IJCRR - 13(4), February, 2021
Pages: 65-69
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
Histomorphometry of Pretransverse Segment of Vertebral Artery and its Clinical Significance - A Cadaveric Study
Author: Prabavathy G, Sadeesh T, Arthi G, Anbalagan J
Category: Healthcare
Abstract:Introduction: Multiple variations in the origin of the vertebral artery have been reported in the literature. Objective: To study the variability in the origin and course of the vertebral arteries on both sides in both sexes and also to compare its microstructure. Methods: The vertebral artery was studied from 60 adult human cadavers on both sides. The origin and point of entry into foramen transversarium were studied and the dimensions of the artery were measured and tabulated. Results: In all 60 cadavers, the right vertebral artery (RVA) originated from the posterosuperior aspect of the first part of the subclavian artery. The left vertebral (LVA) originated from the first part of the left subclavian artery in 52 cadavers (87%). In 8 male cadavers (13%), the left vertebral artery originated directly from the arch of the aorta. The anomalous origin of LVA was longer than the right and the diameter was smaller than that of RVA. Amongst the 8 cadavers, one case appeared hypoplastic with wider close to the origin, constricted, and narrow in the middle part. In remaining cases of the normal origin of the vertebral artery, there was a significant increase in length and diameter of the vertebral artery in males compared to females on both sides. There is a predominantly increase in the length and diameter of the right vertebral artery when comparing both sexes. Conclusion: A thorough understanding of anomalous vertebral arteries is paramount when performing both diagnostic and interventional angiography.
Keywords: Vertebral artery, Aortic arch, Cervical vertebra, Variation, Development, Morphometry
Full Text:
INTRODUCTION
Vertebral artery shows multiple variations in its origin and course. The vertebral arteries originate from the posterior superior aspect of the first part of the subclavian artery.1 The vessels take a vertical posterior course to enter into the foramen transversarium of the sixth cervical vertebra. The segment of the artery from its origin at the subclavian artery to its respective transverse foramen is termed as pre-transverse or prevertebral segment.2 The second part passes through foramen transversarium of sixth cervical vertebra (C6) to the first cervical vertebra (C1). The third part curves medially behind the lateral mass of the atlas. It passes through foramen magnum as fourth part and at the lower border of pons; two vertebral systems unite to form the basilar artery. The vertebral arteries form the vertebrobasilar vascular system and supply blood to the upper spinal cord, cerebellum, and posterior part of the brain stem. Topographically, the vertebral artery is divided into four parts: cervical or prevertebral, vertebral, sub-occipital, and intracranial part.3
Origin of the abnormal vertebral artery has been noted incidentally during anatomic postmortem and angiographic examinations, because, they are clinically asymptomatic in most cases. However, such types of abnormalities are of diagnostic importance either before vascular surgery in the neck or in intravascular diseases such as arteriovenous malformations or cerebral aneurysms.4 Anatomical knowledge of vascular variations may help to avoid wrong interpretation of the non-opacification of the vertebral artery, as blockage or stenosis. Nizanowski et al.5 studied the course and variations of the left vertebral artery (LVA). The clinical importance of such variations in cerebrovascular disorders, head and neck surgery, angiography and arterial dissection has been cited in the literature.6,7 The prevalence of the left vertebral artery arising from the aortic arch is reported to be 2.4-5.8%. LVA arising from the arch of aorta reported entering the foramen transversarium of fourth or fifth cervical vertebra instead of the sixth cervical vertebra.8 Variations in the abnormal origin of the vertebral artery may cause cerebral disorders.
A case of bilateral vertebral arteries originating from the aortic arch proximal to the left subclavian artery has been reported.9 Lemke et al.4 reported nine cases of right vertebral artery (RVA) arising from the aortic arch. Preeti et al.10 reported that they observed a common stem for left subclavian artery and left vertebral artery, arising from the arch of the aorta with the incidence of 2.5% of 40 cases studied. Anatomical knowledge of anomalous origin and dimensions of supra-aortic arteries are important in emergency patients undergoing four-vessel angiography. A review of the literature showed insufficient data on the morphometric and histological comparison of both normal and anomalous origin of the vertebral artery. The present work is aimed to study the variability in the origin, course and dimensions of the vertebral arteries on both sides in both sexes and also to compare its microstructure.
MATERIALS AND METHODS
The vertebral artery was studied in 60 dissected adult cadavers on both sides collected from the Department of Anatomy, Mahatma Gandhi Medical College, Sri Balaji Vidyapeeth, Puducherry, after the completion of neck dissection by undergraduate students. The sample included 30 male and 30 female cadavers in the age group of 60 - 70 years. In all the cadavers the scale no-vertebral region was dissected to expose the prevertebral segment of the vertebral artery on both sides. The superior mediastinum was dissected to expose the arch of the aorta with its branches. The following parameters were considered for the present study. 1. Site of origin of the vertebral artery on the left and right side 2. Length of vertebral artery from its point of origin to the entry at foramen transversarium of the cervical vertebra using digital Vernier calliper and a thread. 3. The diameter of vertebral arteries at its origin and entry at the foramen transversarium were measured using digital vernier calliper 4. The level of entrance of the vertebral artery at foramen transversarium 5. Variations in its origin, topographic and morphological variations were recorded.
For the histological study, a small segment of the artery was cut at its origin and the entry into foramen transversarium. The tissue was subjected to routine histological procedures and sections were stained with Haematoxylin and Eosin, and observed under the microscope. The thickness of the arterial wall, arrangement of smooth muscle, and elastic fibres were recorded.
Statistical analysis
The data were analyzed using software SPSS 20. A comparison of the length of the vertebral artery in males and females on both sides was analyzed using Student ‘t’ test. The diameter of the vertebral artery at the proximal and distal part was done using the Mann-Whitney U test. P<0.05 was considered statistically significant.
Results
Among 60 cadavers studied, the right vertebral artery originated from the posterosuperior aspect of the first of the subclavian artery in all cases (Figure 1a). The left vertebral originated from the first part of the left subclavian artery in 52 cadavers (87%). In all cases, vertebral arteries crossed the stellate ganglion, ventral rami of seventh and eighth cervical spinal nerves before entering the foramen transversarium of the C6 vertebra.
In the remaining eight cadavers (13%) left vertebral artery was found originating directly from the arch of the aorta between left common carotid and left subclavian artery. The prevalence was mostly in male cadavers. The left vertebral ascended along the lateral border of longus colli in the scaleno vertebral region. The stellate ganglion and ventral rami of C7, C8 was behind the vessels and were crossed by thoracic duct and inferior thyroid artery anteriorly. In all these cases, the left vertebral artery entered the foramen transversarium of C5. The anomalous origin of LVA was longer than the right and the diameter was smaller than that of RVA. Amongst the eight cadavers, one case appeared hypoplastic with wider close to the origin, constricted, and narrow in the middle part (Figure 1b, c). Arterial segments were collected at a wider and narrow distal part for structural analysis.
The mean length and standard deviation of normal origin of the vertebral artery were compared in 52 cadavers on both sides. After intercomparison, on the right side, the p-value was found to be 0.003 (p<0.05) and p=0.002 on the left side, which was statistically significant (Table 1). Hence, a significant increase in the length of the vertebral artery was observed in males than the female on both sides indicating predominance in the length of the right side vertebral artery in either sex.
On comparing the diameter of the vertebral artery at its origin on both sides, the p-value was found to be 0.004 and <0.001(p<0.05) which was statistically significant showing increased diameter in males compared to females (Table 2). On comparing the diameter of the vertebral artery at its entry into foramen transversarium on both sides, the p-value was found to be <0.001 (p<0.05) which was statistically significant showing increased diameter in males compared to females (Table 3).
Histological features
Structural features of the proximal, middle and distal segments of vertebral arteries on both sides were studied in 60 cases. No significant structural difference in the layers of the vertebral artery was observed. However, a marked structural change was observed in one anomalous originated LVA. In the proximal segment, the absence of internal elastic lamina, the presence of more elastic fibres and smooth muscles in tunica media were observed. Tunic adventitia showed collagen fibres (Figure 2a). The middle segment showed the narrowest lumen, with thin tunica intima and media. The distal segment showed a prominent internal elastic lamina with increased layers of smooth muscle in tunica media, collagen fibres in tunica adventitia were observed (Figure 2b, c). Normal features of muscular artery features were observed in all the right side vertebral artery (Figure 2d, e).
Discussion
Anatomical and topographical variations of the vertebral artery are of immense importance in surgery, angiography, and all non-invasive radio diagnostic procedures.2 Without a thoroughly comprehensive knowledge of anomalous origins of the great vessels; angiography can be difficult or impossible. If the vertebral arteries are not originating in their normal position, this finding can be misinterpreted as the vessels being congenitally absent. Variation in the origin of the vertebral artery may expose the patient to the formation of an intracranial aneurysm, due to the altered hemodynamics
Earlier studies have reported numerous variations in the origin of the vertebral artery. The origin of the left vertebral artery directly from the aortic arch between the left subclavian artery and the left common carotid artery is the most common variation with a distribution of (2.4-5.8%). In such cases, the left vertebral artery generally enters the transverse foramen of C4-C5 rather than C6.8
The incidence of aortic origin of the Left vertebral artery was cited by many authors. 3.1% by Nizanowski et al.5, 5% by Vorster et al.11, 3% by Matula et al.2, 5% by Panicker et al.12 and 7% Fayza et al.13 In the present study, we found an increased incidence of aortic origin of the LVA in 13% cases.
Bruneau et al.14 studied 500 vertebral arteries, they observed an abnormal level of entrance into foramen transversarium in 7% specimens (35 cases). In our study, we found that the aortic origin of the left vertebral artery entered the transverse foramen of the fifth cervical vertebra in all 8 cadavers (13%). In remaining cases on both sides, the vertebral artery entered the transverse foramen of the sixth cervical vertebra. Sikka and Jain15 reported that the length may vary according to the origin of the vertebral artery, and according to the vertebra at which it enters the transverse foramen. In the present study, in all the 8 cadavers of anomalous origin of LVA, the length of the left vertebral artery is more than its right counterpart.
Imre et al.16 reported a reduced diameter (5.51 mm) of the variant LVA at its origin. Their findings are concordant with our result, that in all 8 cases of anomalous origin, the left vertebral artery diameters were significantly smaller than those of the right side. Dodevski et al.17 reported that the VA on both sides was equal in diameter in 23.3% patients. The right VA was larger in 30% patients, and the left VA was larger than the right in 46.6% of patients. In the present study, there was a significant increase in the length of the vertebral artery in males compared to females on both sides. There is a predominantly increase in the length of the right vertebral artery when comparing both sexes. The diameter of the vertebral artery both at its origin and entry into foramen transversarium showed increased diameter in males compared to females.
A hypoplastic artery (diameter < 3.5 mm) was found in 8.6% of the cases studied by Matulaetal2. Among the eight cadavers in our study, in one case the left VA is hypoplastic, it was wider close to the origin, constricted, and narrow in the intermediate part. The true value of detecting anomalous origin is in the diagnostic gain before vascular surgeries of supra-aortic arteries, and the knowledge of potential vertebral artery variants appears to be mandatory for planning aortic arch surgery or endovascular interventions.
Embryological basis
To understand the hypothetical development of the anomalous origin of the vertebral artery, knowledge of embryonic development of the aortic arch is necessary. Usually, the first part of the vertebral artery develops from the proximal part of the dorsal branch of the 7th cervical intersegmental artery proximal to a postcostal anastomosis. The second part is derived from the longitudinal communications of the postcostal anastomosis. In the present eight cases of anomalous origin of the left vertebral artery, sixth dorsal intersegmental artery might have persisted as the first part of the vertebral artery; hence left vertebral artery is arising from the arch of the aorta.
Conclusion
Knowledge about the morphology and variations of the great vessels of the aortic arch is important to the endovascular interventionist and diagnostic radiologist, for making the proper diagnosis. The morphology and morphometric parameters of both the vertebral arteries studied in both the sexes will be added data and may be important in the design of carotid artery stents, vertebral artery stents, and new therapeutic options for intracranial intervention. The aortic artery branch pattern has to be evaluated before any manoeuvre in the local region to avoid unexpected events due to the existence of aberrant VA. There has been no evidence yet, reporting the clinical signs or symptoms associated with anomalous origins of the vertebral artery. Thorough knowledge of vertebrobasilar variations may improve the outcome of the skull base and other head and neck operations, which also aid in the interpretation of imaging. The present data is to create awareness about topographical and morphological variations and the knowledge may help to avoid complications during surgical and radio diagnostic interventions.
Acknowledgement: We acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. We are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflicts of Interest: Nil
Source of funding:Nil
Contribution Details:
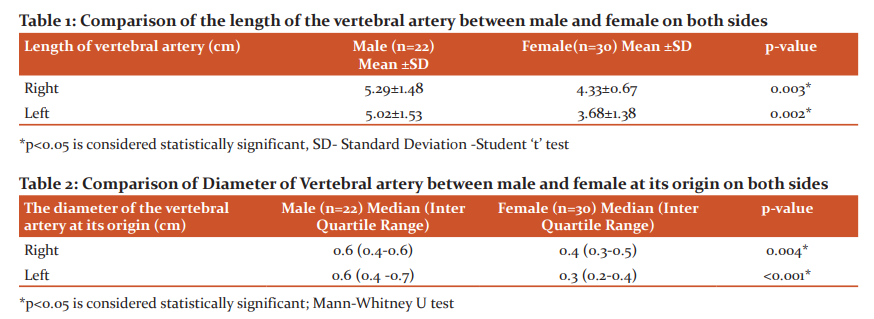
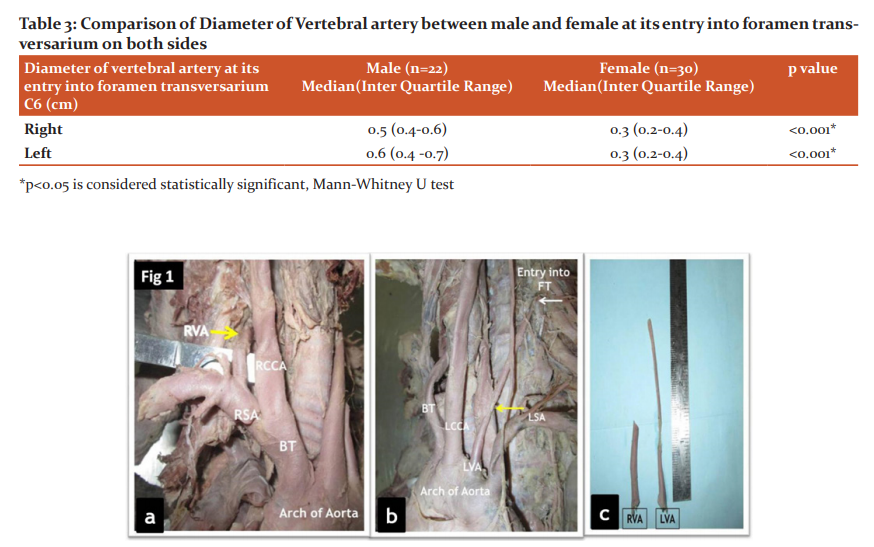
Figure 1: a) Section of the neck showing Right vertebral artery arising from Subclavian artery (BT- Brachiocephalic Trunk, RSA- Right Subclavian Artery, RCCA- Right Common Carotid Artery, RVA- Right Vertebral Artery); b) Section of the neck showing anomalous origin of the left vertebral artery from the arch of the aorta with a narrowed middle segment (Yellow arrow). (LVA- Left Vertebral Artery, LCCA- Left Common Carotid Artery, LSA- Left Subclavian Artery; c) Comparison of length of both vertebral arteries in a case of anomalous origin.
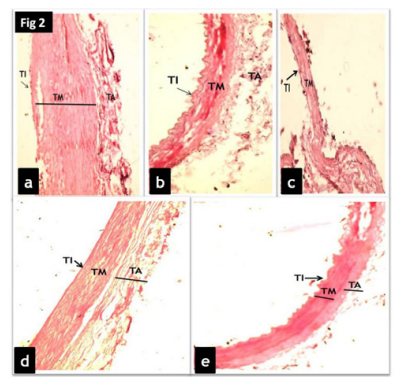
Figure 2: Histological section of an anomalous origin of Left vertebral artery (H&E stain 10x: a- Left vertebral artery -proximal segment, b- LVA- distal segment, c- LVA- middle constricted segment, d- RVA- proximal segment, e- RVA- distal segment) TI- Tunica intima, TM- Tunica media, TA- Tunica adventitia.
References:
-
Moore KL, Dalley AF. Clinically Oriented Anatomy. 4th Ed., Philadelphia-Baltimore-New Aires-Hong Kong-Sydney-Tokyo: Lippincott Williams & Wilkins; 1999:893–94.
-
Matula C, Trattnig S, Tschabitscher M, Day JD, Koos WT. The course of the prevertebral segment of the vertebral artery: Anatomy and clinical significance. Surg Neurol 1997; 48:125-131.
-
Hollinshead WH. Arteries: The Neck. In: Anatomy for Surgeons. Vol. I, The Head & Neck. New York: Paul B Hoeber, Inc, Medical Book Department of Harpers & Brothers; 1954:467–74.
-
Lemke AJ, Benndorf G, Liebig T, Felix R. Anomalous origin of the right vertebral artery: a review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. Am J Neuroradiol 1999; 20:1318–1321.
-
Nizanowski C, Noczynski L, Suder E. Variability of the origin of ramifications of the subclavian artery in humans. Folia Morphol 1982;41:281–294.
-
Vicko, G, Goran I, Damjan M, and Sanja P. Anomalous origin of both vertebral arteries. Clin Anat 1999; 12: 281-284.
-
Komiyana M, Morikawa T, Nakajiman H, Nishikawa M, and Yasui T. High incidence of arterial dissection associated with the left vertebral artery of aortic origin. Neurol Med Chir (Tokyo) 2001;41(1):8-11.
-
Schwarzacher SW, Krammer EB. Complex anomalies of the human aortic arch system: a unique case with both vertebral arteries as additional branches of the aortic arch. Anat Rec 1989; 225(3):246-250.
-
Albayram S, Gailloud P, Wasserman BA. Bilateral Arch Origin of the Vertebral Arteries. Am J Neuroradiol 2002;23(3):455-458.
-
Preeti S, Vasanti A, Rieshav A. Study of variations in the origin and course of vertebral artery. Int J Cur Res Rev 2015;7(14):85-90.
-
Vorster W, Du Plooy PT, Meiring JH. Abnormal origin of internal thoracic and vertebral arteries. Clin Anat 1998;11:33–37.
-
Panicker HK, Tarnekar A, Dhawane V, Ghosh SK. Anomalous origin of left vertebral artery – embryological basis and applied aspects – A case report. J Anat Soc India 2002; 51:234–235.
-
Fayza A, Abd El Gawad, Mohamed H, Shaaban DM, Shuaib HM. Anatomical variations of the vertebral artery and its relation to the atlas vertebra - Radiological and dry bone study. Eur J Anat 2019;23(1):49-58.
-
Bruneau M, Cornelius JF, George B. Anterolateral approach to the V3 segment of the vertebral artery. Neurosurgery 2006; 58:29-35.
-
Sikka A, Jain A. Bilateral variation in the origin and course of the vertebral artery. Anatomy Research International. Hindawi Publishing Corporation. 2012:1-3.
-
Imre N, Yalcin B, Ozan H. Unusual origin of the left vertebral artery. Int J Anat Variat 2010;3:80-82.
-
Dodevski A, Lazareska M, Tosovska-Lazarova D, Zhivadinovik J, Aliji V. Morphological characteristics of the first part of the vertebral artery. Prilozi 2011;32(1):173–188.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





