IJCRR - 13(4), February, 2021
Pages: 132-138
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
A Standardized Formula to Analyse the Neurovascular Safety in Clavicular Plating; An Anatomical Study
Author: Shruthi BN, Vivikta Venkatesh, Chandrakala C, Akash Venkatesh, Sarala HS
Category: Healthcare
Abstract:Introduction: Clavicle shaft fractures are common traumatic injuries that occur in the middle third of the clavicle, treatment is controversial but may be nonoperative or operative based on the degree of displacement and patient factors. Objective: Our present study aims to determine a relationship between the length of the clavicle and the depth at which the neurovascular structures lie. Methods: Our study was conducted on 30 cadavers (30 right upper limbs & 30 left upper limb). Measuring tape, vernier callipers and cay wires were used to determine the length and the depth of the clavicle. Results: After the thorough statistical observation and analysis of the data set, we were able to apply the regression equation. By careful calculation, we derived the regression coefficient for this particular data set and were able to arrive at an accurate result. Conclusion: Hence, by this equation, we could determine the depth of the neurovascular structures just by knowing the length of the clavicle. The present study could help orthopaedics intraoperatively in the precise selection of the screws which could minimize the risk of injury to subclavian vessels in the surgery and favour desirable outcomes.
Keywords: Clavicular fracture, Clavicular plating, Subclavian vessels, Clavicular length, Neurovascular bundle, Standardized formula
Full Text:
INTRODUCTION
The clavicle or the collar bone is one of the most peculiar bones in our body. It is the only long bone which lies horizontally and has two primary centres of ossification with a membranous development. This bone is responsible for the transmission of weight from the upper limb to the trunk. The clavicle is closely related to the neurovascular structures supplying the upper limb. Hence, breakage or fracture of the bone can have adverse effects on the day to day lifestyle of the affected individual. The clavicle has important anatomical relationships with subclavian vessels and brachial plexus, especially in its middle third, where the curvature is the reference point used for accessing these structures. In case of trauma or surgery in the middle third of the clavicle, fixation is done employing open surgery using synthetic material; these structures may become injured because of their anatomical proximity.1,2
Plating of clavicle fractures has been thought a safe and reliable procedure but it is not without risks. There are 2 described locations for plate placement in clavicle fractures, superior and anterior. Those who advocate of superior plating claim less soft-tissue injury, stronger biomechanical profile, and easier surgical technique.3-5 Complications of superior plating include injuries to major neurovascular structures as subclavian vessels and brachial plexus.6 Iatrogenic neurovascular complications are fortunately rare. However, there are several case reports and small series of limb-threatening and even fatal neurovascular complications after clavicle surgery.7 These injuries have been reported while drilling or screwing.8-10
Given their rarity, we could find no high-level studies that looked specifically at neurovascular injuries but represents a potentially devastating outcome from an operation that is treating a problem that is neither life nor limb-threatening. If the screw applies pressure to the underlying structures or pierces it, it could lead to adverse effects since these underlying structures are responsible for the entire neurovascular supply of the upper limb. Several reports have advocated different techniques to avoid damaging these important infraclavicular structures but an excessive undesired soft-tissue dissection is required or a safe drilling angle should be calculated which is not easy during the trauma surgery.
This study aims to find the simple and effective method to avoid neurovascular complications in clavicle fractures plating by determining the relationship between the depth at which the neurovascular structures lie from the length of the clavicle. This helps the orthopaedic surgeons by choosing the right sized screw for clavicular plate fixture surgeries. This establishes neurovascular safety at the surgery of the middle third of the clavicle, employing dissection in cadavers.
MATERIALS AND METHODS
Inclusion and Exclusion Criteria
This study is cadaveric, 30 cadavers of an elderly age group between 55-70yrs, with a mean weight of 70kg, mean height 1.7m. Both sides of the cadaveric specimen were used and they were void of any congenital malformations, trauma or previous surgery in the shoulder region.
Instruments
Cay wires, bone drill, measuring tape, vernier callipers and instruments in the anatomical dissection kit were used which include scalpel, forceps and scissors.
Procedure
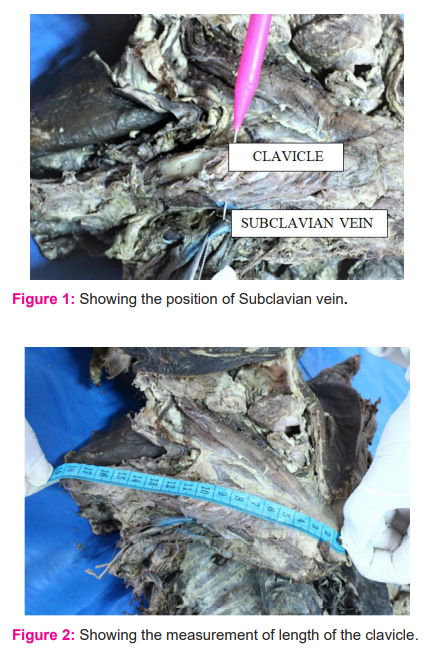
30 adult south Indian cadavers were dissected in the clavicular region bilaterally. The standard guidelines to expose the clavicular area were followed according to Cunningham’s manual of dissection, volume 1, 16thedition11. Deep dissection was performed on either side of the cadavers to expose the clavicle and the neurovascular structures beneath it. The following structures were identified: subclavian vein, upper trunk of brachial plexus and supraclavicular nerves. The subclavian vein is marked to measure the distance from the most proximal point of the middle third of clavicle (Figure 1).
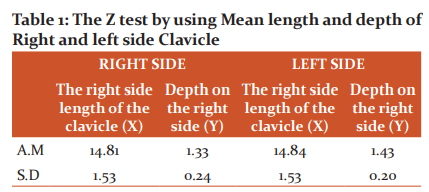
The baseline anatomical measurements like the length of the clavicle are measured by plating from the acromioclavicular joint that is the outermost part of acromial end on the lateral side to the sternoclavicular joint that is the innermost part of sternal end on the medial side by using measuring tape without considering the bony curvatures (Figure 2). While taking the length of clavicle the midpoint was calculated and marked with marking pencil. The superior clavicular plate was screwed from the superior surface and screw was introduced at the midpoint of the clavicle consequently, the depth is measured from the nearest clavicular cortex from the screw tip to the subclavian vein by keeping the arm in anatomical position. The data obtained were photographed and tabulated separately for right and left upper limbs. Then the data was statistically analysed using Microsoft excel.
The regression equation is as follows:
Y-y=byxX-x
Y is the depth of the subclavian vessels from the clavicle
X is the length of the clavicle for which you would calculate the depth
Statistical Analysis
Based on the regression equation our research has arrived at a formula which can determine the depth at which the subclavian vessels are situated concerning the clavicle measuring from its superior surface by knowing the length of the clavicle. The regression equation helps us in determining a dependent variable based on an independent variable. In this case, the independent variable would be the length of the clavicle and the dependent variable would be the depth of the neurovascular structures from the clavicle.
The regression equation of Y on X
To estimate the depth of subclavian vessels are situated based on length of clavicle both on Right side and Left side)
Y = y + b yx (X- x)
Here,
Y is the depth of the subclavian vessels from the clavicle
y is the mean of the depth of the clavicle
byx is the regression coefficient
X is the length of the clavicle for which you would calculate the depth
x is the mean of the length of the clavicles
The regression coefficient can be calculated as follows:
byx=n∑xy-∑x ∑y / n ∑x2 – (∑x)2
Here,
∑xy is the sum of the product of the length of the clavicle and underlying depth.
∑x is the sum of the lengths of the clavicles
∑y is the sum of the underlying depths of the structures
∑x2 is the sum of the squares of the lengths of the clavicle
(∑x)2 is the square of the sum of the lengths of the clavicle
N is the number of specimens
RESULTS
The anatomical distance from the midpoint of the clavicle to the subclavian vein was measured in all the specimens with the arm held in anatomical position. The mean values of all the specimens are tabulated in table 1 and 2. A data set was formed with the following information, length of the clavicle, mid-point of where the hole was drilled and the depth of the neurovascular structures.
The mean length of clavicular length on right 14.81cm and left side 14.84 cm, and from the middle of the clavicle to the subclavian vein, the mean depth is 1.33cm & 1.43 cm on right and left side respectively.
The standard deviation of the clavicular length on the right and left side is 1.53cm on both right and left side. The SD of the depth at which the vessels lie is 0.24cm and 0.20cm on right and left sides respectively.
RIGHT SIDE
Calculating for the right side Regression Coefficient,
∑x=444.2
∑y=39.86
∑xy= 589.74
∑x2=6644.58
(∑x)2=197313.6
X= 14.81
Y= 1.33
Substituting the above values in the equation for the regression coefficient formula we get,
Regression coefficient (byx) = n∑xy-∑x ∑y / n ∑x2 – (∑x)2
= 30*596.35-(444.2) (39.86)/ 30*6644.58-197313.6
byx = -0.0067
Therefore, regression co efficient (byx) for the right side = -0.0067
Y on X Regression equation is fitted, to find the depth of subclavian vessels is situated based on length of clavicle on Right side.
For example to estimate depth when length of clavicle on right side is x = 12.4
Y = y + b yx (X- x)
= 1.33 + (-0.0067) (X – 14.81)
=1.33-0.0067X +0.0992
= 1.4292 – 0.0067X
= 1.4292 – 0.0067 (12.4)
= 1.4292-0.0830
Y (12.4) =1.3462
LEFT SIDE
∑xy=634.2
∑x=445.3
∑y=42.9
∑x2=6677.51
(∑x2) =198292.1
X= 14.84
Y= 1.43
Substituting the above values in the equation for the regression coefficient formula we get,
Regression coefficient (byx) = n∑xy-∑x ∑y / n ∑x2 – (∑x)2
=30*634.2-445.3*42.9/30*6677.51-198292.1
byx = - 0.0381
Therefore, regression co efficient (byx) for the left side is = - 0.038
Y on X Regression equation is fitted, to find the depths of subclavian vessels are situated based on length of clavicle on Left Side.
For example to estimate depth when length of clavicle on left side is x = 12.3
Y = y + b yx (X- x)
= 1.43 + (-0.0381) (X – 14.84)
=1.43-0.0381X + 0.5654
= 1.9954 – 0.0381X
= 1.9954 – 0.0381 (12.3)
=1.9954-0.4686
Y(12.3) =1.5268
To Analyse the Z test by using Mean length and depth of Right and left side Clavicle is given in Table 1.
Z test: (To know is there any significant difference in length of Clavicle considering in right and left side)
To analyse the significant difference between Right and Left side Length of Clavicle
The Null Hypothesis:
H0: There is no significant difference between Right and Left side Length of Clavicle
H1: There is a significant difference between Right and Left side Length of Clavicle
Under H0 the test statistic is
Z = X1 –X2 is ~ N(0,1)
s12 +s22
n1 n2
Z= -0.093, (The P-value is 0.9259, 0.9259 >0.05 therefore it is not significant)
Here the test is the two-tail test at 5% level of significance, the critical values are -1.96 and 1.96
Since the value lie within this region, therefore, H0 is accepted,
That is there is no significant difference between Right and Left side Length of Clavicle
Z test: (To know is there any significant difference in depth of Clavicle considering in right and left side)
To analyse the significant difference between Right and Left side depth of Clavicle
The Null Hypothesis:
H0: There is no significant difference between the Right and Left side depth of Clavicle
H1: There is a significant difference between the Right and Left side depth of Clavicle
Under H0 the test statistic is
Z = X1 –X2 is ~ N(0,1)
s12 +s22
n1 n2
Z= -1.758 (The P –value is 0.0787, 0.0787 >0.05 therefore it is not significant)
Here the test is the two-tail test at 5% level of significance, the critical values are -1.96 and 1.96
Since the value lie within this region, therefore, H0 is accepted.
Correlation Analysis is used to find the correlation between length and depth of Right and left side Clavicle (Figure 1)
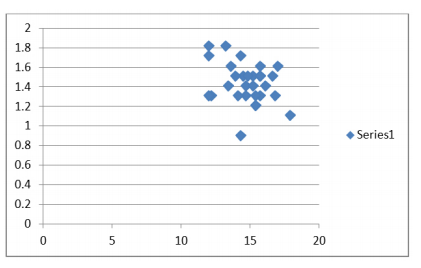
Figure 1: Correlation between length and depth of clavicle in right limbs. r = -0.0419, P-value 0.829, It is not significant. Calculations and digits are expressed in centimeter.
Correlation Analysis is used to find the correlation between length and depth of Right and left side Clavicle (Figure 2)
Figure 2: Correlation between length and depth of the clavicle in left limbs. r = - 0.2905, P-value 0.12, It is not significant. Calculations and digits are expressed in centimeter.
After the data set were grouped & thorough statistical analysis we came to know that:
-
There is no significant difference between Right and Left side Length of Clavicle
-
There is no significant difference between the Right and Left side depth of Clavicle.
-
Z test: (To know there is any significant difference in depth of Clavicle considering in right and left side)
-
Z= -1.758 (The P –value is 0.0787, 0.0787 >0.05 therefore it is not significant)
-
Here the test is the two-tail test at 5% level of significance, the critical values are -1.96 and 1.96
-
Since the value lie within this region, therefore, H0 is accepted
-
Correlation between Right length and depth of clavicle : r = -0.0419, P value 0.829, It is not significant.
-
Correlation between Left length and depth of clavicle : r = - 0.2905, P value 0.12, It is not significant.
DISCUSSION
Clavicular fractures at midshaft (at the junction of medial 2/3rdand lateral 1/3rd) are very common. The most common and current treatment of choice is the internal fixation with superior plating. Though there are many options available for surgical fixation, like clavicular plating and intramedullary(IM) fixation they pose highest risk. IM fixation has the potential advantages of a smaller incision and less dissection and soft tissue exposure. For the last two decades, the use of rockwood and hagie pins represented the most popular form of IM implants. The use of alternate IM implants, such as Kirschner wires, titanium elastic nails, and cannulated screws, also has been described in limited case series. However, concerns persist regarding the complications associated with the use of these implants.
Though there are several studies which have reported regarding the morphometry of clavicle, there is less number of studies which report a method which aids in the accurate selection of screws to avoid these iatrogenic injuries. The present study establishes the interrelationship between the length of the clavicle to that of the depth at which the subclavian vein lies to reduce the complications caused due to IM devices.
The 3-dimensional study by Sinha12have reported that the subclavian vein is closely related to the clavicle in the medial half, drills and screws should be aimed superior to inferior in the medial third and anterior to posterior in the middle third of the clavicle. Caution must be employed if the measured screw length is >16 mm. This is derived from the narrowest reported clavicle thickness (11 mm) and the closest reported distance of the vessels to the middle third of the clavicle (5 mm). If the screw is longer than this or is markedly longer than the adjacent screws, the surgeon must pay close attention to the trajectory of the screw and the degree of prominence to ensure they are within the safe range. The maximum allowable is 4 mm, based on the closest reported distance of the vessels to the middle third of the clavicle (5 mm).
A cadaveric study by Robinson3 has found out that the closest structure to the clavicular cortex is a subclavian vein which lies about 4.8mm. Unlike other surgical approaches, palpation or visualization of the deep neurovascular structures at risk is difficult to be performed by a single approach and performing additional incisions is not part of the routine approach.
The minimum screw prominence resulting in a vascular injury was 8 mm. It is alarming that this length is less than the report
References:
1. Standring S. Gray's anatomy: the anatomical basis of clinical practice. 40th ed. New York: Churchill Livingstone; 2008:406-407.
2. Basamania CJ, Rockwood CA Jr. Fractures of the clavicle. In: Rockwood CA Jr, Matsen FA 3rd, Wirth MA, Lippitt SB, editors. The shoulder. 4th ed. Philadelphia: Saunders; 2009:617-770.
3. Hussey MM, Chen Y, Fajardo RA. Analysis of neurovascular safety between superior and anterior plating techniques of clavicle fractures. J Orthop Trauma 2013;27:627–632.
4. Celestre P, Roberston C, Mahar A. .Biomechanical evaluation of clavicle fracture plating techniques: does a locking plate provide improved stability? J Orthop Trauma 2008;22:241–247.
5. Iannotti MR, Crosby LA, Stafford P. Effects of plate location and selection on the stability of midshaft clavicle osteotomies: a biomechanical study. J Shoulder Elbow Surg 2002;11:457–462.
6. Qin D, Zhang Q, Zhang YZ. Safe drilling angles and depths for plate-screw fixation of the clavicle: avoidance of inadvertent iatrogenic subclavian neurovascular bundle injury. J Trauma 2010;69:162–168.
7. Clitherow HDS, Bain GI. Major neurovascular complications of clavicle fracture surgery. Shoulder Elbow 2015;7:3–12.
8. Ding M, Hu J, Ly H. Iatrogenic subclavian arteriovenous fistula: a rare complication of plate osteosynthesis of clavicle fracture. Orthopedics 2012;35:287–289.
9. Johnson B, Thursby P. Subclavian artery injury caused by a screw in a clavicular compression plate. Cardiovasc Surg 1996;4:414–415.
10. Ring D, Holovacs T. Brachial plexus palsy after intramedullary fixation of a clavicular fracture. A report of three cases. J Bone Joint Surg Am 2005;87:1834–1837.
11. Cunninghams manual of dissection. Vol 1, 11th edition; Pg 54-58.
12. Sinha A, Edwin J, Sreeharsha B. A radiological study to define safe zones for drilling during plating of clavicle fractures. J Bone Joint Surg Br 2011;93B:1247–1252.
13. Robinson L, Persico F, Lorenz E. Clavicular caution: an anatomic study of neurovascular structures. Injury 2014;45:1867–1869.
14. Galley IJ, Watts AC, Bain GI. The anatomic relationship of the axillary artery and vein to the clavicle: A cadaveric study. J Shoulder Elbow Surg 2009;18:21–25.
15. Wijdicks FJ, Van der Meijden OA, Millett PJ, Verleisdonk EJ, Houwert RM. Systematic review of the complications of plate fixation of clavicle fractures. Arch Orthop Trauma Surg 2012;132:617–625.
16. Collinge C, Devinney S, Herscovici D.Anterior-inferior plate fixation of middle-third fractures and nonunions of the clavicle. J Orthop Trauma 2006;20:680–686.
17. Venkatachalam S, Packer GJ, Sivaji CK. Anterior versus superior plating of fresh mid-shaft clavicular fractures. Injury Extra 2008;39:170–171.
18. Chauhan A, Gawande V, Saoji KK, Mittal A. The outcome of Distal End Clavicle Fractures Treated with Locking Plates, Int J Curr Res Rev 2020;12(14):30-34
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





