IJCRR - 13(4), February, 2021
Pages: 19-24
Date of Publication: 16-Feb-2021
Print Article
Download XML Download PDF
Incidence of Subcutaneous Emphysema in the Head, Neck and Thoracic Region of Intubated COVID-19 Patients: Our Experiences
Author: Santosh Kumar Swain, Ishwar Chandra Behera, Saurjya Ranjan Das
Category: Healthcare
Abstract:Background: The current global pandemic of the coronavirus disease 2019(COVID-19) is a threat to the lives of the millions of people worldwide. A high number of patients with COVID-19 infections lead to pneumonia or respiratory compromise and followed by undergoing invasive mechanical ventilation. The invasive ventilation may cause barotrauma and further cause pneumothorax, pneumomediastinum and subcutaneous emphysema in the head, neck and chest region. Objective: To assess the surgical emphysema in the head, neck and thoracic region of the intubated COVID-19 patients. Methods: In this retrospective study, clinical and imaging data of the COVID-19 patients with invasive ventilation and development of the subcutaneous emphysema were studied between March 2020 and September 2020. There were 262 patients files were evaluated those were under mechanical ventilation at the intensive care unit (ICU) of COVID-19 hospital. Results: A total of 262 patients with COVID-19 patients underwent invasive mechanical ventilation. Out of them, 38 patients presented with surgical emphysema in the head, neck and chest region. The mean age of the participating patient was 62 year \?14 (standard deviation). Out of the 38 patients, 26(68.42%) were male and 12 female (31.57%) with male to female ratio of 2.16:1. Conclusion: Patients with COVID-19 infections with invasive mechanical ventilation have a high chance of the barotrauma. The development of the barotrauma in the lungs may lead to pneumothorax and surgical emphysema in the head, neck and chest region.
Keywords: COVID-19 patients, Acute respiratory distress syndrome, Surgical emphysema, Pneumomediastinum
Full Text:
INTRODUCTION
The coronavirus disease 2019(COVID-19) is a dreaded viral disease caused by a novel virus called severe acute respiratory syndrome coronavirus 2(SARS-CoV-2) and has been called as a pandemic by the World Health Organization(WHO) with more than 4.8 million confirmed patients and 300 thousand death globally.1 Acute respiratory distress syndrome (ARDS) and hypoxemic respiratory failure are found in COVID-19 infections and considered as feared complications of this disease.2 These patients require intensive care admission and mechanical ventilation. In current COVID-19 pandemic, there is the rising number of patients requiring orotracheal intubation or tracheostomy for ventilation. One study from the USA, 22% of the hospitalized COVID-19 patients requires invasive mechanical ventilation.3 These patients are developing a life-threatening condition called as pneumomediastinum or pneumothorax where the air is present in the mediastinum or pleural space respectively. These manifestations often lead to subcutaneous emphysema in the head and neck region.4 Clinical practice during non-COVID-19 time showed the development of the subcutaneous emphysema and pneumomediastinum as uncommon entities which often result from air leak from the lungs or other luminal organs.5 It is commonly associated with injuries of the tracheobronchial tree, lungs or pleural space and trauma to the oesophagus. In the last few months, there is the increasing number of the pneumomediastinum and subcutaneous emphysema in the head, neck and chest region following orotracheal intubation and ventilation in confirmed COVID-19 patients. This is a novel clinical finding among the intubated COVID-19 patients, which carries high morbidity and mortality. We found many COVID-19 patients with invasive ventilation at the COVID hospital ICU presenting with pneumothorax, pneumomediastinum and subcutaneous emphysema at the head. Neck and chest region. On this observation, we hypothesized that barotrauma related to invasive mechanical ventilation can cause subcutaneous emphysema in COVID-19 patients. Numerous publications are documenting the clinical presentations and outcome of the COVID-19 infection. However, there are very few or no studies done in these rare complications like pneumothorax, pneumomediastinum and subcutaneous emphysema in this region. Here, this study aims to evaluate the details of the subcutaneous emphysema in the head, neck and chest region in COVID-19 patients under invasive mechanical ventilation.
MATERIALS AND METHODS
This retrospective study was conducted at a COVID-19 hospital with an intensive care unit (ICU) attached to a tertiary care teaching hospital. This study was done between March 2020 to September 2020. This study was approved by the institutional ethical committee (IEC) of our medical college with reference number IEC/SOA/IMS/34/12.02.2020. The institutional review board made waiver of authorized consent by the patients or patient relatives because of the urgent pandemic situation. There were 262 patients under mechanical ventilation at the ICU who participated in this study. All the participating patients were COVID-19 patients confirmed based on real-time reverse transcription-polymerase chain reaction assays. The clinical features including age, sex, date of admission, date of invasive mechanical ventilation(IVM), date of development of the subcutaneous emphysema and date of death (if applicable) were documented. The patient outcomes were evaluated. Chest X-ray was done in all the participating patients. The inclusion criteria of this study were age older than 18 years, COVID-19 patients with ARDS at the ICU and with invasive mechanical ventilation. Patients admitted until September 30, 2020, were included in the study. All the data and variables were collected from the electronic patient registry. The diagnosis of the pneumothorax and subcutaneous emphysema were confirmed by the chest X-ray or CT scan. All these 38 patients were invasively ventilated for respiratory compromise with severe hypoxemia. We documented details of the co-morbidities, ventilation, signs and symptoms associated with pneumomediastinum and the management. The patients with a previous history of lung surgery or thoracotomy before the diagnosis of the COVID-19 were excluded from this study. The details of the ventilator settings were not documented as these were outside the scope of this observational study. In this study, all the data were recorded and analyzed by using Statistical Package for Social Science (SPSS) software, v20.
RESULT
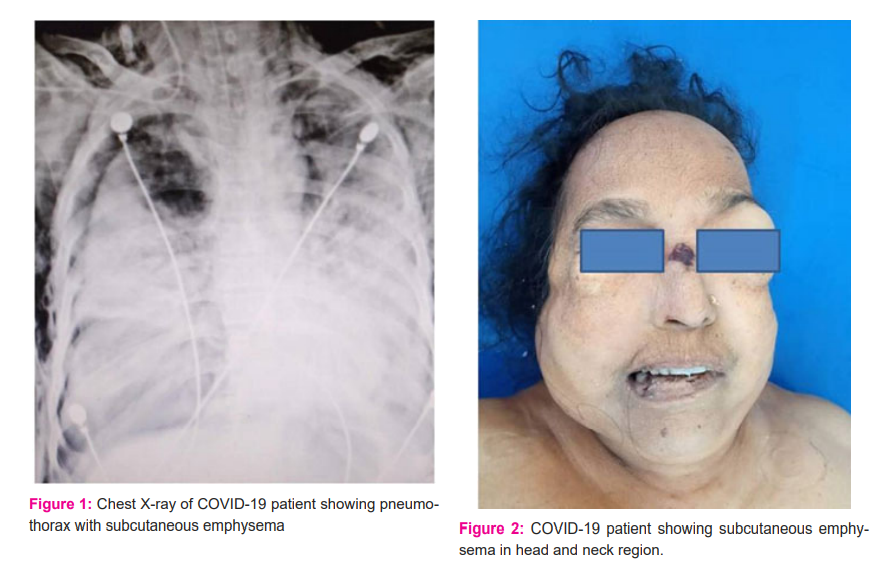
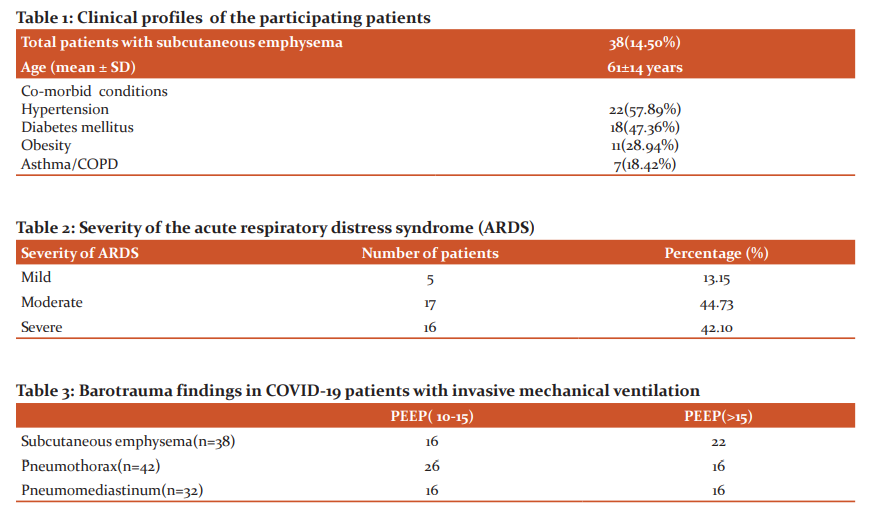
There were 38 patients (14.50%) developed subcutaneous emphysema in the head, neck and thoracic region out of the 262 intubated patients at the ICU of the COVID hospital. The age ranges were 18 years to 84 years with a mean age of 61±14 years. Barotrauma was found in 64 cases (24.24%) and confirmed in chest X-ray and CT scan of the thorax. Out of 64 cases with barotrauma, 42 showed pneumothorax (Figure 1), 38 showed subcutaneous emphysema and 32 with pneumomediastinum. Out of the 38 patients with emphysema in the head, neck and chest region (Figure 2), 26 were male and 12 female with male to female ration is 2.16:1. All these 38 patients were also diagnosed with pneumothorax. The majority of the patients had underlying comorbidities such as hypertension in 22 patients (57.89%) and diabetes mellitus in 18 patients (47.36%) (Table 1). Out of 38 patients, 11 (28.94%) were suffered from obesity and had body mass index (BMI) above 30. There were 7 patients with a previous history of COPD (18.42%). Out of 38 patients, 24 were intubated by using direct laryngoscopy and by video laryngoscopy in 14 patients. No bougies or stylets were used at the time of intubations in all of the cases. On average, COVID-19 patients were hospitalized for 4.8 days before invasive mechanical ventilation (range 1 to 22 days). Time to develop subcutaneous emphysema after tracheal intubation ranged from 5 hours to 16 days with a mean duration of 5.3 days. All these 38 patients were managed with lung protective strategies. Out of the 38 patients, 16(42.10%) showed evidence of severe ARDS at the time of the barotrauma (PaO2/FiO2<100) (Table 2). Positive expiratory pressure (PEEP) requirements were 10 to 20 cmH2O with mean 14.6 cmH2O. All these 38 patients developed subcutaneous emphysema in the head and neck region along with increasing requirements of the oxygen. There were 32 patients with pneumomediastinum (Table 3). The diagnosis of the pneumomediastinum was done due to progressive increase of the subcutaneous emphysema in the head and neck and chest area and this is confirmed by the imaging such as X-ray chest or CT scan of the chest. Four patients (10.52%) revealed tracheal injury visible in the CT scan of the thorax and again confirmed by the flexible bronchoscopy. Bilateral intra-pleural and subcutaneous chest drains were placed in 15 patients for treating the sequelae presumed injuries at the trachea. All those developed pneumothorax underwent bedside insertion of the thoracostomy tube. Out of the 38 patients with surgical emphysema at the head, neck and thoracic region, 25 patients (65.78%) were passed away. Three patients were died after being put on extracorporeal membrane oxygenation (ECMO) with increasing lactate and right heart failure because of pulmonary hypertension. Ten patients were successfully decannulated after removal of the chest drains and are presently clinically stable.
DISCUSSION
The current pandemic of the COVID-19 infections is a global threat and affect the lives of the millions of people of the worldwide. It has made a huge burden on health care systems globally. SARS-CoV-2 pneumonia often needs mechanical invasive ventilation for treating the hypoxemia.6 However, the subcutaneous emphysema and pneumothorax aggravate respiratory failure. The exact pathophysiology for development of the pneumothorax and subcutaneous emphysema in SARS patients are thought to be associated with diffuse alveolar damage which causes leakage of the gas into the pulmonary interstitium leading to the pneumomediastinum and subcutaneous emphysema.7 This mechanism supported by the postmortem studies on SARS lungs showing extensive features of acute exudative alveolar and vascular damage.8 The alveoli of the lungs are prone to rupture by a diffuse alveolar injury caused by SARS-CoV-2 infections.9 The alveolar rupture causes air leakage and interstitial emphysema. One report documented the alveolar rupture in a patient without invasive ventilation which indicates that subcutaneous emphysema and pneumothorax may be associated with SARS-CoV-2 infection.10 In this study, 38 patients (14.50%) presented with subcutaneous emphysema and 42(16.03%) presented with pneumothorax. As there is long term increase of alveolar pressure, decrease in alveolar capillary blood supply and impairment in the nutrition of the lung tissue in chronic obstructive pulmonary disease (COPD), the tolerance and elasticity of the alveolar wall are usually weakened. So, SARS-CoV-2 pneumonia in COPD patients is more likely to result in spontaneous pneumothorax and subcutaneous emphysema.11 Pneumothorax, mediastinal emphysema and subcutaneous emphysema are known complications of invasive mechanical ventilation found in critical patients.12 In case of invasive ventilation in the patient, the air pressure in the respiratory tract is very high which lead to the raised pressure gradient between the alveoli and surrounding tissues, causing rupture of the alveoli and development of the emphysema. During the same time, as average air pressure at the mediastinum is lower than surrounding lung tissue, the air enters the mediastinum and cause pneumomediastinum and subcutaneous emphysema.13 Traumatic or improper intubation of the endotracheal tube may cause injury to the tracheal wall and further cause subcutaneous emphysema. The airway of the elderly persons is more prone to injury than young age during tracheal intubation. Patients with a history of thoracotomy are more prone to the development of the subcutaneous emphysema. In this study, patients with a history of thoracotomy were excluded. Patients with mediastinal emphysema, pneumothorax and subcutaneous emphysema and with ventilators progress to more respiratory dysfunctions. So, patients with ventilators require a dynamic review with chest radiograph to early identification of the complications.COVID-19 patients COPD and invasive mechanical ventilation are prone to respiratory failure. So, clinicians should think of these clinical situations and repeat X-ray chest for preventing respiratory failure.
COVID-19 infections cause inflammation and oedema of the upper and lower airways and make patients vulnerable to injury from the instrumentation.14 Tracheal intubation in case of hypoxemia during an emergency may cause tracheobronchial injury. Proximal injury of the trachea is often responsible for the development of the subcutaneous emphysema at the head and neck area. In this study, 4 patients revealed tracheal injury visible in the CT scan of the thorax and again confirmed by the flexible bronchoscopy. The COVID-19 patients who develop acute respiratory syndrome (ARDS) require aggressive ventilatory support and further may land in multi-organ failure which needs intensive care stay for longer periods. There is an unusual occurrence of pneumothorax or pneumomediastinum along with surgical emphysema in the head and neck region in intubated patients.15 Subcutaneous emphysema and pneumomediastinum are usually resulting of spontaneous rupture of the alveoli or more rarely due to disruption of the upper airways or gastrointestinal tract and associated with the presence of air within the mediastinal cavity or in subcutaneous tissues respectively.16 The clinical presentations of subcutaneous emphysema and/or mediastinum depend on the amount of the extravasated air and degree of extension in the affected area. Mostly, the presentations include swelling and crepitus in the affected anatomical site, chest pain, dyspnea and dysphagia.17 The most commonly accepted explanation for the development of the subcutaneous emphysema and pneumomediastinum are presently based on the sequence of events called as the so-called “Macklin Effect”.18 Once there is rupture of the alveoli due to primary lung trauma or increased pressure gradient between alveoli and their surrounding interstitial space, free air enters along the peri-bronchovascular interstitial sheaths or the visceral pleura. This air finally spreads into the mediastinum and head and neck region.19 During the SARS outbreak in 2002-2003, a study at Hong Kong documented an incidence of 11.6% of spontaneous pneumomediastinum in infected persons. 20 There is rarely any study for establishing the exact incidence of spontaneous pneumomediastinum and subcutaneous emphysema in COVID-19 patients. In this study 38 cases (14.50%) presented with subcutaneous emphysema, 42 (16.03%) presented with pneumothorax and 32 cases (12.21%) presented with pneumomediastinum.
COVID-19 patients have a higher chance of barotrauma. This incidence may be explained based on the previous studies with ARDS resulting from pneumonia which may cause early barotrauma.21 These patients often need high PPEP to maintain oxygenation, which increases the chance for barotrauma. Reports from China also documented the spontaneous pneumomediastinum in COVID-19 patients.22 In COVID-19 patients, barotrauma may occur and progresses rapidly after invasive mechanical ventilation, which may show the worsening of the spontaneous barotrauma from lung injury as seen in some of our patients. This manifestation may also reflect the severity of lung injury by SARS-CoV-2 infections.
There were three case reports published of spontaneous development of pneumomediastinum in COVID-19 patients. In the first case, pneumomediastinum developed on 11th day after intubation, however, resolved with conservative management.23 The second case of 38-year-old man developed pneumomediastinum was found to be with multiple bullae leading to surgical emphysema and pneumomediastinum. This was thought to be increased intra-thoracic pressure after coughing which managed conservatively.24 The third case was a female patient where CT thorax showed pneumomediastinum. This patient passed away after two days with respiratory failure.25 Pneumomediastinum is an uncommon but well-documented entity in acute respiratory distress syndrome (ARDS). One retrospective study on CT scans of the thorax in invasively ventilated patients for ARDS shown 7.4% radiologically confirmed pneumomediastinum.26 Subcutaneous emphysema and pneumomediastinum are usually diagnosed with chest X-ray, however, non-contrast CT scan of the chest is more sensitive for diagnosis.27 As the presence of the subcutaneous cervical and thoracic emphysema is suggestive of injury to thoracic structures, the examination of the chest may also give a further diagnostic benefit. So, the clinical presentations and imaging are helpful for diagnosis of the surgical emphysema and pneumomediastinum in intubated patients with COVID-19 infections.28 Pruning of the mechanically ventilated patients for optimizing the ventilation-perfusion mismatch is a possible cause for tracheobronchial injury and surgical emphysema in the head and neck part along with pneumothorax. The repositioning manoeuvre is a risk factor for causing this dreaded clinical entity, so clinicians should be alert before planning the prone position of the patient.29 Rupture of alveoli and subsequent development of the pneumothorax may be the cause of development of the surgical emphysema in the head and neck region. In instances of barotrauma which progress into pneumothorax, a percutaneous thoracostomy tube is often done as treatment of choice in comparison to the open thoracostomy as it decreases the exposure of the health care staffs and other patients to the aerosolized particles.
CONCLUSION
Development of the subcutaneous emphysema, pneumothorax and pneumomediastinum in COVID-19 patients are considered as bad prognostic markers. Alveolar damage and weak membranous part of the trachea, traumatic intubation in emergency scenarios, frequent pruning and barotrauma due to high ventilator pressures may lead to pneumomediastinum and follow by the emphysema at the head &neck and thoracic region. Bilateral chest and subcutaneous drains are helpful for the management of this critical situation for avoiding the decompression. In conclusion, subcutaneous emphysema in the head and neck region, pneumothorax and mediastinal emphysema may found in patients with SARS-CoV-2 infections.
Conflict of interest: Nil
Funding: No Funding sources were granted or used specifically for this work.
Author Contribution: SKS: Concept, data collection and data analysis; ICB: Data collection, data analysis, and drafting the manuscript; SRD: Data collection and drafting the manuscript.
References:
1. Johns Hopkins University. The COVID-19 United States Cases 2020, May 14; Available from https://coronavirus.jhu.edu/us-map.
2. Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. J Am Med Assoc 2020; 323(13): 1239-1242.
3. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: a prospective cohort study. Br Med J 2020;369:m1966.
4. Swain SK, Behera IC. Managing pediatric otorhinolaryngology patients in coronavirus disease-19 pandemic-A real challenge to the clinicians. Ind J Child Health 2020;7(9):357-362.
5. Sun R, Liu H, Wang X. Mediastinal emphysema, giant bulla and pneumothorax developed during COVID-19 pneumonia. Korean J Radio 2020;21(5):541.
6. Swain SK, Acharya S, Sahajan N. Otorhinolaryngological manifestations in COVID-19 infections: An early indicator for isolating the positive cases. J Sci Soc 2020;47(2):63.
7. Chu CM, Leung YY, Hui JY, Hung IF, Chan VL, Leung WS, et al. Spontaneous pneumomediastinum in patients with the severe acute respiratory syndrome. Eur Resp J 2004;23(6):802-804.
8. Gu J, Korteweg C. Pathology and pathogenesis of the severe acute respiratory syndrome. Am J Pathol 2007;170(4):1136-1147.
9. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, Liu S, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Resp Med 2020; 8(4):420-422.
10. Zantah M, Castillo ED, Townsend R, Dikengil F, Criner GJ. Pneumothorax in COVID-19 disease-incidence and clinical characteristics. Resp Res 2020;21(1):1-9.
11. Gadre SK, Duggal A, Mireles-Cabodevila E, Krishnan S, Wang XF, Zell K, et al. Acute respiratory failure requiring mechanical ventilation in severe chronic obstructive pulmonary disease (COPD). Medicine (Baltimore) 2018;97(17):e0487.
12. Badaoui R, Thiel V, Perret C, Popov I, Dupont H. Bilateral pneumothorax, cervicofacial and mediastinal emphysema after surgical tracheostomy. Ann Fr Anesth Reanim 2013;32:718–720.
13. Sonobe S, Inoue S, Nishiwada T, Egawa J, Kawaguchi M. A case of subcutaneous emphysema/mediastinal emphysema during the use of a humidified high-flow nasal cannula. J Am Clin Rep 2019;5(1):1-3.
14. Swain SK, Agrawal R. Mastoid surgery: a high risk aerosol-generating surgical procedure in COVID-19 pandemic. Int J Otorhinolaryngol Head Neck Surg 2020;6(10):1941.
15. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020;395(10223):507-513.
16. Banki F, Estrera AL, Harrison RG, Miller III CC, Leake SS, Mitchell KG, et al. Pneumomediastinum: aetiology and a guide to diagnosis and treatment. Am J Surg 2013;206(6):1001-1006.
17. Sahni S, Verma S, Grullon J, Esquire A, Patel P, Talwar A. Spontaneous pneumomediastinum: time for consensus. North Am J Med Sci 2013;5(8):460-464.
18. Wintermark M, Schnyder P. The Macklin effect: a frequent aetiology for pneumomediastinum in severe blunt chest trauma. Chest 2001;120(2):543-547.
19. Dehours E, Vallé B, Bounes V, Lauque D. A pneumomediastinum with diffuse subcutaneous emphysema. J Emergency Med 2013;44(1):81-82.
20. Chu CM, Leung YY, Hui JY, Hung IF, Chan VL, Leung WS, et al. Spontaneous pneumomediastinum in patients with the severe acute respiratory syndrome. Eur Resp J 2004;23(6):802-804.
21. Eisner MD, Thompson BT, Schoenfeld D, Anzueto A, Matthay MA, Acute Respiratory Distress Syndrome Network. Airway pressures and early barotrauma in patients with acute lung injury and acute respiratory distress syndrome. Am J Resp Crit Care Med 2002;165(7):978-982.
22. Zhou C, Gao C, Xu M. COVID-19 with spontaneous pneumomediastinum. Lancet Infect Dis 2020;20(4):510.
23. Janssen J, Kamps MJ, Joosten TM, Barten DG. Spontaneous Pneumomediastinum in a male adult with COVID-19 pneumonia. Am J Emer Med 2020. doi: 10.1016/j.ajem.2020.07.066 [Epub ahead of print]
24. Quincho-Lopez A, Quincho-Lopez DL, Hurtado-Medina FD. Case Report: Pneumothorax and Pneumomediastinum as Uncommon Complications of COVID-19 Pneumonia—Literature Review. Am J Trop Med Hygiene 2020;103(3):1170-1176.
25. Wang J, Su X, Zhang T, Zheng C.Spontaneous pneumomediastinum:a probable unusual complication of coronavirus disease 2019(COVID-19) pneumonia. Korean J Radiol 2020;21:627-628.
26. Simon M, Braune S, Laqmani A, Metschke M, Berliner C, Kalsow M, et al. Value of computed tomography of the chest in subjects with ARDS: a retrospective observational study. Resp Care 2016;61(3):316-323.
27. Fosi S, Giuricin V, Girardi V, Di Caprera E, Costanzo E, Di Trapani R, et al. Subcutaneous emphysema, pneumomediastinum, pneumoretroperitoneum, and pneumoscrotum: unusual complications of acute perforated diverticulitis. Case Rep Radiol 2014;2014:1-5.
28. Dahlawi H. Changes in Haematological Parameters among COVID-19 Patients. Int J Cur Res Rev 2020;12(18):2-4.
29. Swain SK, Achary S, Das SR. Vertigo in pediatric age: Often challenge to clinicians. Int J Cur Res Rev 2020;12(18):136-141.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





