IJCRR - 13(2), January, 2021
Pages: 176-181
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
Surgical Management of Distal Femur Fracture Using Anatomical Locking Compression Plate
Author: Aditya K. Agrawal, Anirudh Bansal, Sudheer Rawat, Shubham Kapadiya, Sarvang Desai, Paresh Golwala
Category: Healthcare
Abstract:Introduction: Distal femur fractures are common injuries and are mostly caused due to vehicular injuries in the middle-aged population. Operative treatment has been preferred in the current scenario with open reduction and internal fixation in these fractures. Objective: To observe the surgical outcome of distal femur fractures operated with anatomical locking compression plate. Methods: This is a prospective observational study in 24 patients (20 male and 4 female). We classified the fractures according to AO/OTA classification and the patients were treated accordingly with anatomical locking compression plating. Functional outcomes were assessed according to \"Schatzker and Lambert Score\" at final follow up. Results: The mean age of presentation at the time of injury in the present study was 40.6 years. Open fractures were seen in11 patients and associated ipsilateral limb injuries were seen in 8 and contralateral limb injuries were seen in 4 patients. The mean follows up in the present study was 9 months. There were 8 cases of infection with seven being superficial infection treated conservatively and one case hada deep infection which was treated with debridement and antibiotics.In our study, there were 79.2 % (n=19) excellent to good results and 20.8 % (n=5) fair outcome according to Schatzker and Lambert criteria). Conclusion: Distal femur fracture treated with anatomical locking compression plate needs careful anatomical reduction, rigid fixation, early knee mobilization and weight-bearing onsigns of healing with the early presentation to the hospital from the time of injury were the essential factors in achieving a better outcome for the patient.
Keywords: Distal femur fracture, Anatomical locking plate, Schatzker and Lambert scoring system, Soft tissue contractures, Rehabilitation, Vehicular accidents
Full Text:
INTRODUCTION
 Fractures in the distal femur have posed considerable therapeutic challenges throughout the history of fracture treatment. These fractures are usually comminuted and readily deformed because of muscle forces acting on the distal fragment. This results in functional impairment of the knee joint and ankle because of injury to the quadriceps system. The distal femur fractures also often occur in elderly patients withosteoporosis.1
Fractures in the distal femur have posed considerable therapeutic challenges throughout the history of fracture treatment. These fractures are usually comminuted and readily deformed because of muscle forces acting on the distal fragment. This results in functional impairment of the knee joint and ankle because of injury to the quadriceps system. The distal femur fractures also often occur in elderly patients withosteoporosis.1
Distal femur fractures occur at approximately one-tenth the rate of proximal femur fractures and makeup 6-7% of all femur fractures.2,3 The most common high energy me
chanism of injury is road traffic accident (53%) and the most common low energy mechanism is a simple fall (33%).4,5 These potentially serious injuries resulting in various degrees of permanent disability and continue to pose a therapeutic challenge to the orthopaedic surgeons, eventoday in achieving successful outcome. Various modes of treatment have been advocated by several authors. They vary from closed treatment with traction, application of cast brace following preliminary traction, open reduction and internal fixation with a variety of implants.
Elderly patients and osteoporosis add to the difficulty in intra-articular fractures. Loss of stable fixation is of great concern. The Locking compression plate has added advantages in these patients.6 Despite the advance in techniques and the improvement in surgical implants, treatment of distal femoral fractures remains a challenge in many situations.1 Anatomic reduction of the articular surface, restoration of limb alignment, and early mobilization are effective ways of managing most distal femoral fractures.7
The locking compression plate has the advantage of the combination of compression plating, locked plating and bridge plating.8-10 This reduces soft tissue damage and periosteal vessels are preserved. Therefore, it acts as a closed external fixator.11 In this study, we evaluated the results of distal femur fractures treated with distal femur anatomical locking compression plate, their clinical, radiological outcomes & complications.
MATERIALS AND METHODS
 The prospective study was carried out in the selected group of patients treated in the Department of Orthopedics at the tertiary care district hospital.Study was conducted on consecutive 24 patients diagnosed with distal femur fractures presented to the casualty and orthopaedic department from November 2016 to October 2018, after taking written and informed consent. The study was approved by the Ethics Committee of the university (SVIEC/ Medi/BNPG15/D16208).
The prospective study was carried out in the selected group of patients treated in the Department of Orthopedics at the tertiary care district hospital.Study was conducted on consecutive 24 patients diagnosed with distal femur fractures presented to the casualty and orthopaedic department from November 2016 to October 2018, after taking written and informed consent. The study was approved by the Ethics Committee of the university (SVIEC/ Medi/BNPG15/D16208).
Patients were selected according to the inclusion criteria of the study and were briefed about the nature of the study, intervention to be done and post-operative rehabilitation. Inclusion Criteria included patient aged 18 years and above, the fractures of the distal femoral metaphyseal, metaphyseal-diaphyseal with or without intra-articular extension and distal third fractures of the femur, comminuted distal femur fracture, close fractures, fractures with Gustilo Anderson open grade I and II wounds were also included. The exclusion criteria included patients who didn’t want to participate in this programme, patients under 18 years of age, patients medically unfit for surgery and patients who did not have minimum six months followup.
All the patients were treated according to a protocol which consisted of standard antero-posterior and lateral digital X-ray and pre-operative CT scan. Open wounds were taken to the operation theatre for wound debridement within 5 hours ofadmission. Polytrauma patients were fixed as soon as their general condition allowed for surgery. Passive quadriceps exercises were started after 3-5 days post-operative.The patient was discharged with non-weight bearing walking for 12-16 weeks depending on the fracture pattern. Partial weight-bearing was started after early signs of the clinical and radiological union. Patients were followed up depending on the clinical examination as well as the radiological findings ofthe union. The statistical analysis was done using SPSS software (Illinois, Chicago) with a p-value less than 0.05 considered as statistically significant.
RESULTS
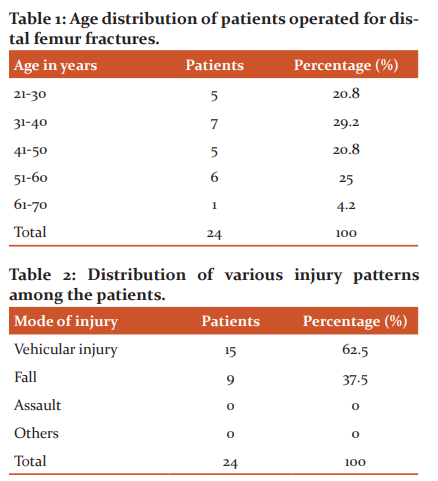
The prospective study was carried out in the selected group of patients treated in the Dept Orthopedics of a tertiary care district hospital from November 2016 to October 2018 on 24 consecutive patients. These included closed as well as open injuries and polytrauma patients. The average age of our present study was 40.6 years. The youngest patient in ourstudy was 21 years and the oldest patient in our study was 68 years. There were 17 patients below 50 years of age and only 1 patient above the age of 61 years. We observed more of the young active population in our study. In our study, there was a male preponderance (n=20, 83.33%). It is generally observed that the number of males out ranks females in a trauma series in ourcountry.
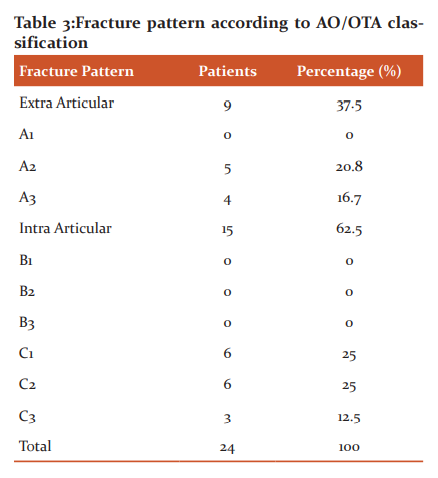
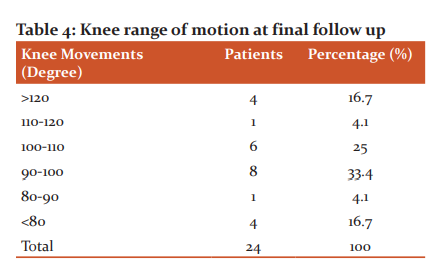
Manual labourer and farmer sustained a maximum injury to the distal end of the femur. Vehicular accident and fall from height were the main modes of injuries in our study fordistal end of femur fractures. In our study, there were 13 cases of closed injuries (54.2%) and 11 cases of open injuries (45.8%) in which Gustilo Anderson Grade-I and Grade-II were (25%) & (20.8%) respectively. According to AO/OTA classification, Type–A accounted for 37.5%, Type B accounted for 0% and Type C accounted for 62.5% fracture in our study. Half of the patients (n=12, 50%) were operated within 2 days of admission.
In our study 19 patients (79.2%) were fixed with distal femur lock compression plate (DFLCP) as definitive treatment primarily and 5 patients (20.8%) were fixed with DFLCP in second procedure due to the presence of open grade II fractures fixed with external fixator primarily. In our study, 62.5% (15 patients) required only one surgical procedure followed by five patients who required two surgeries due to open injuries and three patients who required more than two surgical procedures due to post-operative complications (infection and non-union). The average time of hospitalization in our studywas 18.8 days. In our study, the most common complication was an infection which occurred in eightpatients (33.3%). Seven patients had developed a superficial infection and one patient had developed a deepinfection. All patients except one resolved with intravenous antibiotics for two weeks and regular dressing. One patient had to get operated for debridement. The second most common complication was fatembolism which occurred in 2 patients (8.3%) developed on second and third days after the operation and had recovered with treatment (oxygenation & heparinisation). Seven (29.2%) patients had knee joint stiffness at long term follow up. The rate ofmal-union was 8.3% (n=2 patients) due to comminuted fracture type, delayed union was 8.3% (n=2 patients) and non-union was 4.2% (n=1 patient where additional bone grafting was done). The average time of union in our studywas18.2 wks. Majority of fractures (75%) united in between (15-20) weeks. The rate of fracture union in our study with anatomical locking compression plate was 95.8%. Out of 24 patients, only one patient had non-union and three patients developed union at >20 weeks follow up. In our study, 66.7% of patients (n=16) returned to their previous occupation while 12.5% of patients (n=3) had to change their occupation (clerical from manual).7,8,9
In the present study 16 (66.7%) patients had no shortening, 5 (20.8%) had to shorten less than 1.5 cm, 2 (8.3%) had shortening in between 1.5-2.5cm. All seven patients were given shoe compensation as they denied further surgical intervention. In our study total, 5 (21%) patients developed fixed flexion deformity (10±2°, range 5-23°). All five patients had open fracture grade II. All patients opted for aggressive physiotherapy and continuous passive motion devices. In our study, there were 79.2% (n=19) excellent to good results and20.8% (n=5) fair outcome according to SCHATZKER AND LAMBERT’criteria. The fair results were due to open type of injury, more than two surgical procedures, presence of deep infection, shortening and fixed flexion deformity of the knee due to soft tissue contractures.
DISCUSSION
An impacted linear or slightly displaced fracture results from a trivialtrauma to the flexed knee from the anterior and slightly medial aspect ofthe knee. Usually, this kind of fracture pattern is seen in an osteoporoticbone. A violent force applied on the anterolateral side of the flexed kneeproduces an oblique fracture extending just proximal to the lateral epicondyle to well above the medial epicondyle. A transverse fracture is produced by severe force applied to the lateral side of the extended limb. This usually produces a condylar segment which islonger on the lateral side classically seen when a limb is struck by a motor vehicle at the knee.10,11
The extensive force applied to the anterior aspect of the flexed knee, as in afall from a height or a ‘DASHBOARD’ injury, produces conjoined fracture of the distal femur extending on the shaft of the femur with communication. Compression adduction forces on knee joint produce condylar fractures. Shearing force when applied right angle to the articular surface of the distal end of femur produces a fracture line parallel to the direction of the force. This is the mechanism of injury in most cases of distal femur fracturewith an inter-condylar extension. The quadriceps and the hamstrings produce longitudinal tension, which tends to produce overriding and angulation of the fragments, driving the proximal fragment into the supra-patellarpouch, and hence causing further displacement and haemorrhage. The posterior angulation and displacement of the distal fragment are caused by the strong pull of gastrocnemius.
There is much controversy regarding the best method of treatment for the distal femur fractures, as most of the time-poor results are obtained. In the past, closed treatment with traction, application of cast following preliminary traction was used forthe treatment of open and close distal femur fractures. Outcomes after non-operative treatment were generally unsatisfactory, with a high incidence of fixed flexion deformity, varus mal-alignment, valgus mal-alignment, shortening and mal-rotation. As a result, since the late 1970s, opens reduction and internal fixation through plateosteo synthesis has emerged as the gold standard of operative therapy.


 In our study, most of the patients belong to the 4th decade (31-40 years) which included 7 (29.2%) patients. The mean age was 40.6 yrs which was almost equivalent to the study of Vishwanath C et al.,12 of 44.0 yrs (range 22-74yrs). All trauma series have high male preponderance. Similarly, we also had a maximum male preponderance with a ratio of male to female of 5:1. In Vishwanath C et al. study, out of 50 patients, there were 32 male & 18 females. Hence, the male to female ratio was 1.7:1 and in Sabarisree M et al.,13 male to female ratio was 2:1. Males are inmajority as they comprise the majority of the earning population who drive for long distance daily. In our study, the most common mode of trauma was motorcycle accidents in 62.5% (15 patients), which is comparable to the study conducted by Vishwanath et al., (66%). In our country, motorcycles are the most common mode of transport in youngmales who are the bread earners of the family. With the rapid increase in populationand number of vehicles plying on the roads in a developing country like ours, the relative expansion and maintenance of roads are not adequate and so the number of road traffic accidents are increasing along with the pattern of injuries.
In our study, most of the patients belong to the 4th decade (31-40 years) which included 7 (29.2%) patients. The mean age was 40.6 yrs which was almost equivalent to the study of Vishwanath C et al.,12 of 44.0 yrs (range 22-74yrs). All trauma series have high male preponderance. Similarly, we also had a maximum male preponderance with a ratio of male to female of 5:1. In Vishwanath C et al. study, out of 50 patients, there were 32 male & 18 females. Hence, the male to female ratio was 1.7:1 and in Sabarisree M et al.,13 male to female ratio was 2:1. Males are inmajority as they comprise the majority of the earning population who drive for long distance daily. In our study, the most common mode of trauma was motorcycle accidents in 62.5% (15 patients), which is comparable to the study conducted by Vishwanath et al., (66%). In our country, motorcycles are the most common mode of transport in youngmales who are the bread earners of the family. With the rapid increase in populationand number of vehicles plying on the roads in a developing country like ours, the relative expansion and maintenance of roads are not adequate and so the number of road traffic accidents are increasing along with the pattern of injuries.

 In our study, the right side was most commonly injured in 66.6% (16 patients) who were comparable to the study done by Vishwanath et al., (66%). Most of the patients had right side involvement and it’s due to left lane driving pattern in our country making right lower limb more vulnerable in the head-on collisions. 33.4% (8 patients) had a left-sided injury in our study. In our study, out of 24 patients, 13 (54.2%) patients had closed fractures and 11(45.8%) patients had open fractures. This shows the gravity of injury and damage to the soft tissue envelope which is vital for healing. Open fractures are one of the most challenging injuries to a trauma surgeon. Compared to closed fractures, they have a significantly higher risk of infection, delay in wound healing, high rate of non-union and often require multiple surgeries for definitive care. This in turn poses a mental trauma to the patient. In our study, the average hospital stay was 18.8 days which was comparable to 17.2 days in the study done by Yeap et al.14 The shortest stay was 5 days. The longest stay was 61 days in a patient who had open grade 2 distal femur fracture along withboth bone forearm fracture, proximal tibia fracture and 2,3,4 metatarsal fracture on the same side. External fixator for the femur and proximal tibia, rush pin and K- the wire was done as additional procedures for associated fractures.
In our study, the right side was most commonly injured in 66.6% (16 patients) who were comparable to the study done by Vishwanath et al., (66%). Most of the patients had right side involvement and it’s due to left lane driving pattern in our country making right lower limb more vulnerable in the head-on collisions. 33.4% (8 patients) had a left-sided injury in our study. In our study, out of 24 patients, 13 (54.2%) patients had closed fractures and 11(45.8%) patients had open fractures. This shows the gravity of injury and damage to the soft tissue envelope which is vital for healing. Open fractures are one of the most challenging injuries to a trauma surgeon. Compared to closed fractures, they have a significantly higher risk of infection, delay in wound healing, high rate of non-union and often require multiple surgeries for definitive care. This in turn poses a mental trauma to the patient. In our study, the average hospital stay was 18.8 days which was comparable to 17.2 days in the study done by Yeap et al.14 The shortest stay was 5 days. The longest stay was 61 days in a patient who had open grade 2 distal femur fracture along withboth bone forearm fracture, proximal tibia fracture and 2,3,4 metatarsal fracture on the same side. External fixator for the femur and proximal tibia, rush pin and K- the wire was done as additional procedures for associated fractures.
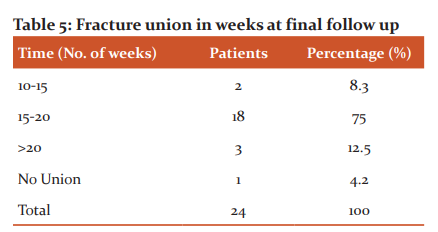
In our study, the average union time was 18.2 weeks who had a union at final follow up.This is comparable to study done by Vishwanath et al., which states average union as 13 weeks and Satish et al which states average union as 19.3 weeks. Rate of the union inour study was 95% which was similar to the studies of Vishwanath et al., (95%) Full knee range of motion (flexion & extension) was attained in 5 of our patients. Because of restricted knee movements, 58.3% of ourpatients had either difficulty or inability to squat. 54.2% of patients had either difficulty or inability to sit cross-legged. The possible causes for restriction of knee movement in our study were associated quadriceps injury, intra-articular comminution, open injuries leading to development of intra-articular adhesions andextra-articular adhesion of quadriceps.
CONCLUSION
The present study on surgical outcome of distal femur fracture treated with anatomical locking compression plate was done at our institute from November 2016 to October 2018. In our study there were 79.2% ( n=19) excellent to good results and 20.8 % (n=5) fair outcome according to SCHATZKER AND LAMBERT’ criteria). The fair results were due to open type of injury, more than two surgical procedures, presence of deep infection, shortening and fixed flexion deformity of the knee due to soft tissue contractures. Open, comminuted and fractures with intra-articular extension had more number of unsatisfactory results. Incidence of infection was comparatively more in open cases due to late presentation as discussed earlier. Proper and adequate debridement is mandatory to minimize the incidence of infection in open cases. In accordance with knee range of motion, 5 (20.8%) patients had less than 90 degrees of range of motion. So we conclude that rigid fixation after anatomical reduction followed by early mobilization of the knee should be implemented in allcases. Injury to quadriceps mechanism or impingement to quadriceps mechanism should be recognized early and should be taken care of, to prevent extensor lag and fixed flexion deformity of the knee.
ACKNOWLEDGEMENT: Authors would like to express their gratitude towards the Department of Orthopedics, Smt. B. K. Shah Medical College and Research Centre, Piparia, Vadodara and Hospital management for their constant support encouragement for the successful completion of the study and utilizing the facilities. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. They are also thankful to the subjects of this study for their valuable participation. Authors also grateful to IJCRR editorial team and reviewers to bring quality of this manuscript.
CONFLICT OF INTEREST: NONE
SOURCE OF FUNDING: NONE

Figure 1: A. 68 years old female with Type- A extra- articular distal femur fracture B. operated with distal femur anatomical plating C. Patient shows good results of knee extension at 12 weeks followup. D. Patient shows good results of knee extension at 12 weeks followup.

Figure 2: A. 42 years old male with Open Type-C distal femur fracture B. Patient was operated primarily with external fixator. C & D. This was followed by distal femur anatomical plating E. Patient with knee extension showing fair result at 12 weeks follow up. F. Patient with knee extension showing fair result at 12 weeks follow up.
References:
1. Brown A, D'Arcy J. Internal fixation for supracondylar fractures of the femur in the elderly patient. J Bone Joint Surg1971;53-B(3):420-424.
2. EnnekingW, Horowitz M. The Intra-Articular Effects of Immobilization on the Human Knee. J Bone Joint Surg 1972;54(5):973-985.
3. Connolly J, King P. Closed Reduction and Early Cast-Brace Ambulation in the Treatment of Femoral Fractures. J Bone Joint Surg 1973;55(8):1559-1580.
4. Pavel A, Smith R, Ballard A, Larsen A. Prophylactic Antibiotics in Clean Orthopaedic Surgery. J Bone Joint Surg 1974;56(4):777-782.
5. Schatzker J, Horne G, Waddell J. The Toronto experience with the supracondylar fracture of the femur, 1966–1972. Injury 1974;6(2):113-128.
6. Gustilo R, Anderson J. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones. J Bone Joint Surg 1976;58(4):453-458.
7. Zickel R, Fietti V, Lawsing J, Van B. Cochran G. A New Intramedullary Fixation Device for the Distal Third of the Femur. Clin Orthop Relat Res 1977;12:185-191.
8. Patterson B, Benirshcke S, Mayo K, Henley M. Comminuted, Intraarticular Fractures of the Distal Femur. J Orthop Trauma 1993;7(2):170.
9. Kolmert L, Wulff K. Epidemiology and Treatment of Distal Femoral Fractures in Adults. Acta Orthop Scandinavica 1982;53(6):957-962.
10. Mize R, Bucholz R, Grogan D. Surgical treatment of displaced, comminuted fractures of the distal end of the femur. J Bone Joint Surg 1982;64(6):871-879.
11. Papagiannopoulos G, Clement D. Treatment of fractures of the distal third of the femur. A prospective trial of the Derby intramedullary nail. J Bone Joint Surg 1987;69-B(1):67-70.
12. Machhi R, Namsha B, Namsha V. Surgical outcome of distal femur fracture by locking compression plate. Int J Orthop Sci 2016;2(4d):233-239.
13. Babu S, Sunku N. A Study on Functional Outcome of Comminuted Supracondylar Fracture Femur Treated by Plating with Fibular Bone Grafting. J Bone Rep Recom 2017;03(01).
14. Yeap E, Deepak A. Distal Femoral Locking Compression Plate Fixation in Distal Femoral Fractures: Early Results. Malaysian Orth J 2007;1(1):12-17.
15. Rajaiah D, Ramana Y, Srinivas K. A study of surgical management of distal femoral fractures by distal femoral locking compression plate osteosynthesis. J Evid Based Med Healthcare 2016;3(66):3584-3587.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





