IJCRR - 13(3), February, 2021
Pages: 78-82
Date of Publication: 03-Feb-2021
Print Article
Download XML Download PDF
Patterns of Anaemia in Elderly Patients in Relation with RBC Indices
Author: Munesh, Vani Mittal, Sunil Arora, Raj Kumar
Category: Healthcare
Abstract:Background: Anaemia, one of the most common manifestations seen in elderly patients is still a concern in the modern world as its prevalence increases with age. Higher mortality rates have been found in elderly who had anaemia in comparison to those who didn't. Anaemia greatly influences the quality of life, ability to recover from illness and functional capability. Objective: To study the patterns of anaemia in elderly patients in relation with RBC indices. Methods: An observational study of 100 elderly patients (visiting hospital including both OPD and IPD) with anaemia was done for four months in a tertiary care hospital to determine the aetiology behind the anaemia with the help of RBC indices. Results: Anaemia was categorized based on haemoglobin levels and patterns on the peripheral blood smear. It was found that in the elderly population most common pattern of anaemia was microcytic hypochromic due to deficiency of iron and high prevalence of chronic diseases. More than 50% of the patients in the study had moderate anaemia with RBC indices showing a wide range of values due to different etiological factors leading to anaemia. Conclusion: Anaemia is one of the major concerns in elderly as it accentuates morbidity and mortality and needs to be investigated thoroughly as most of the cases are treatable and only a few have unexplained anaemia. This being a hospital-based study only a few people could be evaluated, and so screening programs should be encouraged on a community level for older persons.
Keywords: Anaemia, Total blood count, Red blood cells, Hematocrit
Full Text:
INTRODUCTION
Anaemia is defined as a decrease in the number of red blood cell (RBC) or haemoglobin (Hb) which results in lower capability of blood to carry oxygen.1 Anaemia in the geriatric age group is a great concern as it increases the risk of mortality and morbidity.2 The census report of 2011 shows the population of elderly as 8.1% of the total population in India and it is expected to increase to 19% by 2050.3 Anaemia is not related with ageing in elderly but it is associated with poor quality of life, poor performance status, dementia, depression and reduced mobility and it worsens the co-morbidities like cardiovascular disease and other conditions.4-8 The United Nations has accepted age of 60 years or above to define an ‘elderly’ or older person.9 According to the World Health Organization (WHO), the prevalence of anaemia in people of age group 60 years or older was found to be 23.9% i.e. 164 million people affected across the globe.10
Anaemia is defined by WHO as a haemoglobin concentration of <13gm/dl for men and <12gm/dl for women.11 Evaluation of anaemia to explicate its cause can be done by collaborating the morphological classification of anaemia with the red blood cell indices given by the automated cell counter. Categorization of anaemia like normocytic normochromic, microcytic hypochromic, macrocytic and dimorphic picture is helpful in treatment.12 Peripheral blood smear (PBS) examination comes up with invaluable information for diagnosing anaemia with red cell morphology evaluation i.e. size, shape, chromasia, the concentration of haemoglobin, and inclusions.13 In the present study, we aimed to investigate the pattern of anaemia in the elderly patient with RBC indices in combination with PBS study and underlying aetiology of anaemia.
MATERIALS AND METHODS
An observational study was undertaken in the Pathology Laboratory at a tertiary care hospital for a period of 4 months from December 2019 to March 2020. All blood samples of patients which were received in k3- EDTA anticoagulated vacutainer in the laboratory and were processed within one hour of collection using the 6 part automated haematology analyzer. Haemoglobin and red blood cell (RBC) indices i.e. mean corpuscular volume (MCV), mean corpuscular haemoglobin (MCH), mean corpuscular haemoglobin concentration (MCHC), red cell distribution width (RDW-CV) and hematocrit (Hct) were recorded and anaemia and its pattern was reevaluated by peripheral smear examination on Leishman stained slides in all cases. We included 100 patients of age more than 60 years with anaemia (Hb <12 gm/dl in women, Hb <13gm/dl in males.11
Approval for waiver of patients consent and patient information sheet was obtained from Institutional Ethical Committee since the study involved the data available in the record that were anonymized and coded to delink with any identity of patient (Reference- National Ethical Guidelines by ICMR on biomedical research 2017, chapter 5, Informed consent process Box 5.2 “Conditions for granting waiver of consent”).
Inclusion criteria
1. Patients of age 60 years and older 9
2. WHO criteria of haemoglobin <12gm/dl in women and <13gm/dl in males to define anaemia. [11]
Exclusion criteria
1. Patients who had a history of blood transfusion within the 3 past months
2. Patients on chemotherapy and radiotherapy
3. Patients with a history of bleeding disorders or having acute bleeding
4. Patients with End-Stage Renal Disease
Haemoglobin and red blood cell indices were assessed in all cases. The data were tabulated and analyzed. Statistical mean and standard deviation (SD) was calculated for the respective parameters and comparison was done between different categories.
RESULTS
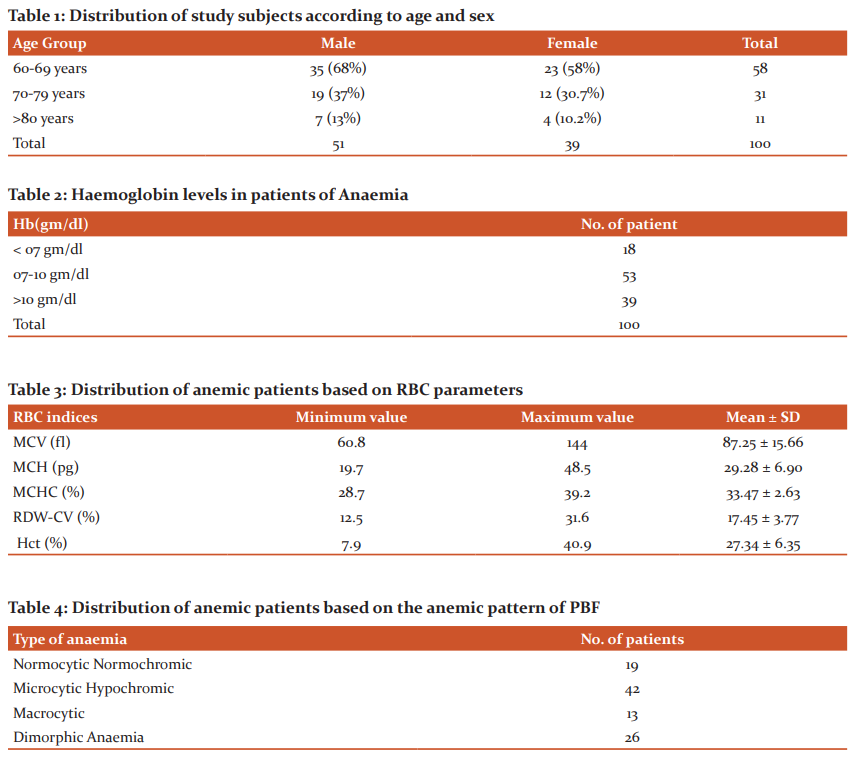
In this study, we included 100 patients who required Complete Blood Count (CBC) investigation as a part of their management and were found to be anaemic. The age group of presenting patients varied from 60 to 90 years of age, with the mean age of 68.43 ± 7.5 years in the study. A majority of patients were in the age group of 60-69 years i.e. 58%. When correlated with the gender both males and females showed higher numbers in this age group. An overall slight male predominance was observed in our study with 51% males as compared to 39% of female patients. (Table 1)
More than half of the patients i.e. 53% suffered from moderate anaemia, with haemoglobin level between 7-10 gm/dl. This was followed by 38% with mild anaemia (haemoglobin >10gm/dl) and only 18% had severe anaemia (haemoglobin <7 gm/dl). The mean haemoglobin of the 100 anemic patients came out to be 9.09 ± 2.16 gm/dl (Table 2).
In this study, we studied the RBC parameters of all the patients. The mean corpuscular volume (MCV) was in the range of 60.8 to 144.0fl with the mean value of MCV as 87.25±15.66 fl. The mean ± SD value of mean corpuscular haemoglobin (MCH) and mean corpuscular haemoglobin concentration (MCHC) was 29.28±6.90 pg and 33.47±2.63% respectively. The red cell distribution width (RDW-CV) showed a varied range from 12.5 to 31.6% with a mean of 17.45±3.77%. The mean hematocrit (Hct) value was 27.34±6.35%. (Table 3)
On peripheral smear examination, RBC morphology was evaluated for anaemia. It was found that microcytic hypochromic anaemic pattern was observed in the majority of the patients (42%), which was followed by the dimorphic pattern of RBCs in 26% cases. The normocytic normochromic and macrocytic pattern was found in only 19% and 13% cases respectively (Table 4)
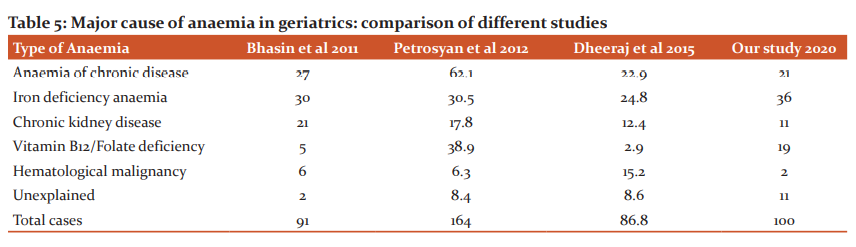
Table 5 evaluates the cause of anaemia in our study and compares the prevalence of each case with the findings of the other studies in the literature based upon anaemia in the geriatric age group.
DISCUSSION
Anaemia is not a disease, but an entity underlying many diseases. It is one of the most common blood disorder found in clinical practice as well as in laboratory investigations, affecting almost one-third of the population all over the world.14 Studying anaemia in geriatric patients is important as it is associated with many complications which deteriorate the quality of life.15 Anaemia also affects the work output of an individual as it leads to a decrease in oxygen supply to tissues.16 Prevalence has been seen to increase with the increase in age.17 Owing to its high prevalence, anaemia is studied widely and it is necessary to classify it so that to evaluate the cause of anaemia. This needs to be diagnosed early as it can be easily missed due to its non-specific symptoms like fatigue, weakness, malaise which are common to ageing also.15
Hundred elderly patients (above or equal to 60 years), who came to our hospital and required Complete Blood Count (CBC) as the part of their management, their reports were taken from the hospital data and analysed in this study. Most of the patients were in the patients were in the age group of 60-69 years (68%) with the total male to female ratio of 1.3:1. A similar finding of elderly males affected more with anaemia as compared to women was observed in the study by Petrosyan et al,18 where 57% males were anaemic as compared to 50% females and more than 60% anaemic falling in the age group of 60-69 years. Male predominance was also seen in few other studies.19-22 But in studies like Jadhav M et al. and Singhal S et al. female predominance was found.23,24 The variation of gender varies from place to place and also the fact that male patients have always been more who have approached to a hospital for their illness as compared to females in a developing country like India, can contribute to the male predominance in this study.
Anaemia was classified based on haemoglobin level i.e. mild anaemia with haemoglobin >10mg/dl, moderate anaemia with haemoglobin in the range of 7-10 gm/dl and severe anaemia in cases of haemoglobin <7gm/dl. Majority of cases i.e. 53% were in the moderate anaemia group which was following Singhal et al.,24 but few other studies had the majority in a mild anaemic group.18,25-27 The mean haemoglobin was 9.09 gm/dl (moderate anaemia) which was similar to many other studies like Hafiz F et al. and Singhal S et al. where the mean haemoglobin was 8.1 gm/dl and 9.24gm/dl.24-25
In our study the mean MCV value (fl), MCH value (pg), MCHC value (g/dl) and RDW (%) of the patients was 87.25fl, 29.28pg, 33.47g/dl and 17.45% respectively. Hafiz et al and Sandhya V et al also reported mean MCV, MCH and MCHC of 82.72fl, 28.54pg, 33.33 g/dl and 81.09 fl, 25.2 pg, and 31.11 g/dl respectively.25,28 The mean RDW was 17.45±3.77%, which was higher than the normal range of 11-15%. The higher values of RDW correlated well with the dimorphic pattern on PBS, around 26 % cases of the total.
Anaemia is also broadly defined as an absolute decrease in the red cell mass.29 Direct measurement of red cell mass is difficult but an estimation of hematocrit (packed cell volume) can help understand the quantity of red cell mass particularly in cases of anaemia. The mean hematocrit was 27.34±6.35% and it showed a wide variation from 7.9 to 40.9% reflecting the degree of anaemia. A study found that lower hematocrit values of less than 33% of patients were found in 50% of patients at admission requiring blood transfusion as a treatment for anaemia.30
On peripheral blood smear examination, the microcytic hypochromic pattern of anaemia was predominant in this study (42%). The findings were similar in studies by Patel S et al, where majority i.e., 72% of cases were of microcystic pattern and was followed by normocytic pattern i.e. 24% cases.31 Mikayla JE et al. also reported 54% cases of microcytic anaemia amongst 165 cases of anaemia in geriatric age group and 31% of normocytic normochromic anaemia. 32 Only low MCV cannot be taken as microcytic anaemia, as there were many cases in which MCV was within normal limits in anaemia cases, but on PBS features of iron deficiency was quite expressive. It was also observed by studies like Goodnough et al. 30 This led to the importance of correlation between RBC indices and PBS for evaluating the aetiology.
Anaemia is a multifactorial disease.33 The major cause of anaemia was found to be iron deficiency anaemia (36%) and anaemia of chronic diseases (21%) which was also the case in the studies by Sharma et al, Petrosyan et al and Bhasin et al.15,18,34 It was followed by vitamin B12/folate deficiency and anaemia due to chronic kidney disease. Vegetarian diet and low socioeconomic status can be attributed as the one of the main reason behind the nutritional deficiency in Indian population as found to be during the clinical data obtained from the records of the patients. Similar reasons were also attributed for nutritional deficiency anaemia in a study by Patel et al.31 In our study only 11% cases had an unexplained etiology, whereas this has been a major cause in studies on geriatric population in developed nations. A study by Goodnough LT in Stanford University, California found that of the 142 anaemic elderly patients, 42 (37%) had unexplained anaemia of the elderly (UAE), which was followed by iron deficiency anaemia. They defined this entity (UAE) as hyperproliferative normocytic anaemia to which any cause of anaemia could not be attributed such as nutritional deficiency, CKD or inflammatory disease.30
We only included the patients who came to the hospital for treatment, which is just the tip of an iceberg. There is a need to evaluate the much greater population suffering from anaemia which is still hidden in the community, and people are incognizant to their illness and the morbidity associated with it. For this reason screening programs for anaemia needs to be organized on the community level.
CONCLUSION
Anaemia amongst the elderly is a health concern in both developed as well as developing countries, hence early diagnosis and treatment is essential. Only CBC parameters cannot help determine the cause or aetiology behind the anaemia, PBS correlation is equally important in evaluating the aetiology of the anaemia. The correlation of CBC parameters and the PBS examination plays an important role in laying down the foundation of the further investigations which need to be carried out to confirm the aetiology of anaemia and help in starting the preliminary treatment for anaemia. This aids in reducing morbidity and mortality due to anaemia.
References:
-
WHO, Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System, World Health Organization, Geneva, Switzerland, 2011.
-
Gaskell H, Derry S, Andrew Moore R, McQuay HJ. Prevalence of anaemia in older persons: a systematic review. BMC Geriatr 2008;8:1.
-
Census of India. Registrar General of India office, Government of India, India 2011.
-
Chaves PH, Carlson MC, Ferrucci L, Guralnik JM, Semba R, Fried LP. Association between mild anaemia and executive function impairment in community?dwelling older women: The women’s health and aging study II. J Am Geriatr Soc 2006;54:1429?35.
-
Atti AR, Palmer K, Volpato S, Zuliani G, Winblad B, Fratiglioni L. Anaemia increases the risk of dementia in cognitively intact elderly. Neurobiol Aging 2006;27:278?284.
-
Onder G, Penninx BW, Cesari M, Bandinelli S, Lauretani F, Bartali B, et al. Anaemia is associated with depression in older adults: Results from the In CHIANTI study. J Gerontol Biol Sci Med Sci 2005;60:1168?1172.
-
den Elzen WP, Willems JM, Westendorp RG, de Craen AJ, Assendelft WJ, Gussekloo J. Effect of anaemia and comorbidity on functional status and mortality in old age: results from the Leiden 85-plus Study. CMAJ 2009;181(3-4):151-157.
-
Culleton BF, Manns BJ, Zhang J, Tonelli M, Klarenbach S, Hemmelgarn BR. Impact of anaemia on hospitalization and mortality in older adults. Blood 2006;107(10):3841-3846.
-
World Health Organization. Definition of an older or elderly person. Available from: http://www.who.int/healthinfo/ survey/ageingdefnolder/en/index.html
-
WHO, Worldwide Prevalence of Anaemia 1993-2005, WHO Global Database on Anaemia, Geneva, Switzerland, 2008.
-
Nutritional anaemias. Report of a WHO scientific group. World Health Organ Tech Rep Ser 1968;405:5–37.
-
Ejaz F, Ahmed M, Hassan NA. Comparative study in the diagnosis of anaemia by Sysmex KX-21N hematology analyzer with peripheral blood smear. Int J Endor Health Sci Res 2013;1(2):89-92.
-
Jones KW. Evaluation of cell morphology and introduction to platelet and white blood cell morphology. In: Harmening D (ed). Clinical Hematology and fundamentals of hemostasis. Philadelphia; 2009: 93-116.
-
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet 2015;388(10053):1545-1602.
-
Bhasin A, Rao MY. Characteristics of anaemia in the elderly: A hospital based study in South India. Indian J Hematol Blood Transfus 2011;27:26-32.
-
Horton S, Levin C. Commentary on Evidence That Iron Deficiency Anaemia Causes Reduced Work Capacity. J Nutrition 2001;131(2):691S–696S.
-
Ershler WB, Sheng S, McKelvey J, Artz AS, Denduluri N, Tecson J, et al. Serum erythropoietin and ageing: a longitudinal analysis. J Am Geriatr Soc 2005;53(8):1360-1365.
-
Petrosyan I, Blaison G, Andrès E, Federici L. Anaemia in the elderly: etiologic profile in a prospective cohort of 95 hospitalized patients. Eur J Intern Med 2012;23:524-528.
-
Price EA, Mehra R, Holmes TH, Schrier SL. Anaemia in older persons:etiology and evaluation. Blood Cells Mol 2011;46;159–165.
-
Tay MRJ, Ong YY. Prevalence and risk factors of anaemia in older hospitalised patients. Proceedings of Singapore Healthcare 2011;20(2):71-79.
-
Bang SM, Lee JO, Kim YJ, Lee KW, Lim S, Kim JH, et al. Anaemia and activities of daily living in the Korean urban elderly population: results from the Korean Longitudinal Study on Health and Aging (KLoSHA). Ann Hematol 2013;92(1):59-65.
-
Contreras MM, Formiga F, Ferrer A, Chivite D, Padrós G, Montero A. Profile and prognosis of patients over 85 years old with anaemia living in the community. Octabaix Study. Rev Esp Geriatr Gerontol 2015;50(5):211-5.
-
Jadhav MV, Agarwal SA, Kadgi NV, Khedkar SS, Kulkarni KK, Kudrimoti JK. The utility of automated RBC parameters in the evaluation of anaemia. Int J Healthcare Biomed Res 2015;3(3):170-181.
-
Singhal S, Verma N, Rathi M, Singh N, Singh P, Sharma SP, et al. Can peripheral blood smear examination be replaced by automated haematology analyser – with special reference to anaemia? Int J Res Med Sci 2016;4(10):4563-4566.
-
Hafiz F, Mahajan S, Koul KK. Study of Morphological Patterns of Anaemia in Adults. J Dent Med Sci 2019;18(11):46-50.
-
Cherian M, Varghese RG. Factors contributing to geriatric anaemia. J Curr Res Sci Med 2016;2:98-101.
-
Melku M, Asefa W, Mohamednur A, Getachew T, Bazezew B, Workineh M, et al. Magnitude of Anaemia in Geriatric Population Visiting Outpatient Department at the University of Gondar Referral Hospital, Northwest Ethiopia: Implication for Community-Based Screening. Curr Gerontol Geriatr Res 2018;9(8):633-643.
-
Sandhya V, Rashmi GS. Correlation of peripheral smear with RBC indices and RBC histograms in the diagnosis of anaemia. Indian J Pathol Oncol 2017;4(2):242-246.
-
Conrad ME, Anaemia. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston: Butterworths; 1990. Chapter 147. https://www.ncbi.nlm.nih.gov/books/NBK254/.
-
Goodnough LT, Schrier SL. Evaluation and management of anaemia in the elderly. Am J Hematol 2014;89:88–96.
-
Patel S, Shah M, Patel J, Kumar N. Iron Deficiency Anaemia in Moderate to Severely Anaemia Patients. Guj Med J 2009;64(2):15-17.
-
Mukaya JE, Ddungu H, Ssali F, Shea T, Crowther MA. Prevalence and morphological types of anaemia and hookworm infestation in the medical emergency ward, Mulago Hospital, Uganda. S Afr Med J 2009;99:881-886.
-
Lanier JB, Park JJ, Callahan RC. Anaemia in Older Adults. Am Fam Physician 2018 Oct 1;98(7):437-442.
-
Sharma D, Suri V, Pannu AK, Attri SV, Varma N, Kochhar R, et al. Patterns of geriatric anaemia: A hospital-based observational study in North India. J Family Med Prim Care 2019 Mar;8(3):976-980.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





