≤0.05. The obtained data in the study were tabulated using Microsoft Excel. Statistical analysis was done using Statistical Package for Social Sciences, version 20.0 software (IBM-SPSS).
RESULTS
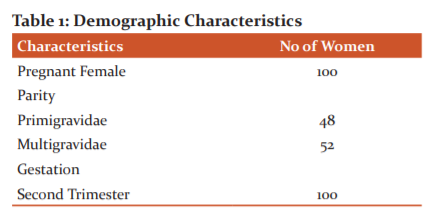
This study included a total of 100 students. Out of the 48 were primigravidae and 52 were multigravidae. All pregnant women belong to the second trimester (Table 1).
Out of 100 pregnant women included in the study, 27% were non-anaemic, 62% were mildly anaemic, 11% were mild anaemic depending on the Hb level in gm per dl ( Table 2).

A total of 100 pregnant women participates in the study, out of the majority of them heard about anaemia, Knows about symptoms and causes of anaemia. However many of them did not know about the consequences that occur during pregnancy due to anaemia. A maximum number of women Knows about ways to prevent anaemia and are aware of iron-rich foods. They are in lack knowledge regarding Iron absorption (Table 3).


Approximately 50 % of women are aware of anaemia and many of them know that it is a serious health problem. They know the importance of including iron-rich foods in their diet but are not that much aware of the preparation of iron-rich foods. Many of them feel that iron-rich foods are tasty but are not confident regarding their preparation (Table 4).


Many of them Practice Consumption of Vitamin C rich fruits, other fruits and consumption of tea/coffee regularly ( Table 5).

The knowledge level of subjects was significantly correlated with their Haemoglobin levels. This indicates that whether the subjects knew about anaemia, its symptoms, causes, consequences or dietary prevention methods, it improves their Haemoglobin levels. There was a significant positive correlation between the Attitude scores of subjects and Haemoglobin levels. This indicates that self-awareness regarding anaemia, attitude on the importance of including iron-rich foods in the diet, attitude regarding the preparation of iron-rich foods and self-confidence in preparing iron-rich foods resulted in better Hemoglobin levels. No significant positive correlation was found between Practice Scores of Subjects and Haemoglobin levels. Practices like consumption of vitamin C rich fruits, frequency of eating fruits and consumption of tea/coffee regularly etc should be incorporated for better Haemoglobin levels of subjects (Table 6).

Some finding revelled through open-ended questions
-
Most pregnant women discontinue the iron tablet due to its side effects and forgetfulness of taking tablets.
-
They are not aware of many sources of iron-rich food and their importance in the diet.
-
They are not aware of their complications
-
Wrong practice of taking iron tablets
DISCUSSION
This study provides the understandings regarding Knowledge, Attitude and Practice study among rural antenatal women regarding anaemia, iron-rich diet and iron supplement. The majority of the women had heard the term “Anaemia” and most of the women knew IFA supplements as “tablet of strength” and were unaware of the terminologies. 70% of the study participants knew about anaemia prevention through dietary measures. They mentioned some common foods in India which are sources of iron. Most of the subjects recognized the lack of iron in food as the cause of anaemia. Knowledge level and attitude scores of subjects were significantly correlated with their Haemoglobin levels. Iron deficiency anaemia is a global health problem as it ranks in the top-20 causes of disability-adjusted life years lost, It is a main cause of morbidity for women of reproductive age, but little is known about knowledge, attitudes and practices related to screening for and management of this problem. This study provides insight into the knowledge, attitude and practices regarding the prevention of IDA among pregnant women attending AVBRH Sawangi, Wardha Maharashtra. According to Allah et al. 21, the risk of IDA anaemia increased with gravidity, decreased birth spacing, gestational age, drinking tea and coffee after meals, and decreased intake of proteins and low level of knowledge and income. Increasing the efforts toward the educational interventions of women of reproductive age regarding preconception counselling and adequate intake of iron-rich food sources, iron and folic acid supplementation and early detection and treatment the anaemia before childbirth.22 Shilpa Jose et al concluded that the Knowledge level of subjects was not significantly correlated with their Haemoglobin levels but a positive correlation between the Attitude and Practice Scores of subjects and Haemoglobin levels.23 Yousuf et al found out that Pregnant women do not have sufficient knowledge related to anaemia during pregnancy. Their perception of complication of anaemia in pregnancy is also poor and attitude towards preventing and treating anaemia is also not satisfactory.24 In this study the pregnant women has knowledge and awareness about anaemia in pregnancy but their practice regarding intake of iron tablets and iron-rich food does not correlate with haemoglobin level. Thus healthy practices should be implemented by them to prevent anaemia. Raksha M, Shameem VPA their study concluded that educating antenatal women about the importance of an iron-rich diet and implementing this into practice will help in the prevention of anaemia.
CONCLUSION
The current study concluded that the studied pregnant women had good knowledge and positive attitudes but poor practice toward prevention and the prevalence of iron deficiency anaemia. To address the issue of anaemia, the health service sector needs to incorporate health promotion strategies that will positively impact the attitude and practice level of the population.
RECOMMENDATIONS
Education should include antenatal care that focuses on the intake of iron-rich foods, iron supplementation and anti-helminths. Counselling and health education are important for pregnant women with anaemia, to improve their knowledge, awareness and practice to prevent anaemia. Encourage pregnant women to practice intake iron-rich food and iron tablets during pregnancy in the proper way.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflicts of Interest -NIL
Source of Funding - NIL
References:
1. Daba G, Beyene F, Fekadu H, Garoma W. Assessment of knowledge of pregnant mothers on maternal nutrition and associated factors in GutoGidaWoreda, East Wollega Zone, Ethiopia. J Nutr Food Sci 2013;4(1):1-7.
2. Subarnalata S, Basmati P. A study of the nutritional status of pregnant women of some villages in Balasore district, Orissa. J Hum Ecol 2006;20(3):227-232.
3. Dim CC, Onah HE. Prevalence of anaemia among pregnant women at booking in Enugu, South Eastern Nigeria. Med Gen Med 2007;9(3):11- 81.
4. Noronha JA, Khasawneh EAI, Seshan V, Ramasubraman S, Raman S. Anaemia in pregnancy and challenges. J South Asian Feder. Obst Gynae 2012;4(1):64-70.
5. Tay KCS, Agboli E. Walana W. Malaria, and anaemia in pregnant and nonpregnant women of child-bearing age at the University Hospital, Kumasi, Ghana. Open J Med Microbiol 2013;3(3):193-200.
6. World Health Organization Serum Ferritin Concentrations for the Assessment of Iron Status and Iron Deficiency in Populations. Available online: http:// www.who.int/vmnis/ indicators/ serum_ferritin.pdf.
7. The global prevalence of anaemia in 2011. Geneva: World Health Organization; 2015. http://apps.who.int/iris/bitstream/10665/177094/1/9789241564960_eng.pdf.
8. World Health Organization; Global nutrition targets 2025: Anaemia policy brief.
9. Anthony SF. Harrison principle of internal medicine, 19th edition, McGraw-Hill Education 2015;625-650.
10. Italian Society of Human Nutrition. DRI of energy and nutrients for the Italian population.A summary document of the XXXV National Congress of The Italian Society of Human Nutrition. Last updated: 2012
11. WHO/CDC. Worldwide prevalence of anaemia 1993–2005.WHO Global Database on Anaemia. Geneva: World Health Organization, 2008
12. Peña-Rosas JP, De-Regil LM, Garcia-Casal MN, Dowswell T. Daily oral iron supplementation during pregnancy. Cochrane Database Syst Rev 2012;12:CD004736.
13. WHO. Guideline: Daily iron and folic acid supplementation in pregnant women. Geneva: World Health Organization, 2012.
14. Balasubramanian T, Aravazhi M, Sampath SD. Awareness of Anaemia among Pregnant Women and the Impact of Demographic Factors on their Hemoglobin Status. Int J Sci Stud 2016;3(12):303-305.
15. Okeke UP. Anaemia in pregnancy is a persisting public health problem in Porto Novo Cape Verde. J Med Sci 2011;5(4):193-199.
16. Salzberg HS. Nutrition in pregnancy. In J.J Sciarra (Ed.), Gynecology and obstetrics. Philadelphia: Lippincott Williams & Wilkins. 2002
17. Karaoglu L, Pehlivan E, Egri M, Deprem C, Gunes G, Genc MF, et al. The prevalence of nutritional anaemia in pregnancy in an east Anatolian province, Turkey. BMC Public Health 2010;10(32):329.
18. Huffman SL. Zehner E. Martin L. Mwadime R. Essential Health Sector Actions to Improve Maternal Nutrition in Africa. Essential Health Sector Actions to Improve Maternal Nutrition in Africa. The LINKAGES Project, Academy for Educational Development 29 January 2014.
19. Ouédraogo S, Koura GK, Accrombessi MM, Bodeau-Livinec F, Massougbodji A, Cot M. Maternal anaemia at first antenatal visit: prevalence and risk factors in a malaria-endemic area in Benin. Am J Trop Med Hyg 2012 Sep;87(3):418-424.
20. Margwe JA, LupinduAM. Knowledge and Attitude of Pregnant Women in Rural Tanzania on Prevention of Anaemia. Afr J Reprod Health 2018;22(3):71-79.
21. AlflahYM, Wahdan IH, Hasab AA. Taye DI, Prevalence and Determinants of Anaemia in Pregnancy, Sana’a, Yemen. Int J Public Health Sci 2017;6(3):213-220.
22. Alghamdi A. Prevalence of Anaemia among Pregnant Women in Riyadh, Saudi Arabia. International J Health Sci Res 2016;6(9):54-60.
23. Shilpa J, Sreni CA, Betty RI. Impact of Knowledge, Attitude and Practice on Anaemia status among women in coastal Kochi, Kerala. Int J Multidisci Curr Res 2016;9(3):346.
24. Shagufta Y. KAP study of mothers with anaemia in pregnancy. Int J Sci Res 2019;8(8):2277–2282.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





