IJCRR - 13(4), February, 2021
Pages: 13-18
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
Anterior Resection (AR) versus Abdominoperineal Resection (APR) Technique in Patients Undergoing Oncogenic Resection of the Rectum for Quality of Life (QOL) Assessment: A Retrospective, SingleCentre, Observational Study
Author: Quresh Bambora, Mangesh Shingade, Aarti Gupta, Aditya Agarwal
Category: Healthcare
Abstract:Introduction: The prevalence of rectal cancer is very high and it is the third most common cancer in male and second in women. Objective: The present study aimed to compare Quality of life (QOL) parameters in patients who had undergone oncogenic resection of the rectum with three different surgical techniques i.e., Abdominoperineal Resection (APR), High Anterior Resection (HAR) and Low Anterior Resection (LAR) of the rectum. Methods: Patients were given the Short Form 36 (SF-36), The European Organization for Research and Treatment of CancerQuality of Life Questionnaire (EORTC QLQ)- C30 and C29 to fill at three-time points in their treatment (before surgery, 3 months and 6 months following surgery). The prospectively collected questionnaires were analyzed retrospectively. Results: On comparing the SF-36 questionnaire, there was no significant difference between patients who underwent all three types of surgeries except for general health which was better in patients undergoing APR and HAR. While comparing EORTC-30 questionnaire, patient undergone APR did well in terms of physical functioning and emotional well-being, while those undergone HAR did well in terms of GI-related complaints. On Comparing EORTC-29 questionnaire, micturition complaints and perception of body image were worst for the patient undergoing APR as compared to LAR. Conclusion: Quality of life as against assumption to be better in patients who had undergone AR, but after overcoming the trauma of surgery and its immediate implications, patients who underwent APR behaved almost equivalent to patients who underwent AR.
Keywords: Quality of Life (QOL), Rectal Cancer, High Anterior Resection (HAR), Low Anterior Resection (LAR), Abdominoperineal Resection (APR)
Full Text:
Introduction
Carcinoma of the rectum is one among the quite common malignancies worldwide and it continues to be a major health-related concern in both the western world and the developing nations. Amongst them, the prevalence of rectal cancer is very high and it is the third most common cancer in male and second in women.1 The main treatment option available is surgery with or without radiotherapy. From quite a long-time surgery had been one of the main constituents of the multi-modality approach of the disease. Among surgical techniques, anterior resection (AR) and Abdominoperineal Resection (APR) are the two standard procedures followed worldwide.
Surgeons have to consider not only the surgical methods for treating low rectal cancer but also the QoL after surgery. The main factors determining the patient quality of life seems to be an operation technique, the level of resection, the presence of a stoma following surgery and whether the stoma is temporary or permanent. Injury to the nerves controlling bladder, bowel, and sexual organs, is a major concern during resection of rectal cancer. In addition to endpoints of cancer such as survival and complications, comparison of QOL measurements are not widely used in clinical practice and the effect of different methods of surgery on the quality of life is not known.
A large number of studies had been performed so far looking into issues regarding the quality of life in patients operated for rectal cancer using standard techniques of AR and APR, however, the comparison between different surgical methods from QOL perspective is hardy available.2 In addition to helping patients evolve realistic expectations, it will help clinicians identify those for whom these interventions may be appropriate.
Materials and Methods
The present study planned with the primary objective of a retrospective analysis of a prospectively collected Quality of Life questionnaires to compare Quality of Life (QOL) in patients who have undergone oncologic resection of the rectum with Low Anterior Resection (LAR), High Anterior Resection (HAR) and Abdominoperineal Resection (APR) surgical methods.
After taking prior approval from Institutional Ethics Committee, patients undergoing surgery for rectal cancer at Tata Memorial Hospital (TMH) between September 2010 to September 2012 were asked to enrol in the study. The patient was informed about the study details and those who were willing to participate in the study were given the Short Form 36 (SF-36),3 the European Organization for Research and Treatment of Cancer (EORTC) QLQ-C30 and the EORTC QLQ-C29 questionnaires4 to fill at three-time points in their treatment (before surgery, 3 months and 6 months following surgery). The forms were submitted and collected prospectively during the hospital stay and subsequently at each follow-up visit. The collected questionnaires were retrospectively audited. The questionnaires were self-administered in three languages – Hindi, Marathi and English.
The analysis of QOL data included all patients with localized non-metastatic rectal cancer who were operated either upfront or post-neo-adjuvant chemoradiation at TMH. The excluded patients were who had two or more uncontrolled co-morbidities falling into the American Society of Anesthesiologists (ASA)5 category 3 or 4, patients whose disease was invading other pelvic or abdominal organs even after completion of neoadjuvant therapy (T4 tumours), patients who underwent simultaneous resection of metastatic disease, patients who were not able to fulfil regular follow-up schedule, patients undergoing surgery for recurrent disease and illiterate patients who were not able to read and understand the questionnaires.
The main outcome will be quality of life was assessed using the questionnaires of quality of life analysis - European Organization for Research and Treatment of Cancer (EORTC) QLQ-C30 and QLQ – C 29 and QLQ SF-36 questionnaire for comparison of study for improvement in physical, intellectual/cognitive, emotional, and social domains scores.
Scales computed for each domain score were presented as mean (S.D), median. Group comparisons Low Anterior Resection (LAR), High Anterior Resection (HAR) and Abdominoperineal Resection (APR) for rectal cancer were made using Analysis of variance or Kruskal Wallis test as per the distribution of the data. Change in scores from baseline to follow up visit were compared using Paired T-test or Wilcoxon signed rank-sum test as per the distribution of data. Categorical variables were analyzed using the Chi-square test or Fisher’s exact test. P-value < 0.05 was considered statistically significant.
Results
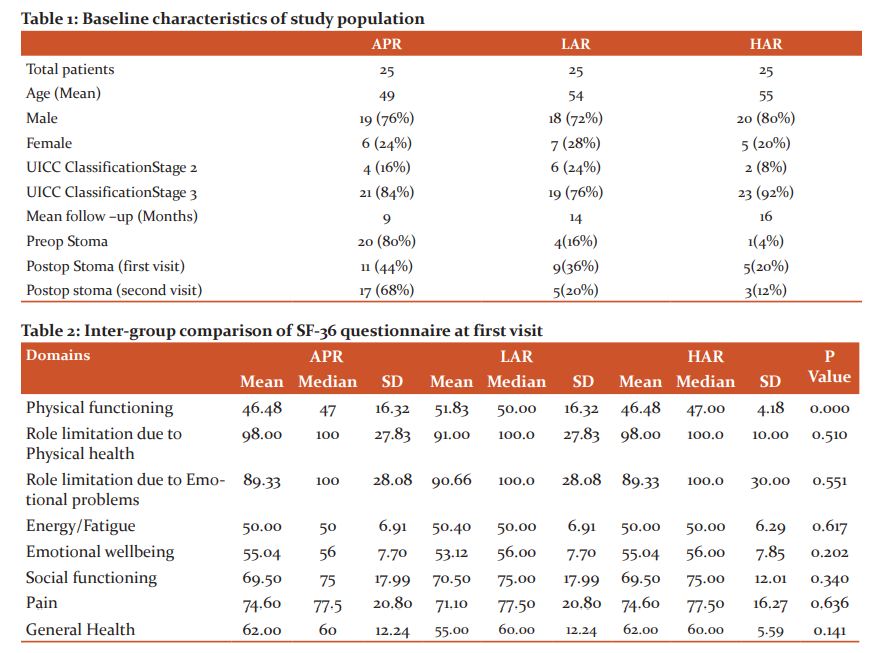
During the study period of two years, a total of 176 patients were operated in TMH for carcinoma rectum of which QOL questionnaires filled by 75 patients were retrospectively audited, wherein mean age of patients who had undergone APR was 49, LAR was 54 and HAR were 55. Male to female ratio on an average for all the arms was around 3-4 (Table-1).
Out of 25 patients in APR arm, 84% were stage 3 and 16% stage 2. In LAR arm, 76% were stage 3 and 24% stage 2 and in the HAR arm 92% were stage 3 and 8% were stage 2. Thus, on an average of 75 to 90% of patients belonged to stage 3 and 10 to 25% to stage 2. Mean follow up of patients was around 13 months. In the LAR arm, 16% of patient underwent pre-op stoma, 36% of patients had a stoma at first and 20% at the second visit. In the HAR arm, 4% had a pre-op stoma and 20% had a stoma at first and 12% second visit.
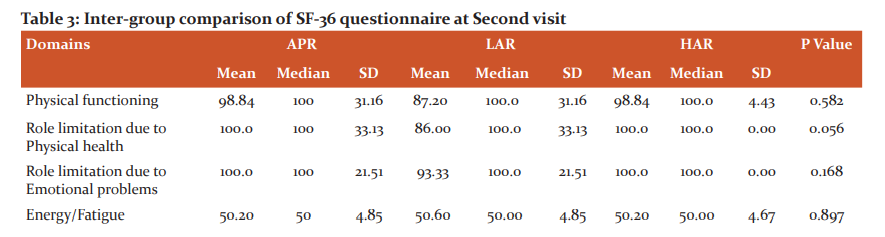
SF 36 Questionnaire was divided into 8 health domains, each domain containing a certain number of questions and a two-step statistical analysis was done with the calculation of P-value. An intergroup comparison was done at the first and second visit. At the first visit, there was a significant difference between physical functioning, patients who underwent low AR showing better results than who underwent APR and high AR, while at second visit there was no significant difference between patients who underwent all three types of surgeries except for general health which was better in patients undergoing APR and high AR. (Table 2 and 3).
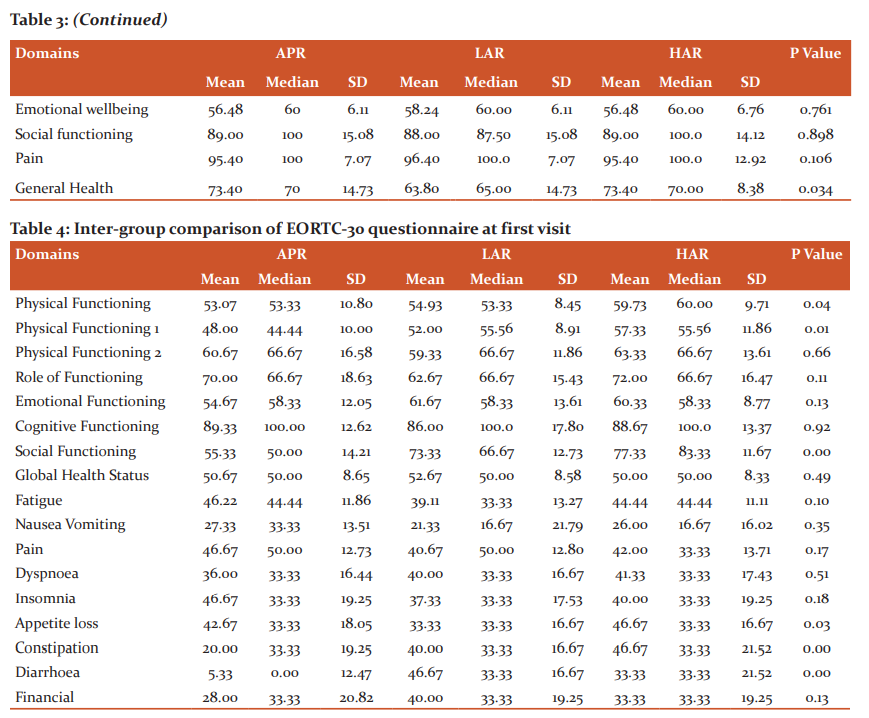
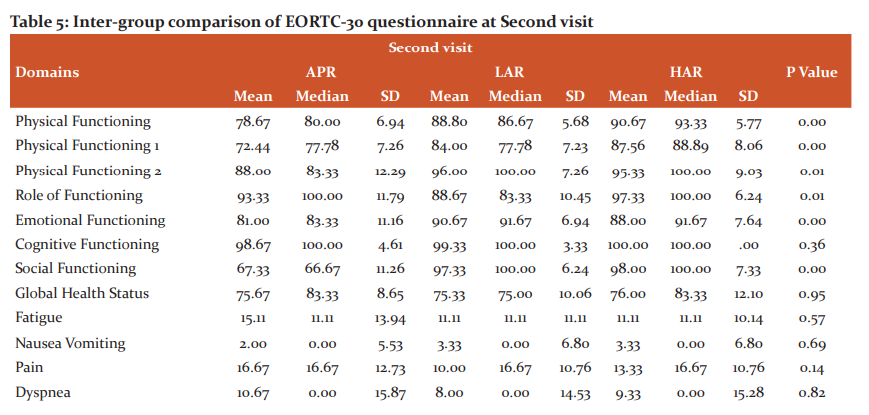
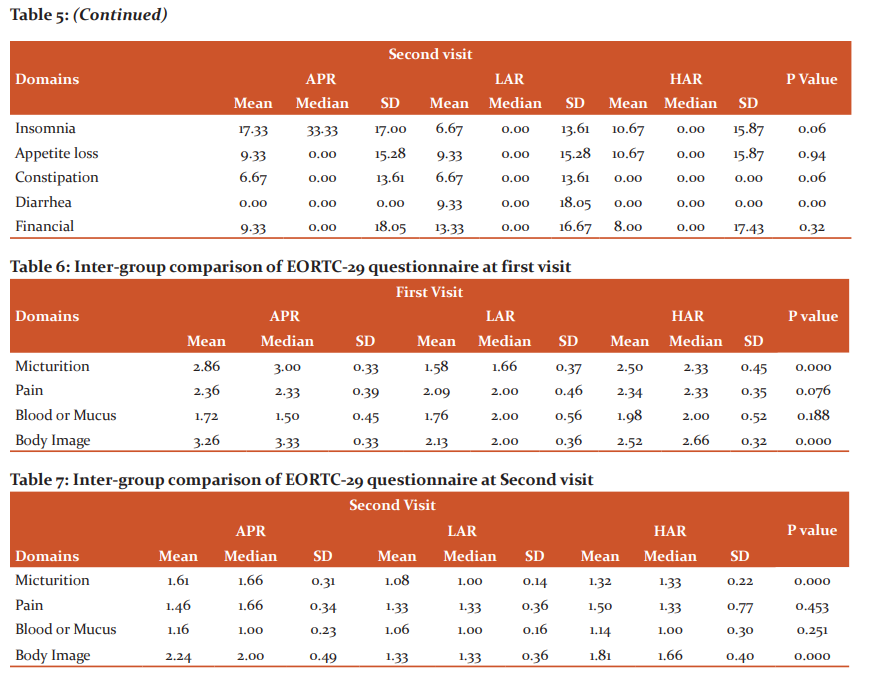
EORTC-30 questionnaire was evaluated with 17 domains, again each containing a certain number of questions and P-value was calculated. An intergroup comparison was done from first to the second visit. At the first visit, a significant difference was found for patients performing strenuous activities and taking part in social activities which were both better in patients undergoing APR. There was also a significant difference in GI manifestations like appetite loss, constipation and diarrhoea, with better appetite and less GI upset in patients undergoing APR. At second visit again patient has undergone APR did well in terms of physical functioning and emotional well-being, while those undergone HAR did well in terms of GI-related complaints like constipation and diarrhoea (Table 4 and 5).
EORTC-29 questionnaire was divided into 4 domains, with 15 questions considered as single items. Out of single items, 7 questions were specific for complications regarding stoma and two regarding sexual dysfunction. Again, intergroup comparison at the first and second visit. While doing intergroup comparison at the first visit, micturition complaints were worst for the patient undergoing APR, while patients undergoing LAR complained least. Similarly, patients undergoing APR had the worst perception of body image and those undergoing LAR had best. Similar results were observed in the second visit as in first (Table 6 and 7).
Discussion
Quality of life analysis following rectal cancer surgery is a sensitive issue among patients because of the implications of treatment on the physical, sexual and psychological status of patients. Though all patients were offered to fill the QOL forms, the compliance rate was 42%. This probably is due to the lack of better understanding by the patients regarding the value of such an audit or shyness on the part of the patient for not giving answers to certain questions related to sexual problems.
Quite a few patients were unwilling to discuss issues regarding their financial and social problems. Particularly questions regarding sexual dysfunction were largely avoided, however low response rates to sexual questions, have also been observed elsewhere6,7 for rest of the questionnaire patient didn’t find much difficulty filling the questionnaire.
A study performed by Tsunoda et al. 8 on Quality of life after low anterior resection and temporary loop ileostomy concluded that patient’s scores on the QOL questionnaires generally well improved after HAR; however, for the patients in whom LAR was performed, the physical and role functioning scores before ileostomy closure were worse than the preoperative scores and generally improved after the closure of an ileostomy.
A study by Gervaz P et al. 9 stated that after one year of surgery, APR patients showed significant improvement QOL as well as tumour-related symptoms; however, the body image remained significantly altered. The treatment-related side effects didn’t improve in the period considered. A meta-analysis was done by Cornish JA et al.10 of quality of life for abdominoperineal excision of rectum versus anterior resection for rectal cancer concluded that when comparing APR with AR, there were no differences in general QOL following the procedures. Individualization of care for rectal cancer patients is essential, but a policy of avoidance of APR cannot currently be justified on the grounds of QOL alone. A study by Guren MG et al.11 concluded that although the rectal function was impaired in patients with low anastomosis, patients who had undergone AR had better QOL than patients who had undergone APR. A study by Gurumann et al.12 concluded that patients undergoing APR have better QOL than patients undergoing AR and patients undergoing LAR have a lower QOL than those undergoing APR. Surgeons should pay close attention to QOL concerns of patients undergoing LAR.
Conclusion
Quality of life as against assumption to be better in patients who had undergone Anterior Resection, in the domains of physical and social functioning, but the effect was diluted when such patients faced more problems regarding gastrointestinal upset. At further follow-up, after overcoming the trauma of surgery and its immediate implications, patients who underwent Abdominoperineal Resection were adjusted to their perception as a social outcast and behaved almost equivalent to patients who underwent Anterior Resection.
Acknowledgements:
We are very thankful to the hospital administration; fellow collogues and all the patient participants who willingly gave consent for the participation in the study.
Source of Funding: None
Conflict of Interest: Nil
References:
-
GLOBOCAN 2008. http://globocan.iarc.fr/factsheets/cancers/colorectal.asp. Accessed September 2020.
-
Jitender S, Mahajan R, Rathore V, Choudhary R. Quality of life of cancer patients. J Exp Ther Oncol 2018;12(3):217-221.
-
Vanessa Burholt, Paul Nash. Short Form 36 (SF-36) Health Survey Questionnaire: normative data for Wales. J Public Health 2010;33(4):587–603.
-
European Organisation for the Research and Treatment of Cancer. Questionnaires: cores. Undated. https://qol.eortc.org/core. Accessed September 2020.
-
Doyle DJ, Goyal A, Bansal P, et al. American Society of Anesthesiologists Classification (ASA Class) In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
-
Koller M, Lorenz W. Quality of life research in patients with rectal cancer: traditional approaches versus a problem-solving oriented perspective. Langenbecks Arch Surg 1998 Dec;383(6):427-36.
-
Sprangers MAG, Te Velde A, Aaronson NK. The construction and testing of the EORTC colorectal cancer-specific quality of life questionnaire module (QLQ-CR38). Eur J Cancer 1999; 35:238–247.
-
Tsunoda A, Tsunoda Y, Narita K, Watanabe M, Nakao K, Kusano M. Quality of life after low anterior resection and temporary loop ileostomy. Dis Colon Rectum 2008 Feb;51(2):218-222.
-
Gervaz P, Bucher P, Konrad B, Morel P, Beyeler S, Lataillade L, Allal A. A Prospective longitudinal evaluation of quality of life after abdominoperineal resection. J Surg Oncol 2008;97(1):14-19
-
Cornish JA, Tilney HS, Heriot AG, Lavery IC, Fazio VW, Tekkis PP. A meta-analysis of quality of life for abdominoperineal excision of rectum versus anterior resection for rectal cancer. Surg Oncol 2007;4(2):24-29.
-
Guren MG, Eriksen MT, Wiig JN, Carlsen E, Nesbakken A, Sigurdsson HK, Wibe A, Tveit KM; Norwegian Rectal Cancer Group. Quality of life and functional outcome following anterior or abdominoperineal resection for rectal cancer. Eur J Surg Oncol 2005;31(7):735-742.
-
Grumann MM, Noack EM, Hoffmann IA, Schlag PM. Comparison of quality of life in patients undergoing abdominoperineal extirpation or anterior resection for rectal cancer. Ann Surg 2001;233(2):149-156.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





