IJCRR - 13(2), January, 2021
Pages: 164-168
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
Socio-demographic Profile of Snakebite Fatalities: An Autopsy based Study from Eastern India
Author: Deepsekhar Dalal, Tanmay Sardar, Saswata Biswas, Arijit Dey
Category: Healthcare
Abstract:Introduction: World Health Organization considers snakebite envenoming as priority neglected tropical diseases. India contributes to 50 per cent of the estimated deaths due to venomous snakebites globally. People from rural areas still believe on traditional healers instead of hospitalisation. Objectives: To depict the socio-demographic analysis of fatal snakebite envenomation by examining medicolegal autopsy in a government medical college in Kolkata, West Bengal. Methods: Total 125 hospitalised snake bite cases with fatal outcome, undergoing autopsy were examined. Sex, age, occupation, socio-economic status of the victims, seasonal variation, time and site of the bite was noted in proforma and analysed. Results: Males, engaged in agricultural activities were mostly the victims who suffered snake bites on their lower limbs in most of the cases. Cases increase in monsoon season. Snake bites occur in highest numbers during the daytime between 6 AM12Noon. Amongst the identifiable species, Krait was responsible for most of the fatalities.37.6% of victims died within the first day, while another 50% died within two weeks after the snakebite. More than 80% of victims were taken to a local therapist/ quack before they were hospitalized. Only 10 patients (8%) were brought within 3 hours after snakebite, while 48% (60) patients were hospitalized within 3-6 hours after the bite and in 15 cases (12%), more than 12 hours elapsed between snakebite and hospitalization. Conclusion: Fatality due to snake bite is preventable. Use of protective gears while working in the field, quick hospitalisation after a snake bite and timely administration of Anti Snake Venom can prevent or reduce its morbidity or mortality.
Keywords: Anti Snake Venom, Farmers, Krait, Lower limb, Snakebite
Full Text:
Introduction
Snakebite envenoming was added to World Health Organization (WHO) priority list of neglected tropical diseases (NTDs) in June 2017.1 Although there are currently more than 3000 species of snakes in the world, approximately 250 of these are listed by WHO as being of medical importance because of the harm their venoms can do.1 In tropical and subtropical countries, snake bite is a major health problem. There is evidence that globally 4.5-5.4 million people are bitten by snakes annually, 1.8-2.7million of them develop clinical illness (envenoming) after snakebite, and the death toll could range from 81,000 to 138,000. Amidst the variable distribution of envenoming and mortality worldwide, it is highest in Sub-Saharan Africa, South Asia and South-East Asia.2 India contributes to 50 per cent of the estimated deaths due to venomous snakebites globally.3 Snake bite cases, although a common medical emergency, mainly affects the rural population, who rather than going to the nearest hospital, often depend on local traditional healers for initial treatment and thus increasing the mortality. The present socio-demographic study was conducted on fatal cases of snakebite envenomation undergoing medicolegal autopsy in a government medical college in Kolkata, West Bengal to depict the current scenario prevailing in this state.
Material AND Methods
This study was conducted on fatal snakebite victims, subjected to medico-legal autopsy at the Department of Forensic Medicine& Toxicology, Nil RatanSircar Medical College and hospital, Kolkatabetween July 2014 to June 2016 (two years). Proper approval was obtained from the Institutional Ethics Committee before the commencement of study. Only hospitalized cases with a prior confirmed history of snakebite or local findings corresponding to snakebite were included in this study while brought dead cases were excluded. The details regarding age, sex, the month of occurrence, residence, were obtained from the inquest papers and Bed Head Tickets. In each case the accompanying relatives were questioned about the circumstances of the bite, time is taken to reach the hospital, reasons for delay if any and socio-economic status (based on Modified Kuppuswamy scale). Information about the snakebite, such as identification of snake, time of snakebite, pre-hospital care, latency between bites and admission were gathered from hospital treatment records. During an autopsy, sites of bites on the body were noted. All these data were entered in a standard proforma and analysed using standard statistical tools and represented in the form of graphs and charts.
Results
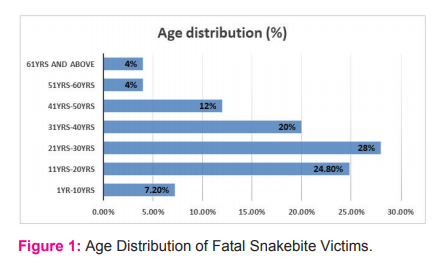
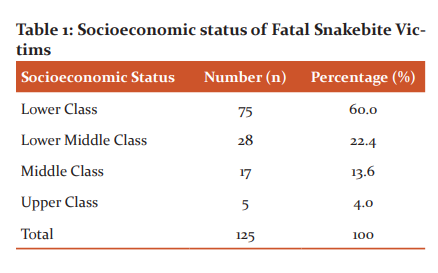
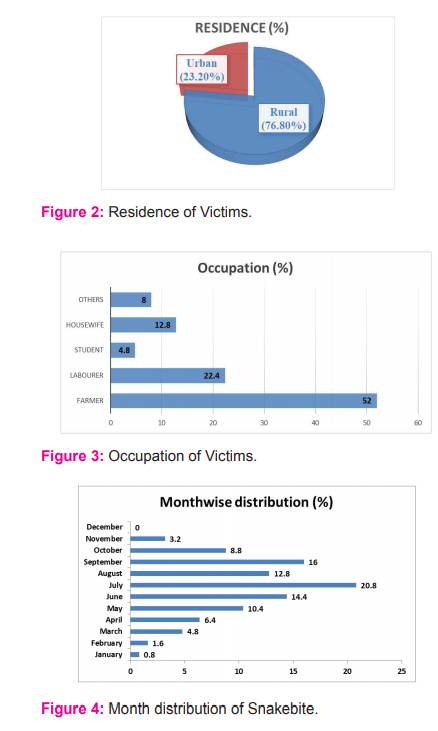
Out of a total 5589 autopsies conducted between July 2014 to June 2016, 125 (2.2%)cases were hospitalised snakebite cases which proved fatal and sent for autopsy. Majority of the victims were male (61.6%, 77) and male to female ratio was 1.6:1. As shown in Figure 1, the most commonly affected age group was 21-30years (28%, 35), followed by 11-20 years (24.8%, 31). The snakebite victims mostly belonged to the lower socio-economic class (60%, 75) [Table 1] and rural population was more affected(76.8%, 96) than its urban counterpart, as seen in Figure 2. The most common occupation involved was that of farmers (52%, 65) and labourers (22.4%, 28), as shown in Figure 3. July (20.8%, 26), September (16%, 20) and June (14.4%, 18) recorded the highest number of cases in decreasing order of frequency while there was no fatality in December, as shown in Figure 4. The majority of snakebites (46.4%, 58) occurred in the early hours of the day (between 6 am to 12 noon), while the least cases were during 12 noon to 6 pm (8.8%, 11) [Table 2]. As seen in Table 3, the involved snake was identified in 50 instances (40%), the most common being Krait (23.2%, 29) followed by Cobra (9.6%, 12). The lower limb was the most preferred site of snakebite (54.4%, 68), followed by upper limb (25.6%, 32) and the least common site was facing/scalp (6.4%, 8) [Figure 5]. 37.6% (47) victims died within the first day, while another 50% (63) died within two weeks and 12% (15) patients survived more than a fortnight following the snakebite [Table 4]. 101 patients (80.8%) were taken to a local therapist/quack before they were hospitalized, while the other 24 (19.2%) were directly brought to hospital [Table 5]. As far as the interval between snakebite and admission to hospital is concerned, only 10 patients (8%) were brought within 3 hours after snakebite, while 48% (60) patients were hospitalized within 3-6 hours after the bite and in 15 cases (12%), more than 12 hours elapsed between snakebite and hospitalization [Table 6].
Discussion
As per WHO, snakebite is one of the most neglected diseases that affect mainly the rural poor population.4In the present study, male to female ratio is 1.6:1; males were more affected owing to their outdoor activities than their female counterpart which is similar to previous studies from Madhya Pradesh 5 Maharashtra6and Karnataka.7 Studies from other countries also indicate male victim preponderance; male: female ratio was reported as 1.9:1 in a study from Thailand8 and 1.3:1 in another study from Pakistan.9 Although in the current study, all the age groups faced fatal outcomes, 21-30 years carried the most brunt like some other previous studies where 21-50 years ago group were mostly at danger.10 Sharp decline of fatalities after the 60 years of age is most probably due to less agricultural works by older people. Another cause may be less outdoor movement by the older persons after the evening.11 Globally, snakebites affect people in rural areas disproportionately.12-14 In this study snakebite mortality was around 3.3 times higher in the rural than an urban setting. Several reasons for higher rural mortality have been reported by previous studies, such as poorly constructed housing, increased agricultural work, treatment-seeking from traditional healers, and limited access to anti-venom therapy.15 Availability and accessibility of anti-venom is known to be limited in sub-Saharan Africa and Asia,16-18 resulting in a supply-price mismatch affecting medical treatment for the rural population and lower confidence in the public health sector's ability to provide effective and safe anti-venom.19,20 Several other kinds of literature also found higher incidences of snakebite cases in rural population. Farmers (52%) were the highest amongst the victims which are at par with other literatures.21,22 This may be attributed to working barefoot in the fields, not using protective gears like footwear etc. Snake bites are common during daytime23 and so was the finding in this study. Most of the bites occurred between 6 am to 12 noon. Studies conducted in Davangere21 and Maharashtra24 also reported high incidence during day time. This higher proportion in the earlier hours of the day corresponds to the increased outdoor activity time. Although, similar studies conducted in other parts of the country showed a relatively higher incidence of snakebite cases between 6:00 PM and midnight25-27 unlike the findings in our study.Seasonal peaks of snakebite incidences are usually associated with rainy seasons, associated agricultural activity and the profusion of prey organisms like frogs.28 Most human snakebites occur during the monsoon season because of flooding of the habitat of snakes and their prey. The breeding habits of frogs closely follow the monsoons and rats and mice are always close to human dwellings. 21 July, September, June and August hold the highest position in terms of the number of victims in decreasing order of frequency which corresponds with the monsoon season in West Bengal. November, December, January and February had very few cases due to hibernation of the reptile in the winter season. Lower limbs (54.4%) were the most preferable site for a bite which is in concurrence with other previous studies.10,21,25,29 Barefoot farmers working in poor visibility during the monsoon seasons in day time along with chances of accidental stomping on the snakes when the fields are full of their prey, can be attributed for this. Harrison RA30,31 found a positive correlation between snake envenomation and poverty. In the current study, we found the lower socio-economic class to fall victims in most of the cases (56%). Modified Kuppuswamy Scale33 was used to derive the socio-economic status of the victims after interviewing the accompanying relatives, in all the cases. The involved snake was identified in 50 instances (40%), the most common being Krait (23.2%, 29) followed by Cobra (9.6%, 12).Out of the total of 125 victims, only 47 (37.6%) patients succumbed to the snakebite within the first day itself, while the 62.4% survived for a variable period after hospitalization. Only 12% of the victims survived for more than two weeks and they received haemodialysis and mechanical ventilation before they died. All patients that suffer venomous snake bite should be resuscitated as per Advanced Trauma Life®Support (ATLS®) guidelines.32 All the hospitalised cases received Anti Venom sera in this study population.The most rapid threat to life is with neurotoxic bites in which respiratory depression secondary to muscle paralysis is a frequent cause of mortality.33 Dialysis and a supportive treatment appear to be the mainstay of the therapy in the cases which are complicated by renal failure.35 More than 80% of the victims were initially taken to local faith healers and quacks, which is a common finding in Indian scenario, as similarly observed in other studies.7,10,11 In the present study, only 10 (8%) victims were brought to the tertiary hospital within the first 6 hours, while 88% (110) patients were hospitalized within 12 hours after suffering from the alleged snakebite, who were referred to the tertiary hospital after receiving initial treatment in primary and secondary level healthcare facilities. This time latency between bite and hospitalization depends on several factors like the time of day when the alleged bite occurred, the distance of victim from a tertiary hospital, awareness about the treatment of snakebite, etc. and it eventually plays a very important role in survivability of the patient after hospitalization.
Conclusion
Snakebite affects mainly the poor people residing in rural areas doing agricultural activities mostly. 21-30 years age group is most vulnerable whereas people more than 61years are less affected. Snakebite cases wax and wanes around the year, with most cases occurring during monsoon season. Victims are mostly bitten by snakes in early daytime. Public awareness programmes are necessary to prevent the victims from being taken initially to local traditional healers and so that the crucial first few hours can be utilized by giving appropriate care at tertiary healthcare facilities. Farmers should be encouraged to use protective gears while farming and Government should ensure proper safety of our feeders.
Ethical Clearance: Ethical Committee approval No. NMC/354, Dated 15/01/2014 of Nil Ratan Sircar Medical College, Kolkata, West Bengal.
Funding: None
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors/editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of Interest: None declared


References:
-
What is snakebite envenoming? Available at https://www.who.int/snakebites/disease/en/ (Accessed on 2nd June 2020)
-
Prevalence of snakebite envenoming-WHO. Available at https://www.who.int/snakebites/epidemiology/en (Accessed on 2nd June 2020)
-
Gutiérrez JM, Calvete JJ, Habib AG, Harrison RA, Williams DJ, Warrell DA. Snakebite envenoming. Nat Rev Dis Primers 2017;3:17063.
-
Mohapatra B, Warrell DA, Suraweera W, Bhatia P, Dhingra N, Jotkar RM, et al. Snakebite mortality in India: A nationally representative mortality survey. PLoS Negl Trop Dis 2011;5:e1018.
-
Kalantri S, Singh A, Joshi R, Malamba S, Ho C. Clinical predictors of in-hospital mortality in patients with snakebite: a retrospective study from a rural hospital in central India. Trop Med Int Health.2006;11:22–30.
-
Mulay DV, Kulkarni VA, Kulkarni SG, Kulkarni ND, Jaju RB. Clinical profile of snake bites at SRTR Medical College Hospital, Ambajogai (Maharashtra). Indian Med Gazette 1986;131:363-366.
-
Kulkarni ML, Anees S. Snake venom poisoning: experience with 633 cases. Indian Pediatr 1994;31:1239-1243.
-
Buranasin P. Snake bites at MaharatNakhonRatchasima Regional Hospital. Southeast Asian J Trop Med Public Health 1993;24:186-192.
-
Rano M. A study of snakebite cases. J Pak Med Assoc 1994;44:289.
-
Shetty AK, Jiri PS. Incidence of Snakebites in Belgaum. J Ind Acad Forensic Med 2010;32(2):139–141.
-
Majumder D, Sinha A, Bhattacharya SK, Ram R, Dasgupta U, Ram A. Epidemiological profile of snakebite in South 24 Parganas district of West Bengal with focus on underreporting of snakebite deaths. Ind J Public Health 2014;58:17-21.
-
World Health Organization. Prevalence of snakebite envenoming.: WHO; (Accessed on 02nd June 2020). Available from: http://www.who.int/snakebites/epidemiology/en/
-
Gutierrez JM, Warrell DA, Williams DJ, Jensen S, Brown N, Calvete JJ, et al. The need for full integration of snakebite envenoming within a global strategy to combat the neglected tropical diseases: the way forward. PLoS Negl Trop Dis 2013;7(6):e2162.
-
Chippaux JP. Snake-bites: an appraisal of the global situation. Bull WHO 1998;76(5):51-24.
-
Chippaux JP. Snakebite envenomation turns again into a neglected tropical disease! J Venom Anim Toxins Incl Trop Dis 2017;23:38.
-
Gutierrez JM, Burnouf T, Harrison RA, Calvete JJ, Brown N, Jensen SD, et al. A Call for Incorporating Social Research in the Global Struggle against Snakebite. PLoS Negl Trop Dis 2015;9(9):e0003960.
-
Williams D, Gutierrez JM, Harrison R, Warrell DA, White J, Winkel KD, et al. The Global Snake Bite Initiative: an antidote for snake bite. Lancet 2010;375(9708):89-91.
-
Chippaux JP, Massougbodji A, Diouf A, Balde CM, Boyer LV. Snake bites and antivenom shortage in Africa. Lancet 2015; 386(10010):2252-2253.
-
Brown NI. Consequences of neglect: analysis of the sub-Saharan African snake antivenom market and the global context. PLoS Negl Trop Dis 2012;6(6):e1670.
-
Dandona R, Kumar GA, Kharyal A, George S, Akbar M, Dandona L. Mortality due to snakebite and other venomous animals in the Indian state of Bihar: Findings from a representative mortality study. PLoS One 2018;13(6):e0198900.
-
Sharma N, Chauhan S, Faruqi S, Bhat P, Varma S. Snake envenomation in a north Indian hospital. Emerg Med J 2005;22:118-120.
-
Panna L, Srihari D, Rotti SB, Danabalan M, Kumar A. Epidemiological profile of snakebite cases admitted in Jipmer Hospital. Indian J Com Med 2005;26: 36-38.
-
Vishwanath B, Ganesh P. Demography, clinical profile, morbidity and mortality pattern of snakebite cases in children: a study at the tertiary teaching hospital, India. Int J Contemp Pediatr 2019;6:1472-1475.
-
Kulkarni RS, Sharma BD. Study of 1140 Cases of Poisonous Snakebite Envenomation In a Rural Hospital of South Konkan Coast of Maharashtra over a period of eight years (1986-1993). Indian Poisonous Snakes. 1stEdition. New Delhi: Anmol Publications Pvt. Ltd.; 2002:279-301.
-
Anjum A, Husain M, HanifSA, Ali SM, Beg M, et al. Epidemiological Profile of Snake Bite at Tertiary Care Hospital, North India. J Forensic Res 2012;3:146.
-
Suchithra N, Pappachan JM, Sujathan P. Snakebite envenoming in Kerala, south India: clinical profile and factors involved in adverse outcomes. Emerg Med J 2008; 25: 200-204.
-
Yoshi S, Honma M. Snakebites in India. Snake 1975;7(1):1-16.
-
Chandrakumar A, Suriyaprakash T.N.K, Linu Mohan P, Thomas L, Vikas PV. Evaluation of demographic and clinical profile of snakebite casualties presented at a tertiary care hospital in Kerala. Clin Epid Global Health 2016;4:140-145.
-
Hati AK, Mandal M, De MK, Mukherjee H, Hati RN: Epidemiology of snake bite in the district of Burdwan, West Bengal. J Indian Med Assoc 1992;90(6):145-147.
-
Harrison RA, Hargreaves A, Wagstaff SC, Faragher B, Lalloo DG. Snake Envenoming: A Disease of Poverty. PLoS Negl Trop Dis 2009;3(12):e569.
-
Kasturiratne A, Wickremasinghe AR, de Silva N, Gunawardena NK, Pathmeswaran A, et al. The Global Burden of Snakebite: A Literature Analysis and Modelling Based on Regional Estimates of Envenoming and Deaths. PLoS Med 2008;5:1591-1604.
-
American College of Surgeons Committee on Trauma. Advanced trauma life support for doctors [8th Edition], American College of Surgeons, Chicago, 2008.
-
Warrell DA. Snake Bite. Lancet 2008;375:77-88.
-
Harshavardhan L, Lokesh AJ, Tejeshwari HL, Halesha BR, Siddharama SM. A Study on The Acute Kidney Injury in Snake Bite Victims in A Tertiary Care Centre. J Clin Diagn Res 2013;7(5):853-856.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





