IJCRR - 13(4), February, 2021
Pages: 59-64
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
Profile of Pediatric Lymphadenopathy- A Cytomorphological Analysis in a Tertiary Care Center of Eastern India
Author: Anasuya Lenka, Mohita Ray, Sukanya Patra
Category: Healthcare
Abstract:Introduction: Lymph node enlargement in the pediatric age group is multifactorial in aetiology and careful assessment of patients combining the clinico-demographic, radiological as well as pathological findings can bring light on various local and systemic diseases which can have trivial effects to even life-threatening consequences for the patients. An easy, rapid and fairly accurate method of Fine needle aspiration cytology (FNAC) is very valuable in giving preliminary diagnosis and guiding further treatment plan for the patient. Objective: To assess the diagnostic role and efficacy of FNAC in the pediatric Lymphadenopathy (LAP) cases. Methods: Data form 235 cytology reports from patients
Keywords: Lymphadenopathy, Pediatric, Fine needle aspiration cytology
Full Text:
INTRODUCTION
In the pediatric age group, lymph node (LN) enlargement is a common finding, owing to exposure of children to a wide variety of infectious agents. Majority of the children have benign self-limiting reactive enlargement of the lymph node. Lymphadenopathy (LAP) also occurs in a small percentage in this age group due to other entities like neoplastic conditions, storage disorders, histiocytosis and sarcoidosis.1,2,3
The geographic variation of the disease prevalence and pattern of lymph node involvement is valuable in suggesting the diagnosis. In most of the cases, the diagnosis can be clinched by proper elicitation of history, clinical examination, ancillary laboratory tests and imaging.4,5In cases where the aetiology remains unexplained for the clinician, or a suspected aetiology needs to be confirmed, Fine needle aspiration cytology (FNAC) is preferred over excisional biopsy, as it is a rapid, minimally invasive and cost-effective procedure, that can be performed on an OPD basis, giving a preliminary diagnosis which can help in triaging the patients.6 Excisional biopsy is an invasive procedure done under anaesthesia and has a risk of complications.
This present study is a retrospective analysis of the diagnostic role and efficacy of FNAC performed in the pediatric LAP cases.
MATERIALS AND METHODS
This was a retrospective study carried out in the department of cytology of a tertiary care centre of eastern India, conducted over 2 years from August 2108 to August 2020. All the patients belonging to the pediatric age group (
RESULTS
Total of 235 pediatric cases presented to the cytology department with lymphadenopathy for FNAC. Out of these FNA procedures could not be done in case of 6 uncooperative patients. Hence FNA results of 229 patients were analyzed. Age of the patients ranged from 8 months to 18 years with a mean age of presentation being 11 years. On analysis of the age-wise distribution of cases, maximum no of cases was found to be in the age group of 11-15 years. (Figure1) There were 144 male and 85 female patients, with the male/female ratio being 1.69:1. The most common presentation was cervical lymphadenopathy seen in 202 cases (88.2%), followed by 9 cases of axillary LAP, 6 cases of inguinal LAP, 6 cases of generalized LAP, 5 cases of intra-abdominal LAP and 1 case of intra-mammary LAP which was present in the peri-areolar region. (Figure 2) Patients predominantly presented with multiple, non-tender lymph nodes in 145 casesand67 cases had a bilateral presentation. 84 cases presented with solitary lymphadenopathy. Tenderness was frequently observed in cases of suppurative lymphadenitis (LAN), which were also associated with tense swelling and erythema in the surrounding area. Multiple matted lymph nodes were seen in 11 cases, 3 of which had discharging skin sinuses. Commonly associated symptoms were fever, cough and sore throat. Other less common symptoms were loss of appetite, weight loss as in cases of Tuberculosis and malignancies. The size of the lymph nodes examined varied from 0.5 to 5 cm. The duration of presentation ranged from short duration of 2-3 days to long-standing LAP present for over 10 years. USG guided FNA was performed in 11 cases of deep-seated LAP, which posed with difficulty in approach during plain FNA. These included 6 cases with deep-seated cervical lymph nodes, 4 cases with mesenteric LAP and 1 case of external iliac LAP.
The FNA diagnoses were conclusive in 223 cases and in the rest 6 cases, the diagnoses were deferred due to inadequate material. The conclusive FNA diagnoses were broadly categorized into – benign and malignant. There were 217 benign diagnoses (97.3%) and 6 malignant diagnoses (2.7%). The benign diagnoses were further subdivided into- reactive LAN, necrotizing/granulomatous LAN, suppurative LAN and special reactive conditions like Rosai Dorfmann disease. The most common benign diagnosis was reactive hyperplasia (131), followed by necrotizing/granulomatous LAN (48), suppurative LAN (36) and Rosai Dorfmann disease (2). Malignant diagnoses included 4 cases of Hodgkin’s lymphoma, 1 case of metastatic Nasopharyngeal carcinoma and 1 case of metastatic Small round cell tumour. (Figure 3) The age-wise distribution of the cases according to FNA diagnoses was done. In the age groups of 0-5, 6-10 and 11-15 years, most common diagnosis was reactive hyperplasia whereas, in the age group 16-18 years, the commonest diagnosis was necrotizing/granulomatous LAN. (Figure 4)
In most cases of benign diagnoses, a biopsy was not performed, except for the 2 cases of Rosai Dorfman disease and2 cases of florid reactive hyperplasia. The biopsy was performed in all the 6 cases of malignancies. On the correlation of the FNA diagnoses with histopathology of 10 cases in which subsequent LN biopsy was performed, the results were concordant in 9 cases and discordant in 1 case, which was a false positive. Hence, accuracy was 90%, sensitivity was 100%, specificity was 80%, PPV was 83.33% and NPV was 100%
DISCUSSION
In our study, a male preponderance was noted with a male-to-female ratio of 1.2:1and the most common site of the presentation was the cervical region, which correlated with other studies.4,6 Benign disorders were more common than malignant disorders (13.67%) in the present study and the most common cause of lymphadenopathy was reactive hyperplasia followed by granulomatous LAN, which was comparable to the findings of other studies in cases LAP in all age groups done by Malhotra et al and in cases of pediatric LAP done by Lee et al, Sharma et al and Annam et al.4-7Our study showed that in <15 years age group most common cause of LAN was reactive hyperplasia and granulomatous LAN in >15 years age group. Many other studies from India, Pakistan, and Sudan, also reported tuberculosis as the most common cause of lymphadenopathy.8-12
In our study done on pediatric LAP cases also found results varying from benign to malignant. Though as per local demographic patterns, most cases belong to reactive hyperplasia followed by granulomatous LAN, few cases also showed malignant diagnosis, where FNA served as a simple, rapid and highly effective for diagnosis and further patient management.
Reactive Hyperplasia
FNA diagnosis of Reactive hyperplasia was given in 131 cases (58.74%) of which Florid reactive hyperplasia was seen in 5 cases. The lymph nodes were firm inconsistency with the average size of lymph nodes being 1.2 cm. The key cytological features that were seen in cases of reactive hyperplasia were a mixed population of lymphoid cells in different stages of maturation, comprised of mature lymphocytes, centrocytes, centroblasts, immunoblasts in a logical proportion along with the presence of plasma cells, histiocytes, tingible body macrophages and lympho-glandular bodies. (Figure 5A) 5 cases showed Florid reactive hyperplasia, 4 in cervical region and1 in the inguinal region, wherein the size of the lymph nodes varied between 1.5 to 3 cm and were advised to stay in follow up. Repeat FNA/Biopsy was advised in case the swelling did not reduce in size after a course of antibiotic therapy. Also seen in some cases were immunoblastic proliferation, may be attributable to viral infections.
Necrotizing/Granulomatous LAN
There were 52 FNA diagnoses (23.31%) of necrotizing/granulomatous LAN, of which epithelioid granulomas were seen in 20 cases, only necrosis was seen in 12 cases and both were seen in 15 cases. The average size of the lymph node at presentation was 1.5 cm, most of which had multiple and matted presentations. The key cytological feature looked for was the presence of epithelioid cell granulomas (figure 5B), histiocytes over a background of reactive lymphoid cells, with/without the presence of necrosis and multinucleated giant cells. When only necrosis has seen reactive lymphoid cells, a diagnosis of Necrotising LAN was given. (Figure5C) ZN stain for AFB was done in all the cases of granulomatous/necrotising LAN and5 cases of suppurative LAN (total 57 cases). ZN stain was positive for AFB in 17 cases in which case a diagnosis of Tubercular LAN was given. In the other AFB negative cases, the advice was given to investigate the patients in the line of tuberculosis with ancillary investigations including culture, CBNAAT and TB-PCR.
Suppurative LAN
There were 32cases (14.35%), which were given FNA diagnosis of suppurative LAN. The average size of the lymph node at presentation was 2 cm and the most commonly presented as a tense, tender or sometimes soft, cystic swelling. Local erythema and rise in temperature. Was also encountered in some cases. Commonly purulent material was aspirated. The cytological feature that clinched the diagnosis was a predominant population of polymorphs, admixed with lymphoid cells, degenerated cells and macrophages over a necrotic background. Slides were thoroughly scanned to look for the presence of epithelioid granulomas, in which case it would point towards granulomatous LAN with superadded suppuration. In such cases, ZN stain for AFB was performed to rule out tubercular aetiology. In other cases suggestion for culture correlation and follow-up was advised.
Rosai Dorfmann Disease
In our study, we found 2 cases (0.90%) of Rosai Dorman disease one of which was a 4-year male presenting with multiple bilateral cervical lymphadenopathies since 7 days, and other cases was a 15-year female presenting with single tender right axillary lymph node, noticed since 15 days. The average size of the lymph node was 3cm. In both cases, the FNA smears showed features of Reactive hyperplasia with the presence of the good number of macrophages, evidence of emperipolesis and plasma cells favouring the diagnosis of Rosai Dorfman disease. The biopsy was done in both the cases and histopathology gave a concordant diagnosis. (Figure5D)
Malignancies
A total of 6 malignancies were diagnosed by FNA during this period. These included 4 cases of Hodgkin’s lymphoma (1.80%), 1 case of metastatic nasopharyngeal carcinoma (0.45%) and 1 case of metastatic Small round cell tumour (0.45%).
All the 4 cases of Hodgkin’s lymphoma presented with bilateral cervical LAN, which were firm, rubbery inconsistency, and the average size was 3.5 cm. the age of these patients ranged from 13-18 years of age. The classical cytological features that clinched the diagnosis were the presence of large atypical mononuclear to multinucleate cells and multilobulated cells, with prominent nucleoli, resembling RS cells, on a background of reactive lymphoid cells, eosinophils, plasma cells and histiocytes. (Figure6A, 6B) All 4 of these cases underwent biopsy of which 3 showed concordance and 1 case was false positive, in which an FNA diagnosis of Lymphoproliferative disorder with associated granulomatous reaction was given and in-toto lymph nodal excisional biopsy was advised to rule out the possibility of Hodgkin’s lymphoma. The cause of suspicion was the presence of a few large cells with bi-nucleation at places, prominent nucleoli and abundant cytoplasm, along with the presence of occasional eosinophils. But on histopathology, a final diagnosis of Granulomatous LAN was given, rendering a false positive discordant diagnosis. Immunohistochemistry was done in the concordant cases with lymphoma panel. 2 cases were given the final histopathological diagnosis of Hodgkin’s lymphoma, mixed cellularity type, and 1 case was given the final histopathological diagnosis of Lymphocyte rich Hodgkin’s lymphoma.
A 12-year female presented with bilateral cervical LAN, largest measuring 3x2.5 cm right post-auricular region for 11 months. A previous FNA done outside had given a diagnosis of granulomatous LAN, possibly tubercular and the patient had completed ATT for 6 months. On doing FNA from bilateral cervical lymph nodes in our institute, we saw large neoplastic cells with high N: C ratio and prominent nucleoli, arranged in fibrous strands and occasional acini. (Figure6C, 6D) A diagnosis of Metastatic Nasopharyngeal carcinoma was given which was later confirmed with a biopsy.
A 1-year-old male child presented with a 1.5 cm left posterior cervical lymph node which on FNA yielded richly cellular smears showing monotonous round cells in singles, sheets and fragments with focal rosettoid arrangement. These cells had high N: C ratio, finely granular chromatin, mild nuclear irregularity and scant cytoplasm. An FNA diagnosis of Small round cell tumour was given. On biopsy, we received a lymph node, which on subsequent histopathology showed near-total replacement of the LN by tumour tissue comprised of round to polygonal neoplastic cells arranged in an alveolar pattern and after Immunohistochemical positivity with Myo-D1, the final histopathological diagnosis of Alveolar Rhabdomyosarcoma was given. (Figure 6E, 6F)
On comparison with final histopathology of the LN biopsies in the 10 cases in our study, we observed that FNAC had an accuracy of 90%, sensitivity of100%, the specificity of 80%, PPV of 83.33% and NPV of 100%which was comparable with the findings of Lee et al, who reported an accuracy of 94.5%, the sensitivity of 100%, PPV of 93.3%, for pediatric cervical lymphadenopathy.4 In a study on the profile of lymphadenopathy by FNAC, Malhotra et al reported accuracy of 91.15%, the sensitivity of 94.49%, PPV of 96.26%.5 Hafez et al reported an overall diagnostic accuracy of 82.2%, the sensitivity of 90.9%, the specificity of 67.2%, PPV 82.6% and NPV of 81.3% in FNAC of cervical lymph nodes.13
CONCLUSION
LAP can be a manifestation of a myriad of underlying local or systemic diseases. Being mostly superficial and well localized, it is very approachable for simple procedures like FNAC, thus making it a widely used practice for initial evaluation of cases. FNAC is a simple, cost-effective, minimally invasive and reliable technique to provide a rapid diagnosis in the majority of cases of pediatric LAP and helps in the screening of the cases to allows the clinicians to take the timely decision on the course of action. Thus it helps to avoid unnecessary invasive procedures like excisional biopsy in pediatric age group, which is associated with its complications. LAP in the pediatric population in our study is mainly due to reactive hyperplasia, most of which responded to therapy, and did not require repeat FNAC/biopsy. Granulomatous/necrotizing LAN also accounted for a large number of cases and were the 2nd most common cause of pediatric LAP, owing to the increased prevalence of Tuberculosis. Amongst the malignancies causing LAP, Hodgkin’s Lymphoma was the most common cause. However, some rare cases of metastasis of Nasopharyngeal carcinoma and Alveolar Rhabdomyosarcoma also accounted for LAP in 1 case each. In the cases where the biopsy was performed, in comparison to histopathology, the FNAC results were very accurate. With an adequate correlation of clinical-radiological and other laboratory findings, FNAC is a very reliable screening and diagnostic tool in the cases of Pediatric LAN. However, considering the broad spectrum of etiologies a high degree of suspicion, along with adequate history needs to be kept in mind, while dealing with cases of pediatric LAP.
Conflict of interest: Nil.
Financial support : Nil.
Authors’ Contribution: AL-concept, design, manuscript writing, editing, final approval, literature search. MR- concept, design, manuscript writing, editing, literature search, drafting, data acquisition. SP- clinical studies, data acquisition.
ACKNOWLEDGMENT: The author acknowledges the help received from Professor and Head, Department of for her guidance. I am also thankful to my colleagues and postgraduates for their kind co-operation. I would like to give my special thanks to all the technicians and staff of cytology and histopathology section, for helping me while conducting the present study. The author is also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed, discussed and cited.
ABBREVIATIONS
AFB- Acid-fast bacilli
DQ- Diff quick
FNA- Fine needle aspiration
FNAC- Fine needle aspiration cytology
HE- Hematoxylin and eosin
LAP- Lymphadenopathy
LAN- Lymphadenitis
LN- Lymph Node
ZN- Ziehl Neelsen
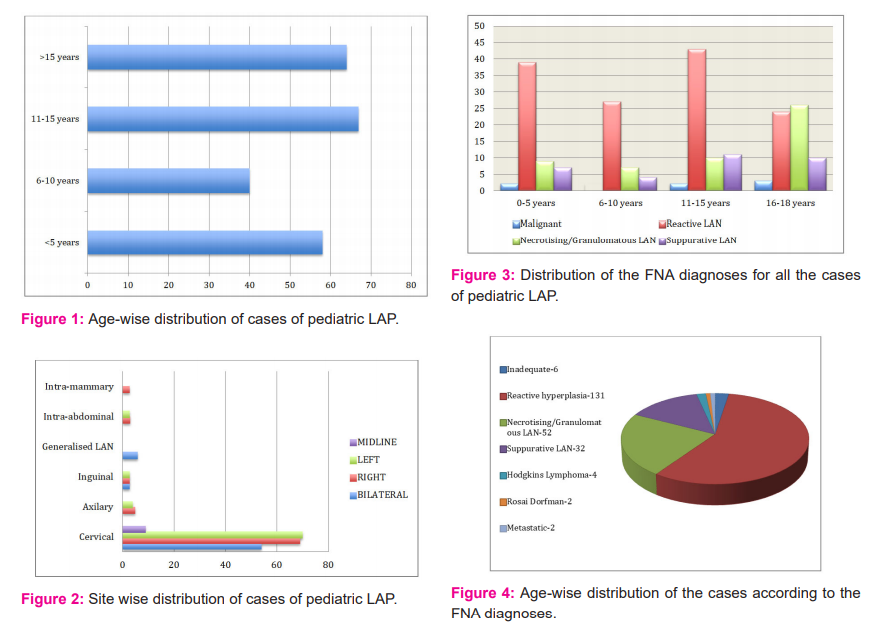
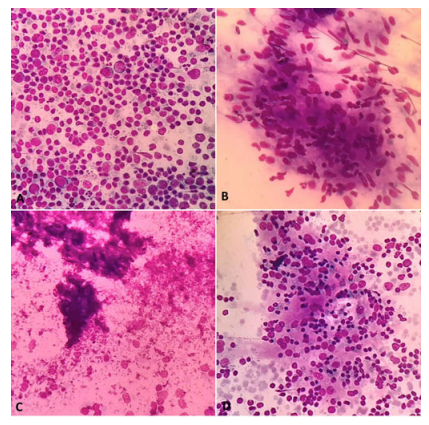
Figure 5: A. Reactive hyperplasia, showing lymphoid cells in different stages of maturation in logical proportion. (DQ, x400); B. Granulomatous lymphadenitis, showing epithelioid granuloma. (DQ, x400); C. Necrotising Lymphadenitis, showing areas of necrosis. (DQ, x400); D. Rosai Dorman’s Disease, Histiocytes showing emperipolesis. (DQ, x400)
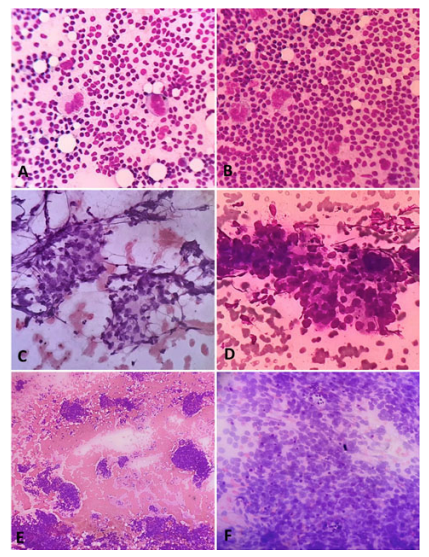
Figure 6. A. Hodgkin’s Lymphoma, showing RS cells. (DQ, x400); B. Hodgkin’s Lymphoma, showing RS cells. (DQ, x400); C. Metastatic Nasopharyngeal Carcinoma, showing tumor fragments. (HE, x400); D. Metastatic Nasopharyngeal Carcinoma, showing acini. (DQ, x400); E. Metastatic small round cell tumor, showing tumor cells in singles, fragments and sheets. (DQ, x100); F. Metastatic small round cell tumor, high power showing high N:C ratio, granular chromatin, scant cytoplasm. (DQ, x400)
References:
-
-
-
-
Rajasekaran K, Krakovitz P. Enlarged neck lymph nodes in children. Pediatr Clin 2013;60(4):923-936.
-
Twist CJ, Link MP. Assessment of lymphadenopathy in children. Pediatr Clin 2002;49(5):1009-1025.
-
Leung AK, Robson WL. Childhood cervical lymphadenopathy. J Pediatr Health Care 2004;18(1):3-7.
-
Lee DH, Baek HJ, Kook H, Yoon TM, Lee JK, Lim SC. Clinical value of fine-needle aspiration cytology in pediatric cervical lymphadenopathy patients under 12-years-of-age. Int J Pediatr Otorhinolaryngol 2014;78(1):79-81.
-
Malhotra AS, Lahori M, Nigam A, Khajuria A. Profile of lymphadenopathy: An institutional-based cytomorphological study. Int J Appl Basic Med Res 2017;7(2):100.
-
Sharma M, Gupta A, Kaul R. Pediatric Lymphadenopathy: Cytological Diagnosis over Two Years in a Rural Teaching Hospital. Ped Health Res 2017;2(3):16.
-
Annam V, Kulkarni MH, Puranik RB. Clinicopathologic profile of significant cervical lymphadenopathy in children aged 1–12 years. Acta Cytologica 2009;53(2):174-178.
-
Nidhi P, Sapna T, Shalini M, Kumud G. FNAC in tuberculous lymphadenitis: Experience from a tertiary level referral centre. Indian J Tuberc 2011;58(3):102-107.
-
Ageep AK. Assessment of adult peripheral lymphadenopathy in Red Sea State, Sudan. Int J Trop Dis Health 2012;2:24-32.
-
Fatima S, Arshad S, Ahmed Z, Hasan SH. The spectrum of cytological findings in patients with neck lymphadenopathy-experience in a tertiary care hospital in Pakistan. Asian Pac J Cancer Prev 2011;12(7):1873-1875.
-
Khajuria R, Goswami KC, Singh K, Dubey VK. The pattern of lymphadenopathy on fine-needle aspiration cytology in Jammu. JK Sci 2006 Jul;8(3):157-159.
-
Shahid F, Mirza T, Mustafa S, Sabahat S, Sharafat S. An experiential status of fine-needle aspiration cytology of head and neck lesions in a tertiary care scenario. J Basic App Sci 2010;6(2).
-
Hafez NH, Tahoun NS. Reliability of fine-needle aspiration cytology (FNAC) as a diagnostic tool in cases of cervical lymphadenopathy. J Egypt Nat Cancer Inst 2011;23(3):105-114.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





