IJCRR - 13(6), March, 2021
Pages: 19-22
Date of Publication: 20-Mar-2021
Print Article
Download XML Download PDF
Clinical Profile of Diagnosed Cases of Acute Pancreatitis Coming to a Tertiary Care Hospital
Author: Rahul Ranjan, Sharaddendu Bali, Tushar Parmeshwar, Akhilesh Yadav
Category: Healthcare
Abstract:Introduction: Pancreatitis is a condition in which inflammation of the pancreas occurs. When the digestive enzymes are trig�gered until they are released into the small intestine and start assaulting the pancreas, pancreatic damage occurs. Pancreatitis is associated with exocrine and endocrine (sometimes) parenchyma damage, resulting in clinical manifestations ranging in severity from a mild, self-limited illness to an acute inflammatory phase that threatens life. Objective: To study the clinical profile of Diagnosed cases of Acute Pancreatitis coming to a tertiary care hospital. Methods: Diagnosed cases of Acute Pancreatitis coming to our hospital. A total of 50 consecutive cases fulfilling the eligibil�ity criteria were taken for study after informed consent. Results: Mean age of the study cases was 41.56 years with over half of the cases (52%) were between 21-40 years of age. Male predominance was seen among study cases. The most common symptoms among presenting cases were a pain in the abdomen (100%) and vomiting (76%). The most common aetiology for pancreatitis among study cases was alcohol. Good outcome was seen in 46% of cases while the mortality rate was 2%. Mean hospital stay among study cases ranges from 1-30 days with a mean stay of 10.2 days. Conclusion: Identification of patients at risk for mortality early in the course of acute pancreatitis is an important step in improv�ing outcome.
Keywords: Acute pancreatitis, Pain in abdomen, Alcohol
Full Text:
Introduction
The pancreas is a major gland situated behind the stomach and next to the small intestine. It releases powerful digestive enzymes into the small intestine to aid food digestion. There are two main things the pancreas does. It stimulates the hormones insulin and glucagon in the bloodstream, too. These hormones allow the body to monitor the way food is used for energy.1 Pancreatitis is a disease where the pancreas is inflamed. Pancreatic damage occurs when digestive enzymes are stimulated before they are released into the small intestine and begin targeting the pancreas. Exocrine and endocrine (sometimes) parenchymal injury are correlated with pancreatitis, resulting in clinical manifestations varying in intensity from a mild, self-limited disease to a life-threatening acute inflammatory phase, which may range in duration from a temporary assault to a permanent pancreatic function loss. Pancreas inflammatory disease can be known as acute or chronic pancreatitis.2,3 A sudden inflammation that persists for a brief period is acute pancreatitis. It can range from moderate pain to a serious, life-threatening illness. Chronic pancreatitis is an inflammation of the pancreas that is long-lasting. It most commonly occurs after an acute pancreatitis episode.4,5 The aetiology of pancreatitis varies according to geographical location, but alcohol, gallstones, metabolic factors and medications are most frequently involved. By both clinical and routine radiological approaches, the pancreas is a hard organ to test. The inflammatory pathology involving the pancreas may be included in the differential diagnosis of other abdominal pain disorders. In most patients, the combination of sufficient clinical results and laboratory testing allows for a correct diagnosis of acute pancreatitis. On the other hand, chronic pancreatitis forms a far more complicated clinically or biochemically assessable entity.6
Material AND methods
This is a Prospective, observational, Clinical study on Diagnosed cases of Acute Pancreatitis coming to our hospital. A total of 50 consecutive cases fulfilling the eligibility criteria were taken for study after informed consent. Valid informed consent was taken from patients or patients relatives to be included in the Study. The clinical, laboratory and radiological data were collected from each patient diagnosed with acute pancreatitis within 24 hours of presentation.
Inclusion Criteria: All adults (> 18 years) of both genders. Cases of acute pancreatitis with raised serum lipase/ amylase levels and confirmed on USG/ CT scan.
Exclusion Criteria: Pancreatitis with gut perforation & Pancreatitis in pregnancy.
Results
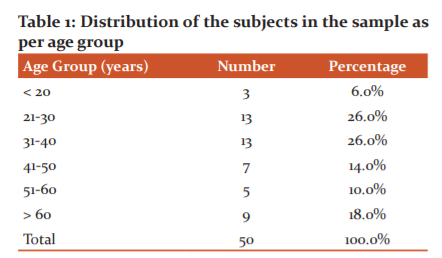
Mean age of the study cases was 41.56 years with over half of the cases (52%) were between 21-40 years of age.
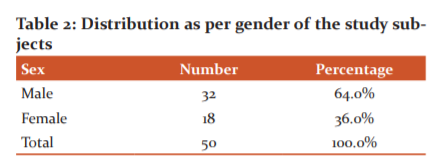
Male predominance was seen among study cases with 64% males to 36% females.
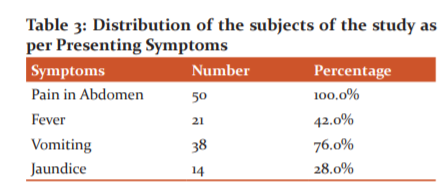
Most common symptoms among presenting cases was pain in abdomen (100%) and vomiting (76%). Other symptoms include fever (42%) and jaundice (28%).
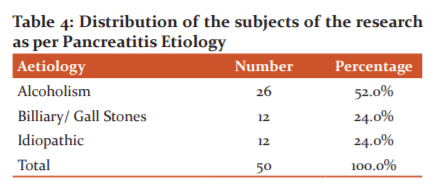
The most common aetiology for pancreatitis among study cases was alcohol (52%) followed by biliary calculi (24%) and idiopathic (24%).
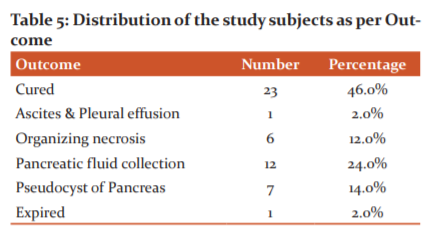
Good outcome was seen in 46% of cases while mortality rate was 2%. Associated complications include pancreatic fluid collection (24%), pancreatic pseudocyst (14%), organizing necrosis (12%) and ascites/ pleural effusion (2%).
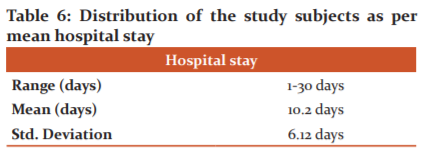
Mean hospital stay among study cases ranges from 1-30 days with a mean stay of 10.2 days.
Discussion
The mean age of the study cases was 41.56 years with over half of the cases (52%) were between 21-40 years of age. The findings show that pancreatitis occurs in relatively younger adults. Male predominance was seen among study cases with 64% males to 36% females with male to female ratio as 1.78:1. In a similar study by Shakeel et al,7 mean age of study subjects was 37.4 years with the highest patients in the age group of 20 – 39 years (51%) followed by 40 – 59 years (36%). Males constituted 80% and females 20%. In another study on acute pancreatitis by Prasad et al,8 out of 40 patients, 22 were males and 18 were females. The majority of patients were in the age group of 21-40 (57.5%). The study by Negi N et al9 included 89 (72.35%) male and 34 (27.65%) female patients with a male to female ratio were 2.6:1. The age of patients ranged between 18 to 81 years. The mean age was 42.89 ±12.53 years. The result observed in the present study and that by other authors showed that pancreatitis mainly affects younger adults with the male being affected more than females. The gender bias can be attributed to the aetiology of the pancreas i.e. alcohol which is consumed predominantly by males in the Indian community. In the present study, the most common symptoms among presenting cases were a pain in the abdomen (100%) and vomiting (76%). Other symptoms include fever (42%) and jaundice (28%). Although pain in the abdomen is the most common symptom of pancreatitis, no specific features easily distinguish pain caused by pancreatitis, from that caused by other abdominal conditions. In a study by Shakeel MD et al, abdominal pain was the presenting symptom in all the patients with acute and acute chronic pancreatitis. Our results also correlate with a study conducted by Lee MG et al10 in which 30 (86%) patients out of 35 cases had abdominal pain. Also in this study 16 out of 31 chronic pancreatitis patients did not have pain. In another study by Prasad et al, all the patients with acute pancreatitis presented with pain abdomen, 80% of them presented with nausea/ vomiting, 42.5% of them presented with fever and 30 % of them with jaundice. The most common aetiology for pancreatitis among study cases was alcohol (52%) followed by biliary calculi (24%) and idiopathic (24%).
In a study by Prasad et al, the most common aetiology observed among male cases of acute pancreatitis was alcoholism (50%) while in female cases was biliary pathology (72%). In Negi et al, the major etiological groups for cases of acute pancreatitis were: alcohol 73 cases (59.3%) and gallstones, (35.6%). Panda et al10 in their study observed alcohol as the most common aetiology (54.84%) followed by idiopathic cases (48.39%). Good outcome was seen in 46% of cases while the mortality rate was 2%. Associated complications include pancreatic fluid collection (24%), pancreatic pseudocyst (14%), organizing necrosis (12%) and ascites/ pleural effusion (2%). Persistent organ failure > 48 hours i.e. severe acute pancreatitis (SAP) was seen in 8 cases (16%). Macherla R et al11 in their study observed complications in acute pancreatitis as the pancreatic fluid collection (20%), organizing necrosis (14%) and ascites/ pleural effusion (6%). Severe acute pancreatitis was seen in 8 cases (20%). Yadav J et al12 in their study observed the following complications: pancreatic pseudocyst (27.7%), organizing necrosis (39.5%) and severe acute pancreatitis (35.2%). Incidence of severe acute pancreatitis as 19.8% and 23% respectively in previous studies.13,14 The mortality rate in the study by Negi et al was 5.7% while in the study by Bota S et al the mortality rate was 4.6%. Mortality rates observed in the previous studies was also in the range of 6-15%.
Conclusion
Identification of patients at risk for mortality early in the course of acute pancreatitis is an important step in improving outcome. The mean age of the study cases was 41.56 years with over half of the cases (52%) were between 21-40 years of age. Male predominance was seen among study cases with 64% males to 36% females. The most common symptoms among presenting cases were a pain in the abdomen (100%) and vomiting (76%). The most common aetiology for pancreatitis among study cases was alcohol (52%) followed by biliary calculi (24%) and idiopathic (24%). Good outcome was seen in 46% of cases while the mortality rate was 2%. Mean hospital stay among study cases ranges from 1-30 days with a mean stay of 10.2 days.
Acknowledgement
The author acknowledges the immense help received from the scholars whose articles are cited and included in references to this manuscript. The author is also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of Interest: Nil
Source of Funding: Nil
References:
-
Deng Y, Wang R, Wu H, Tang CW, Chen XZ. Aetiology, clinical features and management of acute recurrent pancreatitis. J Dig Dis 2014;15(10):570-577.
-
Ranson J, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet 1974;139(1):69-81.
-
Knaus W, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985 Oct; 13(10):818-29.
-
Balthazar E, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: the value of CT in establishing prognosis. Radiology 1990 Feb; 174(2):331-6.
-
Bota S, Sporea I, Sirli R, Popescu L, Strain M, Focsa M. Predictive factors for severe evolution in acute pancreatitis and a new score for predicting a severe outcome. Ann Gastroenterol 2013;26(2):156-162.
-
Khanna A, Meher S, Prakash S, Tiwary SK, Singh U, Srivastava A, et al. Comparison of Ranson, Glasgow, MOSS, SIRS, BISAP, APACHE-II, CTSI Scores, IL-6, CRP, and procalcitonin in predicting severity, organ failure, pancreatic necrosis, and mortality in acute pancreatitis. HPB Surgery 2013;2013:367581.
-
Shakeel M, Irfan SS. Clinical profile of patients with pancreatitis. Int Surg J 2017;4(2):534-537.
-
Prasad HL, Nagarjuna TL. Clinical profile of patients with Acute pancreatitis. Int Surg J 2016;4(7):2994-2997.
-
Negi N, Mokta J, Sharma B, Sharma R, Jhobta A, Bodh V. Clinical Profile and Outcome of Acute Pancreatitis: A Hospital-Based Prospective Observational Study in Subhimalayan State. J Assoc Physicians India 2018 Mar;66(3):22-24.
-
Panda C, Misra B, Behera SK, Das HS, Singh SP. A Study on Changing Clinical Profile of Chronic Pancreatitis from a Tertiary Care Centre. Int J Sci Study 2017;5(4):170-173.
-
Macherla R, Swathi GA comparative evaluation of bisap, apache ii and ctsi scoring systems in the early prediction of severity in acute pancreatitis. J Evidence-Based Med Healthcare 2016;3(94):5190-5196.
-
Yadav J, Yadav SK, Kumar S, Baxla RG, Sinha DK, Bodra P. Predicting morbidity and mortality in acute pancreatitis in an Indian population: a comparative study of the BISAP score, Ranson’s score and CT severity index. Gastroenterol Rep 2015;4(3):216-220.
-
Zheng L, Hong W, Geng W, Stock S, Pan J. A comparison of the BISAP score and Amylase and BMI (CAB) score versus for predicting severe acute pancreatitis. Acta Gastroenterol Belg 2019;82(3):397-400.
-
Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology. 2002;223(3):603-613.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





