IJCRR - 13(3), February, 2021
Pages: 165-167
Date of Publication: 03-Feb-2021
Print Article
Download XML Download PDF
Current Trend in Urology Practice During COVID-19 Pandemic: Our Experience
Author: Debashis Routray, Debabrata Sabat, Suren Kumar Das, Pranab Pattanaik, Rahul Pradhan
Category: Healthcare
Abstract:Introduction: COVID-19 caused a large number of mortality, morbidity and impact on the socioeconomic status of the various countries including India. Over the time COVID-19 affected number of body systems critically including urinary system and related organs. Objective: To evaluate the changing scenario in urology in the present pandemic situation arising due to coronavirus disease-19. Methods: A database of a total number of 160 patients during the period of April to July 2020 were recorded. Symptom-based questionnaires were made for the screening of the patients. The cases were divided based on the severity and emergency of the procedure and tabulated accordingly. The various safety and precautionary measures in this pandemic of COVID-19 are discussed and various emergency procedure undertaken is reviewed. Results: The patients were prioritized based on malignant and non-malignant conditions in elective surgical procedures. The priorities in case of emergency surgical procedures involved haematuria, urosepsis, urological trauma, obstructive uropathy, urinary retention due to urethral strictures etc. Conclusion: During the pandemic covid 19 situations, our centre being the covid referral centre, we have operated 160 patients with various guidelines prepared by the institute from time to time and we have safely operated and discharged all our patients..
Keywords: COVID 19, Pandemic, Mortality, Haematuria
Full Text:
Introduction
The ongoing pandemic of COVID-19 has shaken the world with a large number of mortality, morbidity and impact on the socioeconomic status of the various countries.1 The current situation COVID-19 cases in the whole world, (confirmed cases-17,106,007 and deaths-668,910 on 31st July 2020). India being in 3rd position with confirmed cases-1,638,870, death -35,747 on 31st July 2020.2 Odisha has made achievements with less number of mortality rate and the higher number of recovered cases in comparison to other states of India. As on 31st July 2020 in Odisha, confirmed cases-33,479 and recovered cases -20,000 and death-187.
Our centre being a tertiary care centre as well as COVID hospital in Odisha, our institution is involved in formulating and implementing strategies for optimizing health care outcomes.3,4 The outcome of the current pandemic situation can be monitored by the fact that repeated attempts of lockdown, shutdown, containment and curfew have been implemented for the control of the spread of the disease.5,6 This has impacted various urological illnesses in our community simultaneously.2
MATERIALS AND METHODS
During the initial phases of lockdown, patients visiting our OPD or emergency being screened in the flu clinic using a symptom-based questionnaire (Table 1) and were initially stratified into the suspected case or not. The suspected cases were sent for reverse transcriptase-polymerase chain reaction (RT-PCR).7,8
As soon as lockdown is eased, there is the rush of patients in our OPD. Hence, we have prepared with full proof action plan to prioritize and triage these patients to manage the current situation and manage these urological illnesses according to guidelines prepared by our institution and also according to guidelines prepared by a world health organization, the urological society of India as well.9,10
During the initial month of April 2020, due to less availability of RT-PCR kit in our institution, we used to triage the patient and provide treatment according to priorities.11,12 But in the latter part of April 2020, due to surplus amount of RT-PCR kit and PPE kit in our institution and also new guidelines prepared for the COVID -19, our centre used to send all indoor patients to isolation ward till the covid report turns negative. In this phase, we advocate continued use of symptom-based screening and RT-PCR test before embarking on the elective procedure to save the treating team from cross-infection. Covid-19 rapid antigen test was available in July 2020 in our institution. So we started following the symptom-based screening and RT-PCR test followed by rapid antigen test on the day of surgery. By the end of July 2020, our institution had the highest number of COVID bed availability reaching 900 beds for the separate dedicated covid hospital block with OT, ICU unit, wards and in-house investigation laboratories and imaging facilities with haemodialysis unit.
RESULT AND DISCUSSION
Based on the above protocol, we have operated 160 patients from April to July 2020. 2 patients were COVID positive detected preoperatively. Rest of these patients did not develop symptoms of COVID-19 following surgery.
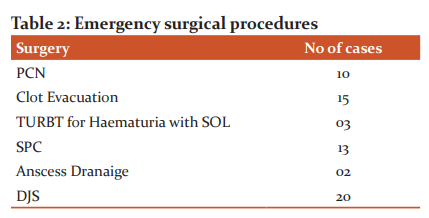
Emergency urology surgical procedures:
Since the beginning of lockdown and as recommended by all guidelines, only emergency procedures are being operated. The rationale for this is to conserve the already strained health care resources. The priorities of our emergency services involved malignancies, haematuria and urosepsis and urological trauma, obstructive uropathy due to stone diseases or strictures. Urinary retention caused by a prostatic enlargement or urethral strictures (Table 2).
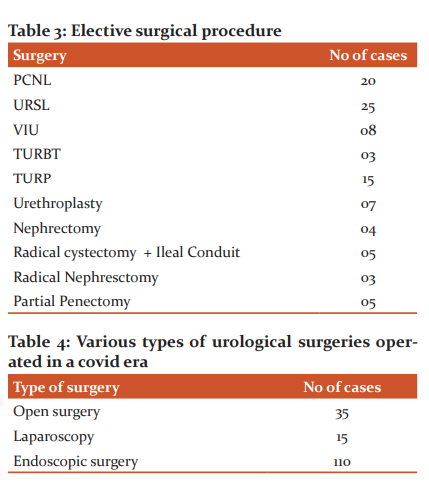
Elective urology surgical procedure
We have prioritized our patients with malignant and non-malignant conditions. We have followed above mentioned guidelines for the surgical procedures (Table 3) and types of urological surgeries operated in the covid era (Table 4).
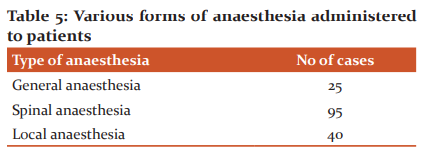
Anesthesia Consideration
General anaesthesia leads to aerosol generations and therefore poses the highest chance of transmission to OT staffs. Hence, wherever feasible, regional anaesthesia considered. Patient under regional anaesthesia wears an N95 mask. During regional anaesthesia, anaesthetist used PPE kit (Table 5).
General Surgical Consideration
Staffs were asked to wear N95 mask and minimum staffs were allowed in OT. Hand hygiene was strictly followed. Donning and doffing procedures were strictly followed. OT was well ventilated with negative pressure ventilation and high-efficiency particulate air (HEPA) filters. Surgeons, anaesthetists and OT staffs were using face shields with N95 mask. Only a few cases of laparoscopy and open surgery, or patients who were having fever, PPE kit were used. All the patients were routinely screened preoperatively for covid 19 and no patients were developed covid 19 symptoms postoperatively and at the time of discharge.
2 patients with ureteric colicky with ureteric calculus were covid 19 positives during routine RT-PCR test. Since these patients requiring surgical intervention, so these patients were posted in covid 19 dedicated OT. All the team members of the OT were quarantined after the procedure. No staffs got covid 19 symptoms after the quarantine period.
Endourology procedures
While viral RNA has been identified in the urine samples of 6.9% of patients who had recovered from COVID 19, others have reported that virus shedding in urine is absent. To decrease the chance of contaminations, the entire operating team had taken precaution with using impervious drapes, closed drainage of returning irrigation fluids. In most of our patients of PCNL and URSL, DJ stenting was avoided where ever applicable and tubeless PCNL were achieved. In the post-operative period, these patients did well and discharged satisfactorily. Most of our cases for stone surgery, regional anaesthesia protocol in the form of spinal anaesthesia was administered.
Laparoscopic Procedures
Due to the risk of transmission of the virus in the smoke due to electrocautery and aerosol due to co2 pneumoperitoneum, we had followed all precautionary measures. Appropriate size port incisions were given to prevent air leak. Electrocautery was used judiciously. Suction and irrigation system was used to prevent aerosol transmission. In our centre, laparoscopy was done for patients who were surgically fit candidate for laparoscopy.
Open Surgical Procedures
Adequate measures to minimize the generation of aerosol were followed. Most of our patients had given regional anaesthesia and general anaesthesia was restricted. Substitution urethroplasty was done with preferred healthy local flaps (inner preputial graft, vaginal flaps) and for unhealthy local flaps, buccal mucosal grafts were preferred.
CONCLUSION
During the pandemic covid 19 situations, our centre being the covid referral centre, we have operated 160 patients with various guidelines prepared by the institute from time to time and we have safely operated and discharged all our patients.
Conflict of Interest: None
Source of Funding: None
References:
-
Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, et al. Presumed asymptomatic carrier transmission of COVID?19. JAMA 2020;323(14):1406?1407.
-
Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al. SARS?CoV?2 viral load in upper respiratory specimens of infected patients. N Engl J Med 2020; 382:1177?9.
-
Jaiswal R. An Indian Doctor, Working in New York ER, Describes War vs. Coronavirus. Available from: https://www.covid19india.org/.
-
Lei S, Jiang F, Su W, Chen C, Chen J, Mei W, et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID?19 infection. E Clin Med 2020;100331.
-
Liu R, Han H, Liu F, Lv Z, Wu K, Liu Y, et al. Positive rate of RT?PCR detection of SARS?CoV?2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clin Chim Acta 2020; 505:172?5.
-
Wang W, Xu Y, GaoR, Lu R, Han K, Wu G, et al. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020; 323:1843-4.
-
Li Z, Yi Y, Luo X, Xiong N, Liu Y, Li S, et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J Med Virol 2020;10.1002/jmv.25727.
-
Zhang W, Du RH, Li B, Zheng XS, Yang XL, Hu B, et al. Molecular and serological investigation of 2019?nCoV infected patients: Implication of multiple shedding routes. Emerg Microbes Infect 2020; 9:386?389.
-
Containment Plan for Large Outbreaks: Novel Coronavirus Disease 2019 (COVID?19). Ministry of Health and Family Welfare Government of India. Available from: https://www.mohfw.gov.in/pdf/3Containment.
-
Kumar A. Corona Virus Disease USI Information Centre. Available from: https://usi.org.in/New/Spe_pdf/USI%20Corona%20advise%20edited.pdf. Al-Muharraqi MA. Testing recommendation for COVID-19 (SARSCoV- 2) in patients planned for surgery - continuing the service and 'suppressing' the pandemic. Br J Oral Maxillofac Surg 2020; S0266-4356:30164-9.
-
Ribal MJ, Cornford P, Briganti A, Knoll T, Gravas S, Babjuk M, et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organization?Wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur Urol 2020;78(1):21–28.
-
Proietti S, Gaboardi F, Giusti G. Endourological stone management in the Era of the COVID?19. Eur Urol 2020; S0302?2838 (20)30217?7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





