IJCRR - 13(4), February, 2021
Pages: 157-161
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
Acceptability of Different Behaviour Management Techniques in Paediatric Dentistry: A Study of Chinese, Indian and Malay Parents
Author: Md Toufiqur Rahman, Aimi Kamarudin, Sumaiya Zabin Eusufzai, Noraida Mamat, Ahmad Shuhud Irfani bin Zakaria, Mohmed Isaqali Karobari
Category: Healthcare
Abstract:Introduction: Uncooperative behaviours of Paediatric patients disrupt the quality of the treatment rendered, thereby increasing the treatment time, triggering restlessness amongst the young patients and in some instances increase risk of accidental injury. Objective: To assess the parental acceptance of different behaviour management techniques (BMTs) used during the dental treatment of children in three major ethnic groups (Chinese, Malay, and Indian) in Malaysia. Methods: A total of 72 parents were included in the study, further divided 3 groups depending on ethnicity. Two university hospitals within Malaysia were chosen for data collection in the years 2019 and 2020. A videotape was used according to American Academy of Paediatric Dentistry (AAPD) derived BMTs to showcase consenting parents ten of the AAPD approved BMTs in the following order: Tell Show Do, Voice Control, Modelling, Action Restraints, Distraction, Parents Present or Absent (PP/A), Hand Over Mouth (HOM), Nitrox Oxide (NO), Oral sedation (OS) and General Anaesthesia (GA). The parents were asked by a coordinator to mark on the scale. Results: Statistical analysis of individual BMTs revealed a significant difference in the three ethnicities (P=.05) with all other techniques remaining unremarkable when compared in the three groups. Conclusions: Tell-show-do, distraction and modelling parental presence/absence and reinforcements have been shown to produce similarly acceptable results amongst. Physical restraint, oral sedation and general anaesthesia were the least approved in the current study.
Keywords: Behavior management techniques, Dental treatment, Paediatric dentistry, Ethnic groups, Chinese, Malay, Indian
Full Text:
Introduction
Paediatric dentists reported that 13% of all children demonstrate reluctance as patients while 11% act negatively.1 Such uncooperative behaviours disrupt the quality of the treatment rendered, thereby increasing the treatment time, triggering restlessness amongst the young patients and in some instances increase risk of accidental injury. Such reluctant and uncooperative patients are often managed by various pharmacological (sedation and anaesthesia) and non-pharmacological Behaviour Management Techniques (BMT). Most commonly used techniques according to the American Academy of Paediatric Dentistry (AAPD) include positive pre-visit imagery, direct observation, tell-show-do (TSD), ask-tell-ask, voice control, modelling, positive reinforcement and descriptive praise, distraction, parental presence/absence, and advanced behaviour guidance techniques, such as protective stabilization, sedation, the controversial ‘hand-over-mouth’ technique and general anaesthesia.2
Most of the widely available methods require the parents and legal guardians to approve of the means, which is affected by a multitude of socioeconomic, racial, philosophical, cultural, and geographic factors. 3, 4 While there have been studies evaluating parental acceptance to such techniques in the Western world no such evaluations have been made as of now within the Asian sphere. Therefore, the current study aimed to evaluate the parental acceptance to various BMTs when the study was subjected to three of the major ethnic groups of Asia; Chinese, Indian and Malay. The null hypothesis was formulated that there will be no significant differences in parental acceptance of different BMTs when assessing the three ethnic groups.
Materials and Methods
Two university hospitals within Malaysia were chosen for data collection in the years 2019 and 2020. Only parents of the three ethnicities educated in written and spoken English have considered whose children were under the age of 18. Children with special disabilities were excluded. Seventy-two parents were conveniently considered with 22 in each of the 3 groups. Ethical approval for the study was obtained from Jawatankuasa Etika Penyelidikan Manusia (JEPeM) of USM (USM/JEPeM/19070410).
A videotape was made according to AAPD derived BMTs to showcase consenting parents ten of the AAPD approved BMTs in the following order: Tell-Show-Do (TSD), Voice Control (VC), Modelling, Action Restraints, Distraction, Parents Present or Absent (PP/A), Hand Over Mouth (HOM), Nitrox Oxide (NO), Oral sedation (OS) and General Anaesthesia (GA). The video was 10 minutes in duration, after which the parents were asked to express their level of agreement to each method using a 100-point visual analogue scale (VAS). The left end of the scale read “completely acceptable” and the right end of the scale read “completely unacceptable”. The parents were asked by a coordinator to mark on the scale.
A statistical software (SPSS, IBM Corporation) was used to evaluate the normality and was followed by 1-way ANOVA to compare the mean of three independent groups and Post Hoc Analysis (Bonferroni).
Results
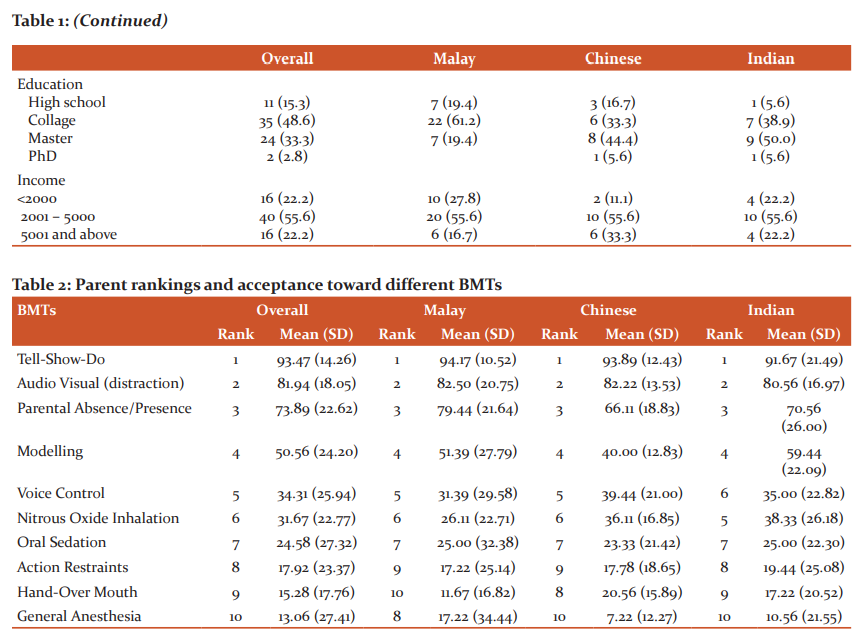
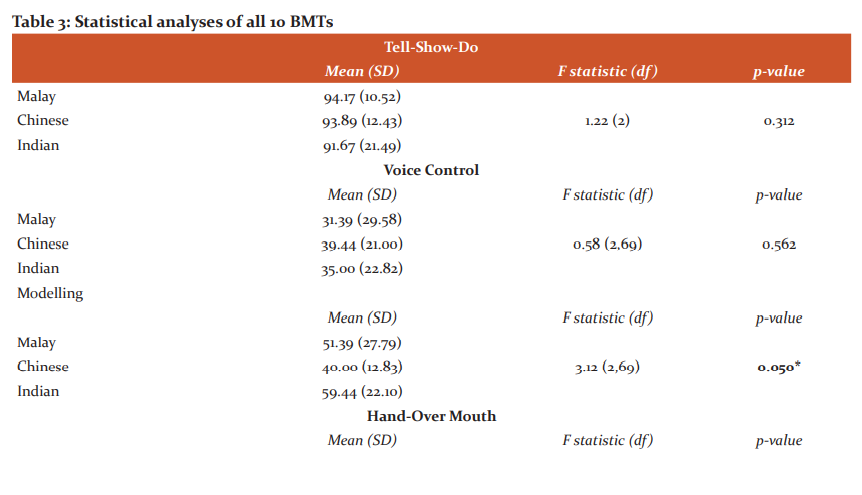
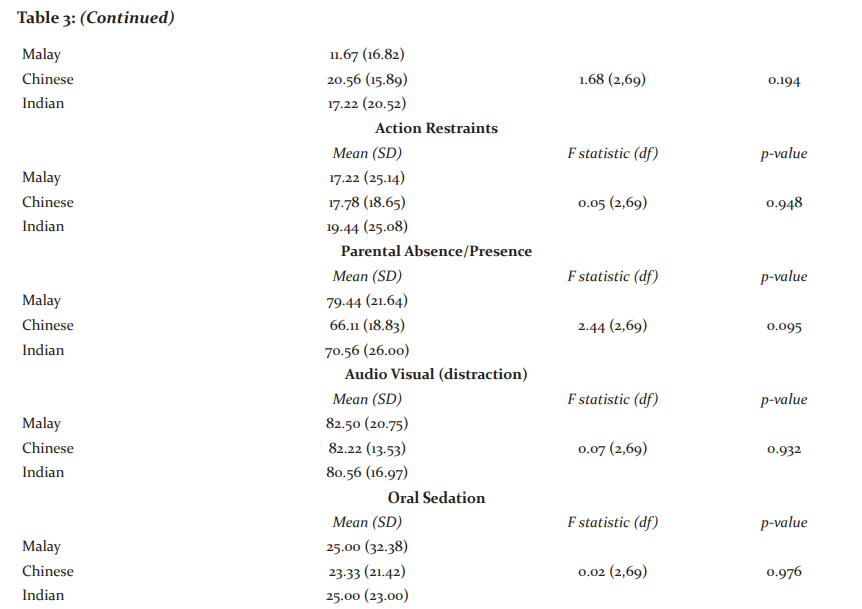
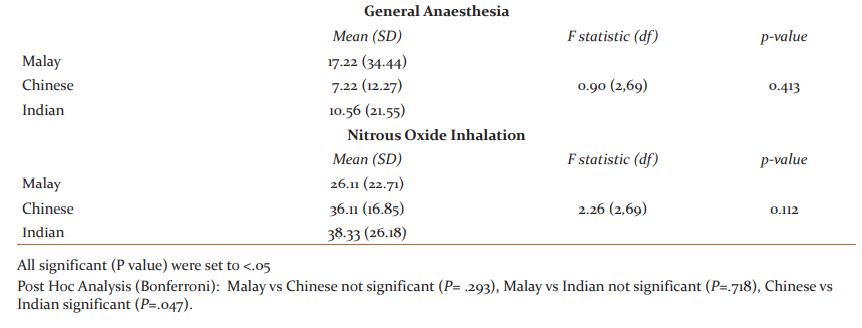
The demographics of the parents have been described in Table 1. The rankings provided by the parents of each ethnicity have been demonstrated in Table 2. Statistical analysis of individual BMTs revealed a significant difference in the three ethnicities (P=.05) with all other techniques remaining unremarkable when compared in the three groups. Detailed outcomes of each BMT has been described in Table 3.
Discussion
The current study aimed to evaluate the different BMT acceptability levels within Chinese, Indian and Malay ethnicities. Nine out of 10 BMTs demonstrated no significant differences in the amount of approval among the three ethnicities with only BMT modelling showing significant differences (P=.05). Therefore, the null hypothesis was partly rejected. This study found that all three ethnicities equally approved Tell-Show-Do, Audio Visual (distraction), Parental Absence/Presence and Modelling. However, there was a significant difference (P<.05) in the amount of approval given to modelling when comparing Chinese and Indian ethnicities. While previous studies have shown modelling as an effective technique with either filmed modelling5 or live modelling6,7 in the Western world, the current study presents contradictory findings when comparing the attitudes of the two largest Asian ethnicities. Modelling and positive/negative reinforcements have had mixed results in the past with certain authors preferring positive 8 while others commenting for negative3,9-11 attribute these possible disagreements to cultural differences12,13 argued that modelling is only effective when the child’s anxiety is controlled before the procedure and the child can be modelled at a relaxed state. However, this study was limited to evaluating Chinese parents of Malaysia and the findings could be different if carried out in Mainland China or India.
While tell-show-do has presented the most popular BMT, similar to previous findings3,9, distraction was also a highly preferred technique. This disagrees with older studies 10 which questioned the effectiveness of the technique. However, children nowadays are more attuned to mobile multimedia and therefore are more sensitive to visual distraction techniques. The current findings agree with previous authors in terms of general acceptability of voice command 14and the widespread disapproval of general anaesthesia in the Asian culture.15 The ‘hand-over-mouth’ technique along with other forms of physical restraint have been labelled controversial and the current Asian findings are similar to results of previous studies conducted in Europe.2,10 In addition to physical restraint, most Asian parents disapproved the readily available conscious sedation as well as general anaesthesia, as was seen in European parents as well.2
Finally, the method of child upbringing greatly affects the type of BMT effective on the child.16 Authors found that authoritative parenting allows for more cooperative children in the dental practice requiring no BMTs in most cases.17 Other studies indicated that authoritarian and permissive parents likely encourage their children to respond to positive behaviour.18 Overprotective parenting, however, leads to the child being less tolerant of sufferings and in most cases require some form of BMT during dental care.19,20 Whether the same findings hold for Asian ethnicities should be a subject of future research. Further studies can be done to evaluate the correlation of different demographic variables in Asian culture, which may affect the child’s behaviour and required BMT in dental practice.
Conclusion
Tell-show-do, distraction and modelling parental presence/absence and reinforcements have been shown to produce similarly acceptable results amongst Asian parents with statistically insignificant differences in the amount of approval given for the techniques. Physical restraint, oral sedation and general anaesthesia were the least approved in the current study.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals from where the literature for this article has been reviewed and discussed.
Conflicts of Interest: The authors declare no conflict of interest.
Funding: This research received no external funding.

References:
1. O'Callaghan PM. The efficacy of noncontingent escape for decreasing disruptive behaviour during dental treatment. J Appl Behav Anal 2006;39(2):161–171.
2. Nunn J, Foster M, Master S, Greening S. British Society of Paediatric Dentistry: a policy document on consent and the use of the physical intervention in the dental care of children. Int J Paediatric Dent 2008;18:39-46.
3. Roberts J, Curzon M, Koch G, Martens L. behaviour management techniques in paediatric dentistry. Eur Arch Paediatr Dent 2010;11(4):166-174.
4. Levitt J, McGoldrick P, Evans D. The management of severe dental phobia in an adolescent boy: a case report. Int J Paediatr Dent 2000;10(4):348-353.
5. Melamed BG, Hawes RR, Heiby E, Glick J. Use of filmed modelling to reduce the uncooperative behaviour of children during dental treatment. J Dental Res 1975;54(4):797-801.
6. Ghose LJ, Giddon DB, Shiere FR, Fogels HR. Evaluation of sibling support. ASDC J Denti Children 1969;36(1):35.
7. Gordon D, Terdal L, Sterling E. The use of modeling and desensitization in the treatment of a phobic child patient. ASDC J Dent Child 1974;41(2):102.
8. Wright GZ, Kupietzky A. non-Pharmacologic approaches in Behavior Management. Behav Mgmt Dent Children 2014:63-69.
9. Newton JT, Sturmey P. Students' perceptions of the acceptability of behaviour management techniques. Eur J Dental Edu 2003;7(3):97-102.
10. Campbell C, Soldani F, Busuttil-Naudi A, Chadwick B. Update of Non-pharmacological behaviour management guideline. 2011;34:1-37.
11. Chang CT, Badger GR, Acharya B, Gaw AF, Barratt MS, Chiquet BT. Influence of ethnicity on parental preference for pediatric dental behavioral management techniques. Pediatr Dent 2018;40(4):265-272.
12. Coll CG, Pachter LM. Ethnic and minority parenting. Handbook of Parenting Volume 4 Social Conditions and Applied Parenting. 2002:1.
13. Machen JB, Johnson R. Desensitization, model learning, and the dental behavior of children. J Dent Res 1974;53(1):83-87.
14. Greenbaum PE, Turner C, Cook EW, Melamed BG. Dentists' voice control: Effects on children's disruptive and affective behavior. Health Psychol 1990;9(5):546.
15. Wong D, Perez-Spiess S, Julliard K. Attitudes of Chinese parents toward the oral health of their children with caries: a qualitative study. Pediatr Dent 2005;27(6):505-512.
16. Robinson CC, Mandleco B, Olsen SF, Hart CH. Authoritative, authoritarian, and permissive parenting practices: Development of a new measure. Psychol Rep 1995;77(3):819-830.
17. Aminabadi NA, Deljavan AS, Jamali Z, Azar FP, Oskouei SG. The influence of parenting style and child temperament on child-parent-dentist interactions. Pediatr Dent 2015;37(4):342-347.
18. Howenstein J, Kumar A, Casamassimo PS, McTigue D, Coury D, Yin H. Correlating parenting styles with child behavior and caries. Pediatr Dent 2015;37(1):59-64.
19. Casamassimo PS, Wilson S, Gross L. Effects of changing US parenting styles on dental practice: perceptions of diplomates of the American Board of Pediatric Dentistry. Pediatr Dent 2002;24(1):18-22.
20. Juneja A, Sultan A, Siddiqui M. A Retrospective Evaluation of Traumatic Dental Injuries in Children Visiting Dental Setup in Delhi NCR. Int J Cur Res Rev 2020;12(22):76-81
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





