IJCRR - 13(5), March, 2021
Pages: 121-125
Date of Publication: 03-Mar-2021
Print Article
Download XML Download PDF
Steam Inhalation as an Adjuvant Treatment in Covid-19 Positive Health Care Professionals: Our Experiences at Tertiary Care Teaching Hospital
Author: Santosh Kumar Swain, Ansuman Sahu
Category: Healthcare
Abstract:Introduction: Steam inhalations are often used for the treatment of the viral infections of the respiratory tract such as common cold or croup. Objective: This study was aimed to evaluate the effect of the steam inhalation on COVID-19 infection. Methods: This is a prospective and descriptive study. The participants of this study were COVID-19 positive health care professionals and divided into two groups such as Group-A and Group-B. Group-A included 52 asymptomatic COVID-19 patients whereas Group-B included 44 symptomatic COVID-19 patients. The steam with a temperature of 42 0C to 45 0C was inhaled by all of Group-A and Group-B patients. Results: There were 52 asymptomatic COVID-19 patients in Group-A where 34 male and 18 female patients with a male to female ratio was 1.8:1. Out of the 44 symptomatic COVID-19 patients, 28 male and 16 female with male to female ratio was 1.75:1 The age ranges of the participant patients were 22 years to 68 years with a mean age of 38\?16 years. All the mild and moderate symptomatic patients except one became symptom-free by one week use of steam inhalation. Conclusions: The symptoms of the COVID-19 patients were drastically reduced after use of the steam inhalation. The favourable effect of the steam inhalation for reducing the symptoms of the COVID-19 infections is to decrease the severity and duration of this infection and it also justifies its therapeutic application and acts as a ray of hope in this dreaded pandemic.
Keywords: COVID-19 infection, SARS-CoV-2, steam inhalation, CO-RADS
Full Text:
INTRODUCTION
Coronavirus disease 2019(COVID-19) is caused by a novel virus called severe acute respiratory coronavirus 2(SARS-CoV-2).1 Rapid transmission of the SARS-CoV-2 leads to COVID-19 pandemic. The route for the entrance of the SARS-CoV-2 is usually through the nose, mouth and eyes. The common clinical manifestations of the COVID-19 patients are fever, dry cough, fatigue, dyspnea, decreased taste and smell sensation. Some COVID-19 patients are asymptomatic but act as silent carriers of this infection.2 Currently medical authorities are emphasizing the preventive strategies such as the use of face mask, social distancing and hand washing. Till now there is no effective treatment protocol for curing the COVID-19 infections. In traditional home remedy, steam inhalation has been used as adjuvant treatment in several respiratory conditions such as common colds, croup and bronchitis.3 The use of the steam inhalation is based on their heat and humidity of warm and moist air. Steam inhalation has been used for centuries for the treatment of Influenza virus or common flu. SARS-CoV-2 is structurally similar to the influenza virus. Previous studies on the influenza virus and coronavirus show strong support towards the effect of the steam inhalation. The rationale behind the use of steam inhalation in common colds was the reduced replication of the human rhinovirus (common aetiology of the common cold) in vitro at the temperature of 33 to 43 0C.4 Humidity is also functioned as secretolytic in case of bronchiolitis.5 In case of croup, steam inhalation soothe inflamed mucosa of the laryngeal surface, reduce the viscosity of mucus and make easy airflow.6 The effect of the heat or steam inhalation on the novel SARS-CoV-2 in contrast to the rhinovirus has been less established. This study aims to evaluate the effect of steam inhalation as an adjuvant treatment among health care professionals with COVID-19 infections. Inhalation of humidified warm air has long been r an effective means of alleviating cold
MATERIALS AND METHODS
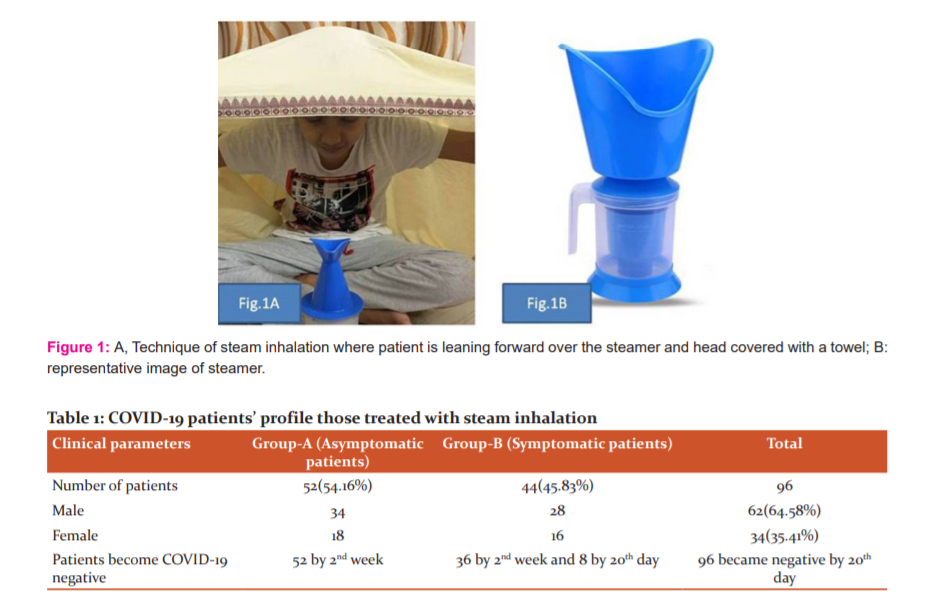
This is a prospective and descriptive study done among the COVID-19 positive health care professionals such as doctor, staff nurse and health care workers in a tertiary care teaching hospital. All these patients were diagnosed based on the reverse transcription-polymerase chain reaction (RT-PCR) and computed tomography (CT) of the thorax. This study was conducted between April 2020 to September 2020. This study was approved by the Institutional Ethical Committee (IEC) with reference number IEC/IMS/SOAU/23/2020. The steam with a temperature of 42 0C to 45 0C was inhaled. All the patients were using ordinary steamer available in the market for steam inhalation (Figure 1). Different variables were obtained before and after steam inhalation was compared. The study participants were divided into two groups: Group A and Group B. Group A was consisting of 52 asymptomatic COVID-19 positive health care professionals. These asymptomatic patients were advised for inhaling steam thrice daily for two weeks by ordinary steamer available in the market and the duration of each inhalation was 5 minutes. Group-B was consisting of 44 symptomatic COVID-19 health care professionals and symptoms were ranging from mild to moderate symptoms. Mild symptoms include only nasal or throat symptoms and moderate symptoms include both nasal and throat symptoms along with more other symptoms. Severe symptoms include dyspnea requiring oxygen or ventilation along with nasal and throat symptoms. In this study patients with severe symptoms were excluded. We also analyzed the CO-RADS score from the CT scan of the thorax of the study patients. CO-RADS score varies from CO-RADS 1 to CO-RADS 5. CO-RADS 6 score indicates proven COVID-19 involvement which supported by RT-PCR test. Each of the five lung lobes in CT thorax were assessed for degree of involvement and classified as none (0%), minimal (1-25%), mild (26-50%), moderate (51-75%), and severe (76-100%). No involvement to a lobe score of 0, minimal to a lobe score of 1, mild to a lobe score of 2, moderate to a lobe score of 3 and severe to a lobe score of 4. The total scores of the five lobes of lungs range from 0 to 20. All these mild to moderate symptomatic patients were advised to take steam inhalation every three hours and each inhalation for 5 minutes along with COVID-19 treatment in the COVID hospital. All the 52 the asymptomatic patients were taking Tab. Zinc, Tab. Vitamin-C, Tab. Vitamin-D3(60K once weekly), Tab. Famotidine (20 mg) twice daily and in mild to moderate symptomatic patients were taking Tab. Azithromycin, Tab. Paracetamol, Tab. Vitamin-C, Tab. Vitamin-D3 and Vitamin Zinc. All of these asymptomatic and mild to moderate symptomatic patients were taking steam inhalation along with the above treatment. Group A was consisting of 52 asymptomatic COVID-19 patients and Group-B consisting of 44 symptomatic COVID-19 patients and all of them under observation for any improvement at the follow-up visit at the 1st week, 2nd weeks, one month and 2 months. In this study, all the data were recorded and analyzed by using Statistical Package for Social Science (SPSS) software, v25(IBM, Armonk, New York, USA).
RESULTS
There were 52 asymptomatic and 44 symptomatic COVID-19 patients. The age ranges of the patients were 22 years to 68 years with a mean age of 38±16 years. There were 62 males and 34 females in this study. The male to female ratio of the participants in this study was 1.8:1. There were 52 asymptomatic COVID-19 in Group-A where 34 male and 18 female patients with a male to female ratio was 1.8:1. In Group-B, out of the 44 symptomatic COVID-19 patients, 28 male and 16 females with male to female ratio was 1.75:1 (Table 1). All the patients were treated with steam inhalation with follow up visit at 1st week, 2nd weeks, one month and two months. Out of the 52 asymptomatic patients, 48 (92.30%) were symptom-free as before at the follow-up visit at 2 weeks, one month and two months whereas 4 patients (7.69%) developed mild symptoms at the first week follow up visit. All these 52 patients became negative for COVID-19 infection during the second weeks with reverse transcription-polymerase chain reaction (RT-PCR) test. In Group-B, there were 44 symptomatic. Out of the 44 symptomatic, 36 were mild symptomatic and 8 were moderate symptomatic. All the mild symptomatic COVID-19 patients became symptom-free in 5 days with steam inhalation whereas in moderate symptomatic patients (except one patient), all of them became symptom-free after 7 days. One moderate symptomatic patient has developed pneumonia followed by orotracheal intubation and this patient extubated at the COVID intensive care unit (ICU) and discharged for home quarantine. The COVID-19 test (RT-PCR) was done in all cases after 10days of the treatment and found negative in 84 cases (87.50%) out of the 96 positive cases. By the second week, all patients of Group-A return to negative after 14 days of treatment. In Group-B, 8 COVID-19 tests came to negative in 20 days. The CO-RADS score was 6 in all cases because of the positive RT-PCR before steam inhalation. The involvements of the lobes of lungs in the CT scan of the thorax were analyzed before and after steam inhalation (Table 2). The entire Group-A and Group-B patients those were using the steam inhalation recovered and became negative for COVID-19. No death occurred from this study patients.
DISCUSSION
The COVID-19 infection is a highly contagious disease which spread rapidly from human to human via droplets. The initial COVID-19 case with pneumonia due to novel coronavirus SARS-CoV-2 manifesting COVID-19 was found in Wuhan, Hubei Province, China in December 2019.7 Then these infections were transmitted from human to human and lead to a pandemic with disastrous manifestations all over the world. The transmission of the SARS-CoV-2 usually occurs through the upper respiratory tract such as the nose, nasopharynx, oral cavity, pharynx and larynx with high levels of viral shedding.7 It typically spreads via droplets but the aerosols generating procedures are more responsible for the transmission of the virus among health care professionals and enhance the spread to the surrounding persons.8 So, health care workers are an important person to stay away from the infections otherwise the health care service will be stopped once they become infected.9 In this study, the focus was on the health care workers as they are more vulnerable and challenge to the health care delivery system of a hospital. Symptomatic or asymptomatic patients of COVID-19 infections are responsible for spreading the disease in approximately 79% of the documented cases.10 The transmission of the COVID-19 occurs because the shedding of the SARS-CoV-2 virus begins before the onset of the symptoms.11 A significant number of COVID-19 patients do not present with symptoms. In this study, out of the 96 COVID-19 positive participating patients, 52 were with no symptoms and 44 were symptomatic. All of them treated with steam inhalation. Steam inhalation has been used as home remedies for relieving the nasal obstruction in patients with allergic rhinitis and the common cold. Inhalation of humid and hot air enhances the temperature of the nasal mucosa, leading to inhibition of the chemical secretion from the mast cells in allergic rhinitis or the common cold.12 One study showed that histamine level in the nasal mucosa significantly reduced after steam inhalation, causing decreased nasal obstruction and vascular leakage.13 So, steam inhalation is helpful for quick relieve of the cold symptoms by reducing the respiratory virus such as rhinovirus or coronavirus.14 It also lowers the inflammatory process and immunological responses by viral infections of the respiratory tract specifically upper airway. Steam inhalation surely relieves nasal symptoms such as nasal block, itching, sneezing, running nose, postnasal drip, facial pain and headache in COVID-19 patients. In this study, 44 patients (Group-B) were COVID-19 positive with mild to moderate symptoms. Mild symptoms include only nasal or throat symptoms whereas moderate symptoms include both nasal and throat manifestations.
All of our patients in this study were diagnosed with RT-PCR test. There are certain investigations are used for diagnosis of the COVID-19 infection such as RT-PCR, rapid antigen test and computed tomography (CT) scan of the thorax. The CT thorax is high sensitivity and specificity for an immediate result.15 CT scan of the lungs shows infiltrates, ground-glass opacities and segmental consolidation. CT picture is also abnormal in asymptomatic COVID-19 positive cases. So, CT scan is also useful for diagnosis of the COVID-19 suspected patients with a negative report, however, these patients may show positive molecular tests report on a repeat test.16 COVID-19 reporting and data system (CO-RADS) is a categorical evaluation scheme for pulmonary involvement in COVID-19 infections at an un-enhanced chest CT which performs well for predicting the COVID-19 patients.15 It assesses the pulmonary involvement in COVID-19 infection on a scale from 1 (very low) to 5 (very high). There are two additional categories respectively encode a technically insufficient examination (CO-RADS 0) and RT-PCR positive for SARS-CoV-2 infection at the time of examination (CO-RADS 6). In this study, CO-RADS score varies from CO-RADS 0 to CO-RADS 5. CO-RADS 6 score indicates proven COVID-19 involvement which supported by RT-PCR test. In this study, the asymptomatic patients were showing the score of 0 to 5 in CT thorax before steam inhalation and became to 0 after steam inhalation. The negative tested COVID-19 may not accurate. Patients should be screened for respiratory symptoms and fever before performing the laryngeal and trachea-bronchial examinations and surgical procedures. Clinical should obtain the COVID-19 test report (RT-PCR) although it has a significant false-negative rate.17
One infected patient of COVID-19 infects an average of three new persons, the reproductive number (R0) being 3 for SARS-CoV-2.18 As this is a novel viral infection of the human being, antiviral drugs and vaccinations are not yet been developed for this rapidly spreading illness. So, currently, the major emphasis is given on hand wash, social distancing and use of the face mask.19 Steam inhalations with humidified warm air is usually regarded as an effective tool for alleviating the cold symptoms. Increasing the intranasal temperature is reportedly effective for decreasing the nasal resistance whereas the exposure of the cold air to the nasal mucosa increases the nasal cavity resistance. High temperature inside the nasal cavity is also helpful to minimize the infectivity of the rhinoviruses. Rhinoviruses are an important group of cold viruses causing respiratory tract infections. The steam inhalation is one of the widely used home remedies for soothing and opening the nasal passages. There are several studies regarding the effect of the different temperature on the virus. On smooth surfaces, the dried virus retains its viability for over five days at a temperature of 22 to 25 0C and relative humidity of 40 to 50% that is typical air-conditioned environments.20 Steam inhalation has a temperature of about 70 0C to 80 0C which is above the instability temperature for the SARS-CoV-2. The study of the influenza virus on human and Guinea pigs showed a similar pattern and the majority of the influenza virus were inactivated above the temperature of the 30 0C.21
One study documented that incubating the SARS-CoV-2 at the temperature of 70 0C make inactivation from 14 days to 5 minutes.22 So, it implies that the higher temperature of the steam may be useful for COVID-19 infection. Effects of steam inhalation on other respiratory infections may give indirect evidence for effectiveness on the COVID-19. Steam inhalation must be differentiated from the cool mist therapy. The cool mist therapy is preferentially used in hospital and developed countries because of its relative uniformity and safety of the delivery.5 Cool veils of mist may help similarly in case of croup by reducing the viscosity of the secretions and mucosal oedema.23 Usually cool mist has been provided via hospital beds or tents whereas steam inhalation is a home-based practice. In home-based practice, steam inhalation is frequently used for minor respiratory complaints. There are several techniques available and some are traditional such as boiling a kettle, staying in a sauna and leaning over a bowl of boiling water or running a hot water shower whereas some utilize the specialized devices like delivering steam via nozzles or nasal cannula. Some devices produce steam at 41 to 47 0C while sauna temperature may attend 80 to 95 0C.24 The practice of tu-ob(leaning over a bowl of boiling water) in the Philippines got the attention of medical specialties about its therapeutic effects of COVID-19 infections.25
Steam inhalation may be hazardous to pediatric age patients and should be done carefully. Steam inhalation may result in scalds and even require hospitalization for these complications and disfigurement. In this study, no patients were affected by any complications like scalds. However, the steam inhalation improves the ciliary function, so helps in mucociliary clearance, decongestion enhances the breathing and reduce the cough.26 Steam inhalation is one of the effective adjuvant treatments in asymptomatic and symptomatic COVID-19 patients. It usually relieves the respiratory symptoms and helps to the speedy recovery of the COVID-19 patients. Steam inhalation is one of the effective adjuvant treatments for COVID-19 infections.
This is an observational study on small size population. It warrants an extended randomized control trial for evaluating the effect of steam inhalation on a larger size population of patients and health care professionals. Further confirmation can be done by the study of a larger scale in Asian and Western populations.
CONCLUSIONS
The clinical symptoms in COVID-19 patients are dramatically reduced by administration of steam inhalation. Steam inhalation can be used as an adjuvant treatment along with the use of face masks, social distancing and hand wash with sanitisers for prevention and treatment of the COVID-19 infection. Steam inhalation is an easily available technique and affordable addition to the treatment for COVID-19 infections which curb the severity of the infections and transmission of the SARS-CoV-2. As we await a definitive treatment to fight this pandemic, steam inhalation currently a safe technique will act as a ray of hope in the treatment of the COVID-19 infection.
Author Contribution: SKS: Concept, data collection and data analysis; AS: Data collection, data analysis, and drafting the manuscript.
Conflict of interest: Nil
Funding: No Funding sources were granted or used specifically for this work.
References:
1. Swain SK, Behera IC. Managing pediatric otorhinolaryngology patients in coronavirus disease-19 pandemic-A real challenging to the clinicians. Indian J Child Health 2020;7(9):357-362.
2. Swain SK, Agrawal R. Mastoid surgery: a high-risk aerosol-generating surgical procedure in COVID-19 pandemic. Int J Otorhinolar Head Neck Surg 2020;6(10):1941-1946.
3. Vathanophas V, Pattamakajonpong P, Assanasen P, Suwanwech T. The effect of steam inhalation on nasal obstruction in patients with allergic rhinitis. Asian Pac J Allergy Immunol 2019. doi: 10.12932/AP-090818-0393. Online ahead of print.
4. Sahin O, Gülen F. Approach to the common cold in children. J Ped Res 2015;2(1):1-6.
5. Umoren R, Odey F, Meremikwu MM. Steam inhalation or humidified oxygen for acute bronchiolitis in children up to three years of age. Cochrane Database Syst Rev 2011;(1): CD006435.
6. Szilagyi PG. Humidifiers and other symptomatic therapy for children with respiratory tract infections. Pediatr Infect Dis J 1991;10(6):478-479.
7. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of Novel Coronavirus-infected pneumonia. N Engl J Med 2020:382;1199-1220.
8. Tran K, Cimon K, Severn M, et al. Aerosol generating procedures and risk of transmission of acute respiratory infections tohealthcare workers: a systematic review. PLoS One. 2012;7(4):e35797.
9. Swain SK, Das S, Padhy RN. Performing tracheostomy in intensive care unit-A challenge during COVID-19 pandemic. Siriraj Med J 2020;72(5):436-442.
10. Li R, Pei S, Chen B, et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020;368(6490):489-493.
11. He X, Lau EH, Wu P, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature Med 2020;26(5):672-675.
12. Ophir D, Elad Y, Dolev Z, et al. Effects of inhaled humidified warm air on nasal patency and nasal symptoms in allergic rhinitis. Ann Allergy 1988;60:239-242.
13. Salman SD, Proctor DF, Swift DL, et al. resistance: description of a method and effect of temperature and humidity changes. Ann Otol Rhinol Laryngol 1971;80:736-743.
14. Rouadi P, Baroody FM, Abbott D, et al. A technique to measure the ability of the human nose to warm and humidify the air. J Appl Phys 1999;87(1):400-406.
15. Levine R, Caputo N. CT scan of a COVID positive patient. J Am Coll Emerg Physic 2020; 18(6):123-128.
16. Huang P, Liu T, Huang L, et al. Use of chest CT in combination with negative RT-PCR assay for the 2019 novel coronavirus but high clinical suspicion. Radiology 2020; 295(1):22-23.
17. Yu P, Zhu J, Zhang Z, Han Y. A familial cluster of infection associated with the 2019 novel coronavirus indicating possible person-to-person transmission during the incubation period. J Infect Dis 2020;221(11):1757-1561.
18. Guo YR, Cao QD, Hong ZS, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Military Med Res 2020;7(1):1-10.
19. Swain SK, Acharya S, Sahajan N. Otorhinolaryngological manifestations in COVID-19 infections: An early indicator for isolating the positive cases. J Sci Soc 2020;47(2):63.
20. Chan KHI, Peiris JS, Lam SY, et al. The effects of temperature and relative humidity on the viability of the SARS coronavirus. Adv Virol 2011;2011:734690.
21. Lowen AC, Mubareka S, Steel J. Influenza virus transmission is dependent on relative humidity and temperature. PLoS Pathog 2007;3(10):1470-1476.
22. Chin A, Chu J, Perera M, et al. Stability of SARS-CoV-2 in different environmental conditions. Med Rxiv 2020;1:10.
23. Knutson D, Aring A. Viral croup. Am Fam Physic 2004;69 (3):535-540.
24.Pach D, Knöchel B, Lüdtke R. Visiting a sauna: does inhaling hot dry air reduce common cold symptoms? A randomised controlled trial. Med J Aus 2010;193(11-12):730-734.
25. Uy TM, Miranda MC, Aro SJ, et al. Should steam inhalation be used in the treatment and prevention of COVID-19? Asia Pac Center Evid Based Health Care 2020;1:1-6.
26.Fehr AR, Perlman S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol Biol 2015; 1282:1-23.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





