IJCRR - 13(2), January, 2021
Pages: 143-147
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
Foetal Anomalies: Correlative Study of Sonography and Autopsy
Author: Aiswarya Lekshmi RV, G Raju, K Chandrakumari
Category: Healthcare
Abstract:Background: Sonography is performed without risk to mother or foetus for a scientific anatomical survey of the external features and all organs related to each system. Objectives: In this study by comparing Ultrasound and Autopsy of intrauterine congenitally anomalous foetuses contrasting findings were detected. Methods: The results of Limb anomalies, Palmar crease defect, Cleft palate and Cleft lip, Club foot, Diaphragmatic hernia, Gastrointestinal anomalies like Omphalocele, Imperforate Anal defects are considered. Results: Four categorizations of anomalies with the comparison of Ultrasound and Autopsy findings are done. Conclusion: Categorization plan shows that each Ultrasound and Autopsy findings are influenced by Socio-economic status and Dietary habits. Early diagnosis of malformations and awareness to parents can be helpful for Medical termination of pregnancy and prevention in subsequent pregnancies.
Keywords: Autopsy, Categorization, Sonography
Full Text:
INTRODUCTION
The aim of this study is to analyse the potential use of Prenatal scan done throughout intrauterine life from 6-20 weeks for the assessment and diagnosis of defective embryological anomalies.Sonography is performed without risk to mother or foetus for a scientific anatomical survey of the external features and all organs related to each system.Two broad subsets of foetal anomalies are major and minor. Minor anomalies about 14% which won’t seriously interfere with viability or physical well being which can or cannot be detected during Prenatal sonography. In this study pattern of different embryological anomalies and sex ratios of foetuses were conducted.
Materials and methods
SOURCE
Fifty Antenatal Ultrasound scan reports of defective embryological anomalies and their foetal specimens obtained after medical termination of pregnancy or delivery.
Study Design
Descriptive Study Case series.
Data Analysis
Student t-test using SPSS Software version 17 and Microsoft Excel.
Materials
This study ( SGMC : IEC No.10/95/01/2014/) was conducted during the period of 2014 to July 2016. Ultrasound scanning reports obtained from Ittyavirah Scan Centre, Thiruvananthapuram. Specimens of those foetuses were obtained from various hospitals were delivery or medical termination was conducted including Placenta. Autopsy was conducted at Sree Gokulam Medical College & Research Foundation, Thiruvananthapuram.
Inclusion criteria
Embryologically defective foetuses detected by Autopsy, agreeing with their Ultrasound Scan reports.
Exclusion criteria
Embryologically defective foetuses whose Ultrasound Scan reports are not available.
Detailed recording of the history of the patients were obtained from parents in the form of a Proforma including
1. Maternal age
2. Duration of Gestation
3. History of Consanguineous marriage
4. Socio-economic status
5. History of the maternal consumption of medicine taken by the mother during pregnancy.
6. History of dietary habits
7. Exposure to radiation, chemicals.
8. History of abortions or still births.
9. Previous history of defective embryological anomalies.
10. Similar history in the family .
The cases were followed up till delivery or Medical termination of pregnancy at various hospitals in Thiruvananthapuram. The fetuses after expulsion / delivery were collected. The external appearances of the babies were examined & noted down and compared with the Ultrasound reports.
Collected foetuses and Placenta were obtained ranging from sixteen to twenty weeks of gestation were preserved in 10% formalin which is the fixative used.
Consent for Autopsy was obtained from parents after explaining the necessity. The Autopsies were conducted in the Department of Anatomy, Sree Gokulam Medical College after comparing with the Ultrasound report. Each foetuses were exploded using surgical knife, scissors and forceps. Internal findings correlated with the Ultrasound and other extra findings looked for. Updating of findings were done by Periodical photography. Placenta also studied.
OBSERVATION AND RESULTS
Correlating the findings of Prenatal, Ultrasound and Foetal Autopsy of the specimens of varied Congenital anomalies classification was done system wise under the following four categories.
Category A – Both findings (Ultrasound and Autopsy) were agreed.
Category B – Additional data of other anomalies detected.
Category C - Foetal autopsy revealed only certain Ultrasound findings.
Category D - Ultrasound and Autopsy findings were totally mismatching.
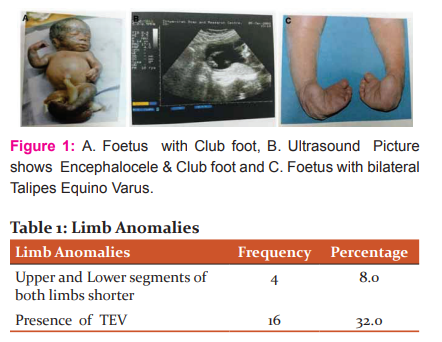
Limb Anomalies
Sixteen foetuses showed Talipes Equino Varus. Out of that four specimens had shortening of Upper and Lower segments of both limbs due to Skeletal dysplasias as given in Graph 1: Limb Anomalies and Table 1: Limb Anomalies.
Talipes Equino Varus
“A combination of talus and pes together with an elevated heel resembling that of a horse (L.Equinus, horse); which is also turned inwards (Varus).Inverted foot, Plantarflexed ankle, Adducted forefoot as shown in Fig 01,Fig 02 and Fig 03(turned toward the midline in an abnormal manner)”. Incidence is approximately one per thousand live births with males affected twice than females.1,2
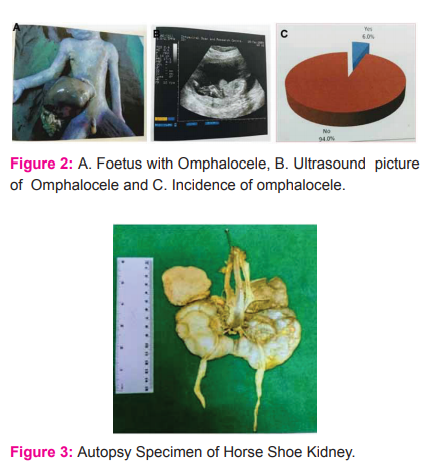
Three fetuses were there with Omphalocele as shown in Fig 04, Fig 05, Table 02 and Graph 02.
Other findings in one foetus
i. Short neck with oedema around
ii. Head twisted towards right
iii. Left lower limb absent
iv. Spine with Scoliosis
v. Right foot with 1,2 and 3 toes fused
vi. Ambiguous genitalia
vii. Omphalocele contain Intestine and Liver
viii. Umbilical cord contain one Umbilical artery.
ix. Kidney was Horse shoe shaped shown in Fig 06
Second specimen
i. Short neck
ii. Dysmorphic facies
iii. Fusion of digits of Hand and Feet.
iv. Left Foot Talipes Equino Varus.
v. Single Palmar Crease.
vi. Lungs were two lobbed.
Third Specimen
Presented only with Omphalocele.
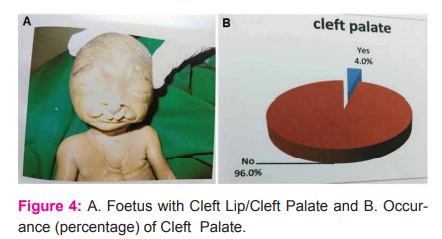
Cleft Palate
Cleft Palate constitute 4% of the total anomalies as shown in Table 3, Graph 3 and Fig 07. One was a male baby with dysmorphic facies, low set ears with flattened ear lobes, upper lip bilateral cleft lip with cleft palate, nose poorly formed, polydactyly with six digits in left hand and right foot, phallus is short with Hypospadiasis.
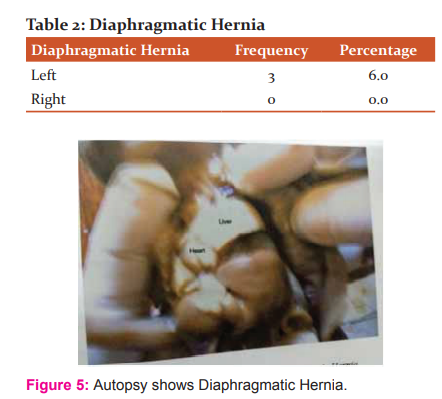
Diaphragmatic Hernia
There were three cases of Diaphragmatic Hernia which shows the frequency is more on the left side as shown in Table 4, Fig 08.
Imperforate Anus
Detected in three foetuses shown in Table 5, Graph 4. Two of them were with Mermaid syndrome .
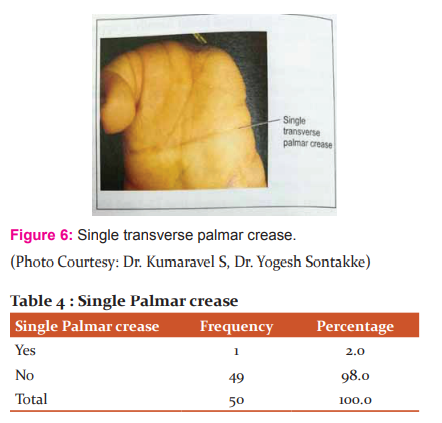
Single Palmar crease
It was hydrops baby with multiple Congenital anomalies, dysmorphic facies, short neck, fusion of digits of hand and feet, left foot Talipes Equino Varus, Single Palmar crease, Omphalocele and both lungs were two lobbed shown in Fig 09,Table 6 and Graph 5.
DISCUSSION
In this study Ultrasound and Foetal Autopsy findings of Foetuses up to 20 weeks of gestation were compared and contrasted; obtained four category results in which
Category A – Both findings (Ultrasound and Autopsy) were agreed.
Category B - Additional data of other systemic anomalies detected.
Category C - Foetal autopsy revealed only certain Ultrasound findings.
Category D – Ultrasound and Autopsy findings were totally mismatching.
Antonsson et al(3) examined Ultrasound and Autopsy on an equivalent methodological basis and came to a conclusion that autopsy could have significant limitation in CNS malformations. During this study we could ready to notice a high degree of correlation between Ultrasound and Autopsy in twenty two cases. 44% of Foetal anomalies revealed in Ultrasound were demonstrated in Autopsy also. These anomalies are grouped under Category A which incorporates neural tube defects, Cystic hygroma, Hydrops foetalis and Omphalocele.
Akgun et al(4) in 2007 concluded that analysis of Foetal autopsy following termination of pregnancy enables the diagnosis of anomalies which isn't detected by Ultrasound. In Category B, limb anomalies, Skeletal defects and Genitourinary anomalies are included mostly. Skeletal dysplasia are often revealed through Ultrasound, but confirmation is required from autopsy. Renal Cystic diseases could even be difficult to define on an Ultrasound scan as Oligohydramnios is usually associated. Other anomalies like Cardiovascular, Cleft lip / Cleft palate and Urinary tract defects are detected in autopsy (Category B) 38% .
Category C included mainly complex, CNS because it gets macerated due to improper preservation of the foetus after death and also due to the delay in autopsy. Moreover it should be borne in mind that certain conditions of expulsion hinder examination as they involve an excessively long period of foetal retention resulting in maceration in Utero and tissue lysis, of brain tissue especially and Cardiovascular anomalies like Valve insufficiencies due to the small size of the heart, Pericardial and Pleural effusions. Seven cases were included in Category C which constitute 14% of the entire anomalies.
In Category D there was total disagreement between Ultrasound and Autopsy. Two cases comes under Category D which constitute 4% of the entire anomalies.
Finally this categorization evidently shows that both Ultrasound and Autopsy may have some important limitations in diagnosing Foetal abnormalities and both are complementary.
The mothers who had undergone Ultrasound scanning and were found to be having Congenitally abnormal foetuses were grouped consistent with the Socio-economic status into High, Middle and Low income groups.
CONCLUSION
Reasons for Common defective embryological anomalies are
i. Genetic factors (Chromosome and Single gene mutation)
ii. Environmental factors (Infectious agents, Chemical compounds, Radiations)
iii. Use of medication by mother
iv. Maternal metabolic diseases
v. Multiple pregnancies
vi. Maternal stress
vii. Prematurity of the Infant.
By this study the potential and limitations of Ultrasound and Autopsy and categorization into four categories was possible. Even though Ultrasound fairly detects the malformations, Foetal autopsy is vital for obtaining extra information.Ultrasound findings rely upon the accuracy of the machine and the experience of the person. The Autopsy also depends on the ability and experience of a Specialist Paediatric Pathologist. Placental examination is also can give supportive findings like Macroscopic study of the Placenta, Position of Umbilical cord, Foetal and Maternal surfaces of the Placenta and Evidence of Placental infections. Earlier detection of Foetal anomalies by Ultrasound leads to early termination of Pregnancy without Autopsy. This results in missing important informations from Paediatric Pathologist which can cause risk of repetition in the subsequent pregnancies.
Defective embryologically malformed infants is prone for morbidity and mortality. Treatment and Rehabilitation of these infants is tough. Recovery is usually not possible. So early diagnosis, interpretation and awareness to parents is very crucial.
Conflicts of interest
All authors have none to declare.
Financial support and sponsorship
No funding to declare.
Acknowledgements
We acknowledge the contribution of Dr.Alex.K.Ittyavirah, Radiologist and Ultrasonologist, Ittyavirah Scan and Research Centre, Thiruvananthapuram and therefore the faculties of the department of Anatomy.
References:
1.Standring S.Development of Pelvic Girdle and Lowerlimb, R Shane Tubbs, Cheryll Tickle. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, Forty-first Edition, Elsevier.2016.9:1336. https://www.worldcat.org/title/grays-anatomy-the-anatomical-basis-of-clinical-practice/oclc/213447727 [last accessed on 2020, Oct 02]
2.Moore KL, Dalley FA, Agur MR Anne. Lower Limb. Clinically Oriented Anatomy, Sixth Edition, Wolters Kluwer (India). 2010.5:668. ISBN-13:978-81-8473-183-5.
3.AntonssonP,SundbergA,KublickasM.CorrelaionbetweenUltrasound&Autopsyfindingsafter2ndTrimesterterminationsofPregnancy.JPerinatMed.2008;36(1):59-69.doi:10.1515/JPM.2008.005.
4.Hulya Akgun, Mustafa Basbug,Mahmut TuncayOzgun.Correlation between Prenatal Ultrasound & Foetal Autopsyfindingsin Foetalano maliesterminatedinthesecondtrimester.Prenat. Diagn.2007;27:45762.doi:10.1002/pd.1710.
5.A.Kaasen, J.Tuveng, A.Heiberg et al. Correlation between Prenatal Ultrasound & autopsy findings: a study of secondtrimesterabortions. Ultrasound Obstet Gynecol.2006,28:925-933.doi:10.1002/uog.3871. https://obgyn.onlinelibrary.wiley.com/doi/10.1002/uog.3871 [last accessed on 2020,Oct 02]
6.Zhraa Abd-Alkader Taboo. Prevalence and Risk Factors for Congenital Anomalies in Mosul City.The Iraqi Postgraduate Medical Journal.2012, Volume11, Issue4, Pages458-470. https://www.iasj.net/iasj?func=article&aId=62828 [last accessed on 2020, Oct 02]
7.Reeka Pradhan, Sajeeb Mondal, Shouvanik Adhya, Gargi Ray Chaudhuri. Perinatal Autopsy: A study from India; JIndianAcadForensicMed.2013Jan-March, Vol. 35, No.1.ISSN0971-0973. https://www.researchgate.net/publication/286858542_Perinatal_autopsy_A_study_from_India [last accessed on 2020, Oct 02]
8.Hashan Amini, Per Antonsson, Nikos Papadogiannikis.Comparison of Ultrasound and autopsy findings in Pregnancies terminated due to foetal anomalies. Acta Obstetricia et Gynecologica Scandinavica. 2006;85:1208-1216.https://obgyn.onlinelibrary.wiley.com/doi/full/10.1080/00016340600880886 [last accessed on 2020,Oct 02]
9.Globus M S, Hall B D, Filly RA, PoskanzerLB.Prenatal diagnosis of achondrogenesis. J Paediatrics. 1977,91;464.
10.Santosand & Duenheolter.1975.
11.Carr D H.Heredity & the Embryo.Science J.1970,6:75.
12.Persaud T V N.Problems of Birth Defects.From Hippocrates to Thalidomide & after.Baltimore, University Park Press.1979
13.Chen-Chith J Sun, Kathy n Grumbach, Donna T. DeCosta.Correlation of Prenatal Ultrasound Diagnosis and Pathologic Findings in Foetal Anomalies, Paediatric & Developmental Pathology.1999, Vol, Issue 2:pp 131-142.
14.Zsanett Szigeti M D, Akos Csaba M D, Barbara Pete M D.Correlation of Prenatal Sonographic Diagnosis and Morphologic Findings of Foetal Autopsy in Foetuses with Trisomy 21.2002
15.Mandeep Singh Bindra.Congenital Malformation in Perinatal Autopsy.A Prospective Study.2010
16.Nayab Alia, Irshad Ahmed, Amir Hayat Maha is. Congenital Anomalies: Prevalence of Congenital anomalies in 2nd Trimester of Pregnancy in MadinaTeaching Hospital, Faisalabad on grayscale ultrasound. JUMDC,2010 Vol.1,Issue 1,Jan-Jun.
17.Rema Devi, Preetha Tilak, Sayee Rajangam.MultipleCongenitalanomalies-an aetiological Evaluation. Bombay Hospital Journal.2007
18.Kulkarni M L.Congenital malformation.Indian Paediatr 1989;26:5-9.
19.Bai N S, Mathew E, Nair PM, Sabrinathan K.Perinatal mortality during a South Indian Population. J Indian Med Assoc.1991;89:97-98.
20.Sharma A K.The Clinical Value of Perinatal Autopsy. Indian Paediatr.1994;31:5-7.
21.Valerie Desilets, Luc Laurier. Fetal and Perinatal Autopsy in Prenatally Diagnosed Foetal Abnormalities with Normal Karyotype. SOGC Technical Update. 2011;No-267:1047-1057.
22.Kobayashi,Fleisher,Sample,Brown,Leopold,Filly,Sanders and Winsberg.1960.
23.Arthur C, Fleischer M D, Sandra G, Krihner M D, and Grey A, Thoma MD. Prenatal detection of foetal anomalies with Ultrasonography. Pediatric Clinics of North America,1985, Vol.32, No.6.
24.TanakaK, MiyajimaG, WagaiT, YasuuraM. Detection of Intracranialanatomicalabnormalities by ultrasound.TokyoMed.J.1950,69:52.
25.Mishra P C, Baveja R.Congenital anomalies in Newborns A Prospective study.Indian Paediatrics. 1989Jan., Vol. 26.
26.GhoshS, BhargavaSK, BhtaniR; Congenitalanomaliesinlongitudinally studied birth cohortinaurban community. Indian J.Med. Res.Nov.1985,82:427.
27.MohanH, Bhardwaj, Bala. Congenital Visceral Malformations Role of Perinatal Autopsyindiagnosis. Foetaldiagnosisand Therapy.2004;19:131-133.
28.AiyarRR, AgarwalJR. Observationon Newborn: A Study of 10,000 consecutive live births. IndianPaediatr 1969;6:729-742.
29.Antonella Vimercati,Silvana Grasso,Marinella Abruzzese.Correlation between Ultrasound diagnosis and autopsy findings of foetal malformations.2010.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





