IJCRR - 13(4), February, 2021
Pages: 33-38
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
Effectiveness of Cytological Scoring Systems for Evaluation of Breast Lesion Cytology with its Histopathological Correlation
Author: Anu, Sweta, Uma Sharma
Category: Healthcare
Abstract:Introduction: Fine needle aspiration cytology (FNAC) is a rapid and inexpensive technique for the diagnosis of breast lesions. Various cytological grading systems are being used for categorisation. For better advancement of categorization and management of breast lesions Modified Masood scoring system has been proposed. Objective: To study the effectiveness and accuracy of Modified Masood Scoring Index (MMSI) and Robinson's cytological grading for evaluation of breast lesions with their histopathological correlation. Methods: A prospective study was conducted in a tertiary care hospital from September 2019 to February 2020. A total of 73 cases were included in the study which had undergone FNAC and had histopathological samples as excision biopsy and mastectomy. The cytological smears were categorised by using MMSI, Robinson's cytological grading system and were compared with the histological findings (the four categories of MMSI) and for carcinoma, cases modified Scarff\?Bloom\?Richardson's scoring system was used. Results: The sensitivity, specificity, Positive predictive value (PPV), Negative predictive value (NPV) and diagnostic accuracy of MMSI were 76.4%, 100%, 100%, 93.3% and 94.5% respectively. The Robinson's grading had sensitivity, specificity, PPV, NPV and diagnostic accuracy of 88.2%, 100%, 100%, 96.5% and 97.2% respectively. Conclusion: Robinson's cytological grading had good sensitivity for evaluation of malignant lesions whereas MMSI can be used for the categorization of both benign and malignant breast lesions with good sensitivity.
Keywords: Biopsy, Breast aspiration cytology, May Grunwald-Giemsa stain, Modified Masood scoring index, Robinson’s grading system
Full Text:
INTRODUCTION
Fine needle aspiration cytology (FNAC) is a simple rapid, minimally invasive, cost-effective technique for evaluation of palpable breast lesions. It is a safe technique to distinguish non-neoplastic breast lesions from neoplastic lesions. Breast carcinoma is the second most common cancer in women in developing countries. FNAC is an important part of Triple test which is used for assessment of breast lesions.1 Despite good diagnostic accuracy, the cytological scoring systems are not used in many tertiary care centres. There are various cytological grading systems which can be used for evaluation of breast lesions which helps the surgeons to decide the treatment.2 The Bethesda System of reporting breast FNAC to categorise the breast lesions based on morphology and arrangement of cells, nuclear features, mitotic figures and the background of smear into 5 categories (Table 1). unsatisfactory, benign lesions, atypical or intermediate, suspicious for malignancy and malignant lesions.3 The Robinson scoring system is the most commonly used cytological grading system. This grading is based on cellular dissociation, cell uniformity, nuclear size, nuclear margin, nucleoli and chromatin pattern.4 Before Robinson’s grading system, Masood Scoring Index (MSI) was developed in 1990 for breast aspiration cytology. Despite its diagnostic accuracy this is not commonly used by cytopathologists. This grading was based on cellular arrangement, cellular anisonucleosis and pleomorphism, the myoepithelial cells, presence of nucleoli and the chromatin pattern. For each criterion, 1-4 scores were given and the total score was calculated by adding all numbers. The final score was ranging from a minimum of 6 to a maximum of 24 scores. Based on scores further, categorisation was done into non-proliferative breast lesions (6-10), proliferative breast lesion without atypia (11-14), proliferative breast lesion with atypia (15-18) and carcinoma (19-24).5 Nandini el al. further modifies the MSI scoring of non-proliferative breast lesion from 6-10 to 6-8 score and proliferative breast disease without atypia from 11-14 to 9-14 (Table 2). This was named as Modified Masood scoring Index (MMSI). After this change, the diagnostic accuracy was significantly improved.6
Considering this change in diagnostic accuracy the MMSI system was used in our study to evaluate the cytological breast aspirate for the categorisation of lesions along with Robinson’s scoring system. The sensitivity, specificity, positive predictive value, negative predictive value and the diagnostic accuracy was calculated by comparing with the histopathological findings and modified Scarff–Bloom–Richardson’s scoring system for carcinomas.
MATERIALS AND METHODS
The prospective cross-sectional study was conducted on the patient who presented with palpable breast lump in the Department of Surgery referred to the Department of Pathology, Shree Guru Gobind Singh Tricentenary Medical College during the period of 6 months, from September 2019 to February 2020. The inadequate aspirate and cases without histopathology specimen were excluded from the study. The ethical clearance number was SGT/FMHS/F/1/9/20-3. For the adequacy of smear, the minimum four clusters of ductal epithelial cells with each cluster having five to six cells were taken.
After explaining the procedure of Fine needle aspiration cytology (FNAC) to the patient written consent was taken from every patient. The detailed history was taken from the patient with USG findings if available. After locating and fixing the lesion FNAC was carried out under strict aseptic precautions with 22 gauge needle and 10 ml syringes. The slides were prepared and air-dried for May-Grunwald-Giemsa (MGG) staining. The stained smears were then categorised by using MMSI (Table 2) and Robinson’s scoring (Table 3).
The breast tissue after excision biopsy and mastectomy were sent from the Surgery Department fixed in formalin. The tissue sections were prepared and stained with Haematoxylin and Eosin. The sections were categorised into four histopathological categories on basis of modified Scarff–Bloom–Richardson’s scoring system (Table 4) to compare with MMSI and Robinson’s scoring for carcinomas. The cytological and histopathological findings were correlated.
The categorical type of data was collected and the statistics of all data were shown in the form of proportions and or percentages. The diagnostic accuracy of MMSI and Robinson’s cytological scoring was calculated. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated by comparing with the gold standard histopathological findings. To assess the agreement between the MMSI cytological scoring, Robinson’s scoring with their histopathological findings and modified Scarff–Bloom–Richardson’s scoring system, Cohen’s kappa coefficient was calculated.
RESULTS
During six months, out of 153 breast FNAC cases, 73 were included in our study as the histological specimens were available of only these cases in form of Tru-cut biopsy, lumpectomy or mastectomy. Other breast FNAC cases without histological specimens or with inadequate material were excluded from the study.
The mean age of female was 35.6 years with the range from 16-75 years. The maximum of cases was in the age group of 31-40 years. Most of the cases were presented with unilateral breast swelling.
As per MMSI, the concordance between cytopathological and histopathological diagnosis for non-proliferative breast disease was 100% and for proliferative breast disease without atypia (Figure 1A & 2A) was 92.5% with histopathology (Figure 1B & 2B) and 7.5% of cases were confirmed as malignant on histopathology. For proliferative breast disease with atypia, concordance was 75% whereas category 4 of carcinoma-in-situ (CIS) and carcinoma (Figure 3A) showed 100% concordance with histopathology (Figure 3B, Table 5).
As per the result obtained with MMSI a 2x2 table was made and the diagnostic accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated (Table 6). The diagnostic accuracy was 94.5% with a sensitivity of 76.4%, specificity of 100%. The PPV and NPV were 100% and 93.3% respectively.
As per Robinson’s scoring for carcinoma (Figure 3A) 15 cases out of 73 were diagnosed as carcinoma which was then graded with the modified Scarff–Bloom–Richardson’s scoring system of histopathology (Figure 3B). In grade 1, there was 100% concordance with histopathology grading whereas, in grade 2, four cases out of nine showed discrepancy, on histopathological grading three cases were of grade 3. Five cases were categorised as grade 3 on cytological scoring, out of them one was of grade 2 on histopathology (Table 7).
As per the result obtained a 2x2 table was made and the diagnostic accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated (Table 8). The diagnostic accuracy was 97.2% with a sensitivity of 88.2%, specificity of 100%. The PPV and NPV were 100% and 96.5% respectively (Table 9).
Based on the overall presence or absence of carcinoma, Cohen’s kappa coefficient was calculated to assess the MMSI and Robinson’s cytological scoring with their histopathological diagnosis, which was 0.828 (approximately 83%) and 0.916 (approximately 92%) respectively.
DISCUSSION
FNAC plays an important role in the assessment of breast lumps and helps the surgeon to further decide the management. Various cytological scoring systems are used to categorize breast lesions. In Masood scoring index, total score from 6 to 24 was given based on cytological category. Proliferative breast disease (PBD) increases the risk of development of breast carcinoma. The risk of breast carcinoma increases by 1.3 folds in PBD without atypia and 4.3 folds in PBD with atypia.1 In non-PBD, cells are arranged in monolayer with no cytological abnormalities. In PBD without atypia, the cells are arranged in sheets with nuclear overlapping and overcrowding at places. In PBD with atypia, tightly packed clusters of cells are present with marked nuclear overlapping and prominent nucleoli. In malignant lesions, the cells are loosely arranged with marked nuclear pleomorphism with irregular nuclear membrane, coarsely clumped chromatin and prominent macronuclei. Myoepithelial cells are absent in malignant lesions. To differentiate the benign lesions from malignant lesions myoepithelial cells played an important role.5
Nandini et al. 2011 conducted a study on 100 cases and observed that the diagnostic accuracy was increased when 9 and 10 scores were shifted from category 1 of non-proliferative breast disease to category 2 of proliferative breast disease without atypia. This change was important as category 2 and category 1 have different prognostic value.1 Robinson’s scoring system is used for the categorisation of carcinoma cases this scoring system is based on the cellular arrangement, cellular morphology and the nuclear details.4 The modified Scarff–Bloom–Richardson’s scoring system of histopathology is based on the tubular formation, nuclear pleomorphism and the number of mitotic figures. All these have features have prognostic values.
So in our study, we used both MMSI and Robinson’s scoring system to assess the accuracy whether this can be used for assessment of the risk of developing breast carcinoma in palpable breast lump and calculate the concordance by comparing with the histopathological diagnosis. From our result this was found that with MMSI, the maximum concordance of 100% was observed in category 1 of non proliferative breast disease and category 4 of carcinoma in-situ/carcinoma followed by category 2 of proliferative breast disease without atypia and minimum concordance of 75% was observed in category 3 of proliferative breast disease with atypia.
The sensitivity and specificity of MMSI was 76.47% and 100% respectively with 100% positive predictive value and 93.33% negative predictive value with a diagnostic accuracy of 94.5%, similar results were found previously.2 Out of 73 cases, 15 were diagnosed as carcinoma on cytology and were categorized by using Robinson’s grading system. Out of 15, one case was graded as grade 1 which was confirmed by using modified Scarff–Bloom–Richardson’s scoring. Nine cases were graded under grade 2, out of which three cases were graded under grade 3 on modified Scarff–Bloom–Richardson’s scoring and 1 was invasive lobular carcinoma. Five cases were graded as grade 3 on Robinson’s out of which three were confirmed as grade 3, one was grade 2 on modified Scarff–Bloom–Richardson’s scoring and one case were diagnosed as invasive papillary carcinoma. So the overall concordance was 60%. Robinson et al. had 57% of concordance whereas similar studies had 71.2%, 64%, 77.19%, 72.2% and 63.3% of concordance.4,12-15
Further slides with more number of cases should be done to standardize the categorical grading system which helps in categorizing benign and malignant breast lesion. This will help the surgeons to plan the treatment and to predict the prognosis of the disease.
CONCLUSION
Our study concluded that cytological scoring systems must be used for the evaluation of all breast FNAC cases. The MMSI for categorisation of benign and malignant lesions and Robinson’s for grading of breast carcinoma cases. These cytological scoring systems have good sensitivity, specificity, PPV and NPV with the good concordance with histopathological diagnosis.
Acknowledgement- None
Conflicting Interest- There are no conflicts of interest.
Financial Support and Sponsorship- Nil
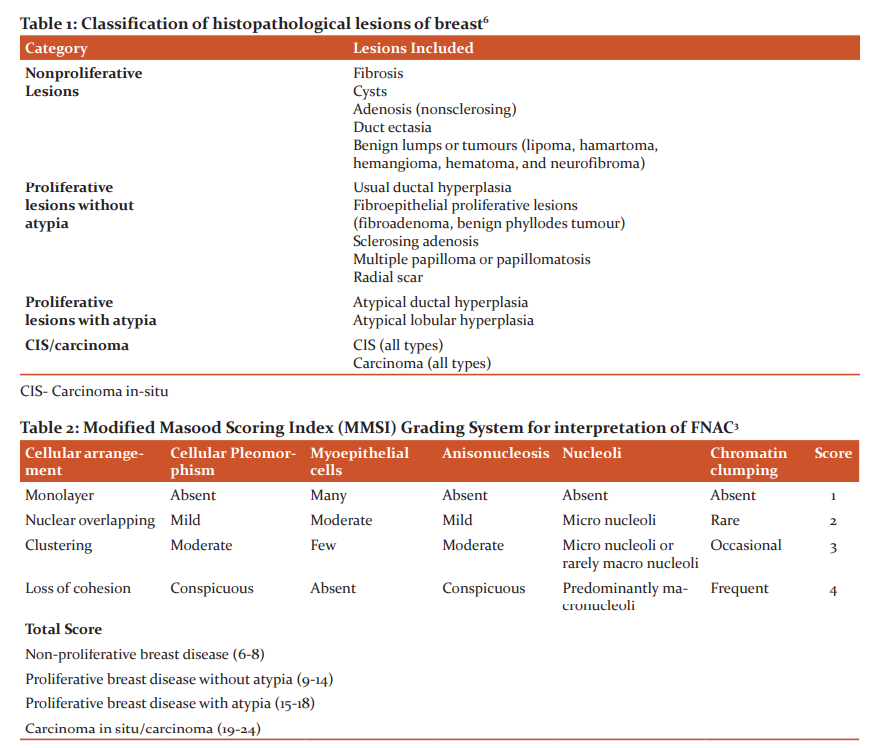
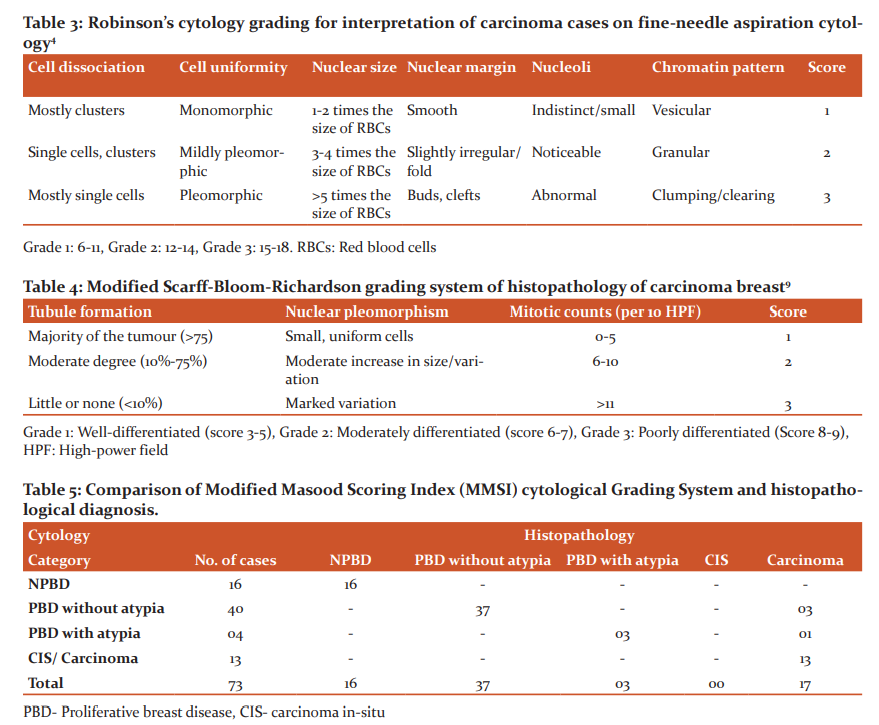
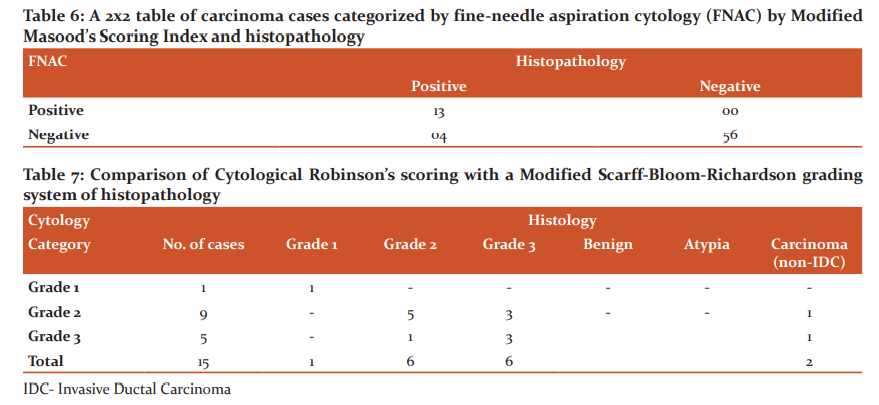
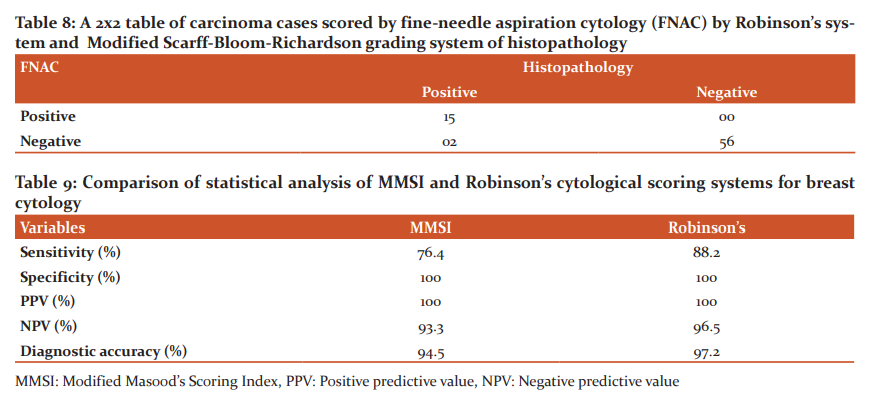
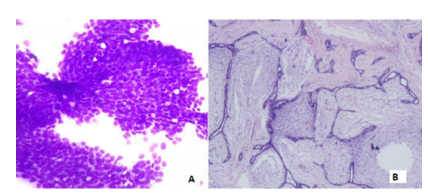
Figure 1: A. Monomorphic ductal epithelial cells in the cluster with many scattered myoepithelial cells (MGG, 400x), B- Corresponding histopathological lesion diagnosed as Fibroadenoma (H&E,40x)
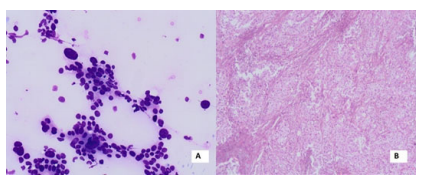
Figure 2: A- Tightly cohesive ductal epithelial cells with spindle shaped myoepithelial cells with stroma (MGG,40x) B- Corresponding histopathological lesion diagnosed as Phyllodes (H&E,40x)
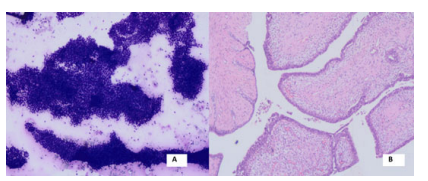
Figure 3: A- Loosely cohesive pleomorphic ductal epithelial cells with high N: C ratio (MGG 100x) B- Corresponding histopathological lesion diagnosed as Invasive ductal carcinoma with >75% tubule formation (H&E,40x)
References:
1. Nandini NM, Rekha TS, Manjunath GV. Evaluation of scoring system in cytological diagnosis and management of breast lesion with the review of the literature. Indian J Cancer 2011;48:240–245.
2. Raju K, Rajanna VS. A comparative study of three scoring systems on palpable breast aspirates at a tertiary health-care centre. A cross-sectional study. J Nat Sci Biol Med 2020;11:21-26.
3. Bansal C, Pujani M, Sharma KL, Srivastava AN, Singh US. Grading systems in the cytological diagnosis of breast cancer: a review. J Cancer Res Ther 2014;10(4):839-845.
4. Robinson IA, McKee G, Nicholson A, D'Arcy J, Jackson PA, Cook MG et al. Prognostic value of cytological grading of fine-needle aspirates from breast carcinomas. Lancet 1994;343:947-949.
5. Masood S. Cytomorphology of fibrocystic change, high-risk proliferative breast disease and premalignant breast lesions. Clin Lab Med 2005;25:713-731.
6. Cherath SK, Chithrabhanu SM. Evaluation of Masood's and Modified Masood's Scoring Systems in the Cytological Diagnosis of Palpable Breast Lump Aspirates. J Clin Diagn Res 2017;11(4): EC06-EC10.
7. Masood S, Frykberg ER, McLellan GL, Scalapino MC, Mitchum DG, Bullard JB. Prospective evaluation of radiologically directed fine-needle aspiration biopsy of nonpalpable breast lesions. Cancer 1990;66:1480-1487.
8. Masood S, Frykberg ER, McLellan GL, Dee S, Bullard JB. Cytologic differentiation between proliferative and non-proliferative breast disease in mammographically guided fine-needle aspirates. Diagn Cytopathol 1991;7:581-590.
9. Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991;19:403-410.
10. Rekha TS, Nandini N, Dhar M. Expansion of Masood's Cytologic Index for breast carcinoma and its validity. J Cytol 2013;30:233-236.
11. Das AK, Kapila K, Dinda AK, Verma K. Comparative evaluation of grading of breast carcinomas in fine-needle aspirates by two methods. Indian J Med Res 2003;118:247-250.
12. Lingegowda JB, MuddeGowda PH, Ramakantha CK, Chandrasekar HR. Cytohistological correlation of grading in breast carcinoma. Diagn Cytopathol 2011;39:251-257.
13. Saha K, Raychaudhuri G, Chattopadhyay BK, Das I. Comparative evaluation of six cytological grading systems in breast carcinoma. J Cytol 2013;30:87-93.
14. Phukan JP, Sinha A, Deka JP. Cytological grading of breast carcinoma on fine-needle aspirates and its relation with histological grading. South Asian J Cancer 2015;4:32-34.
15. Srivastava P, Kumar B, Joshi U, Bano M. To evaluate the applicability of parameters of cytological grading systems on aspirates of breast carcinoma. J Cytol 2018;35:15-21.
16. Dawande P, Bhatt N, Noman O, Bahadure S, Bhake A. Correlation between cytological and histological grading of breast cancer and its utility in patient’s management. Int J Curr Res Rev 2020;12(14):71-76.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





