IJCRR - 13(2), January, 2021
Pages: 136-142
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
Management of Traumatic Wounds of Hand and Foot by Various Modalities: A Comparative Analysis
Author: Venkatesh Dasari, Naresh Kumar Dhaniwala, Sohael M. Khan, Vrushabh U. Kumbhare
Category: Healthcare
Abstract:Background: Hand and foot have lower blood supply as compared to face and scalp, leading to hindrance in wound healing. Delayed and/or inadequate treatment of these wounds may even lead to permanent disabilities. Despite the importance of this matter, there are no widely accepted protocols for the treatment of traumatic wounds of hand and foot which can provide the most optimal treatment to the patients. Objective: To study the outcome of management of traumatic wounds of hand and foot by various modalities and compare the results of the above modalities of wound management in terms of rate of healing, control of infection, and functional outcome. Methods: A total of 30 patients were enrolled in this study and divided into 3 groups with 3 different treatment modalities: A- Regular sterile dressings, B- Infiltration of platelet-rich plasma (PRP) at wound edges, and C - Split thickness skin grafting. Wounds were assessed serially by Bates Jensen Wound Assessment Tool (BJWAT) and skin grafting wounds were assessed by clinical points of graft acceptance, exudation, infection, contractures, etc. The functional outcome was quantified by the QuickDASH score for hand injuries, and the Foot and Ankle Ability Measure (FAAM) score for foot injuries. Results: Pre-treatment, the majority of the wounds were in the size range of 6-10 cm2. The pre-treatment mean BJWAT scores were 31.2 \?4.26, 33.2 \?4.80, and 32.2 \?4.52, in dressing group, PRP group, and Skin grafting group, respectively and it was not statistically significant. There was a statistically significant decrease in BJWAT scores in groups A and B by 9 weeks of treatment, but the PRP group showed a faster rate of healing. 80% of patients in the skin grafting group showed 'excellent' results. Most superior functional outcome scores of QuickDASH and FAAM were observed in the PRP group, followed by dressing and skin grafting groups. Conclusion: Platelet-rich plasma infiltration at wound edges provides a safe and effective treatment modality for the treatment of traumatic wounds of hand and foot.
Keywords: Management of Traumatic Wounds of Hand and Foot by Various Modalities: A Comparative Analysis
Full Text:
Introduction
Traumatic wounds are one of the most common problems seen in day to day life leading people to the hospital.1, 2 Amongst various age groups, children are prone to these injuries while playing outdoors or by household tools. Youth and adults are more likely to get injuries as occupational hazards during working with heavy machinery, as a result of assaults, railway accidents, and road traffic accidents(RTA) involving motorized vehicles leading the list.3 WHO reported 12 lakhs deaths around the world which were related to road traffic accidents in the year 2015, leaving millions more with an array of injuries and many with life-long adverse health consequences.4 India ranks fourth on the list of countries with the highest number of road traffic accidents.5
Trauma and its consequences lead to a heavy burden on the national economy and its individuals. In low- or moderate economy countries, the most affected age group is the one earning the bread in the family and contributing significantly to the working force of the society. With a huge population already below the poverty line in our country, trauma to the breadwinner of the family further worsens their poverty. This is due to loss of income to the family added with the burden of prolonged and costly medical care. Despite this being a large and preventable burden to human life, medical services, and the country’s economy, the measures to minimize the overall trouble have proved inadequate.4
The hands and feet are two very important structures of the human body that are highly functional and useful in activities of daily living (ADL). The hand and foot are the most functional part of the limbs, and hence more prone to traumatic injuries. They are the first, and sometimes the only body part in contact with the surrounding environment during trauma. Face and scalp have high vascularity and hence there are fewer chances of infection secondary to trauma. Relatively low vascularity in hand and foot makes them more prone to post-traumatic infections.6 All these factors make the hand and foot more prone to injury, its complications, long-standing disease, and even permanent deformity in some cases. Correct diagnosis and efficient management are essential to avoid complications.7
Traumatic wound management has had an unsettled history for centuries. The general approach to wound management involves local hemostasis, debridement, and primary closure. On failure or non-applicability of primary suturing, other modalities used are (i) regular dressing and healing of a wound by secondary epithelialization, (ii) infiltration of platelet-rich plasma at wound edges to help epithelization, and (iii) skin grafting. The most appropriate way to accomplish wound healing with a maximum functional and cosmetic gain is still debatable. The hand and foot are a common site of traumatic wounds and the most functional and important parts of human limbs, yet there are not many studies focusing on their wound management. In light of this paucity, the present work was undertaken with the aim of ‘studying the outcome of management of traumatic wounds of hand and foot by various modalities.’
Materials and Methods
This prospective study was conducted in the Department of Orthopaedics, Jawaharlal Nehru Medical College, and Acharya Vinoba Bhave Rural Hospital, Sawangi (Meghe), Wardha (MH), India. The material of the study was constituted by the patients presenting to the Orthopaedics outdoor department or Emergency Medicine department with traumatic injuries of hand and foot. Institutional ethics committee approval was obtained before proceeding with the research work.
Inclusion Criteria:
-
All traumatic wounds on hand and foot with or without tendon, muscles and bony injuries
-
Patients willing to participate in the study
Exclusion Criteria:
-
Traumatic wounds older than 1week from time of injury
-
Patients with uncontrolled diabetes mellitus
-
Patients not willing to participate in the study
On presentation, patients were submitted to a detailed history and clinical examination. A clinical diagnosis was made and necessary emergency medical& primary management was provided. On stabilization of a general condition, advised investigations were done. All patients were taken up for wound debridement at the earliest possible opportunity after stabilizing the general condition. Primary closure was attempted, wherever possible. Associated musculoskeletal injuries were managed as per established protocols.
A single dose of Injection Ceftriaxone 1gm intravenously (IV) was given to every patient at the time of admission and was continued bis in die for 3 days followed by tablet Cefixime 200mg orally twice daily for the next 5 days. Injection Metronidazole 400mg 8 hourly was given in selected patients having gross crushing and contamination to preventing anaerobic infections. Other necessary medical management for analgesia and supplementation was provided.
Thirty patients were enrolled in this research. An informed written consent, in the regional language, was obtained from the patients before enrolment. Systemic randomization of patients was done into 3 groups, each of 10 subjects. In group A, patients received conservative management in the form of regular sterile dressings, group B patients received infiltration of platelet-rich plasma (PRP) at wound edges and in group C patients received surgical management of wound in form of split-thickness skin grafting.
Details of treatment methodology in each group are as follows:
Group A: Debridement and Dressing:
After debridement, patients under this group were managed with the regular sterile dressing of the wound. The wound and surrounding skin were cleaned with a povidone-iodine solution followed by normal saline. After dry mopping, the area, a thin layer of povidone-iodine ointment was applied over the wound and covered with sterile gauze pieces. Specialized dressing materials were not used in this study. The frequency of dressing change varied, depending on the requirement of individual wounds. Most wounds required a more frequent dressing change in the initial period of 1-2 days, which would later be sufficed with alternate day dressing changed regime.
Group B: Platelet-Rich Plasma infiltration:
Autologous Platelet-Rich Plasma (PRP) was prepared in the Centre for Autologous Platelet Biotechnological Intervention (CAP_BI) at the Department of Orthopaedics, AVBRH. The preparation of PRP was done as per the protocol developed by the centre, STARS therapy. [8] 20ml of venous blood was collected from the antecubital vein of the patient and divided equally into 4 Ethylene-diamine-tetra-acetic acids (EDTA) bulbs. These samples were centrifuged by the standard double spin method. The first spin of 10 minutes at 1200 rpm would separate the RBCs at a bottom layer and plasma at the top layer. This plasma was extracted into separate bulbs and a second spin for 10 minutes at 2000 rpm was performed. This separates plasma into the upper buffy coat containing Platelet-Poor Plasma (PPP) and the lower Platelet-Rich Plasma (PRP) layer. This lower layer (normally 2-4 ml) was collected in 2 ml syringes. This whole preparation was done at a room temperature of 22–24°C. Haemoglobin level of 10gm% and above was kept as a requirement for PRP treatment (Figure 1).
Meanwhile, the patient was taken on the table, in the sterile minor procedure room. The wound and surrounding area were cleaned with cetrimide-chlorhexidine (Savlon) solution and normal saline and draping were done using an eye towel. The prepared platelet-rich plasma (PRP) was infiltrated in the wound edges in a pattern similar to giving local anaesthesia, using a 24G gauge needle, followed by the sterile dressing of the wound. This process was repeated every 4th day, till satisfactory wound healing was achieved.
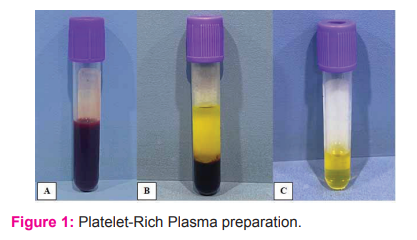
A: Blood collected in EDTA bulb, B: After 1st spin of 10 minutes at 1200 RPM. Upper buffy layer and lower layer of settled RBCs and C: Buffy layer transferred to another bulb and undergone 2nd spin of 10 minutes at 2000 RPM
Group C: Split thickness skin grafting:
Patients in this group were initially managed with regular sterile dressings, similar to Group A, till a healthy granulation tissue bed was formed at the recipient site. The patients were then taken up for surgery after fulfilling the pre-operative requirements and obtaining the necessary consent.
Pre-operative check-list:
-
Haemoglobin >= 10gm%
-
Control of other co-morbidities like systemic hypertension
-
Donor site – Should be free of infections, wounds
-
Recipient site – Healthy granulation bed, no exposed bones, tendons, ligaments
- No signs of infection
- Skin margins healthy
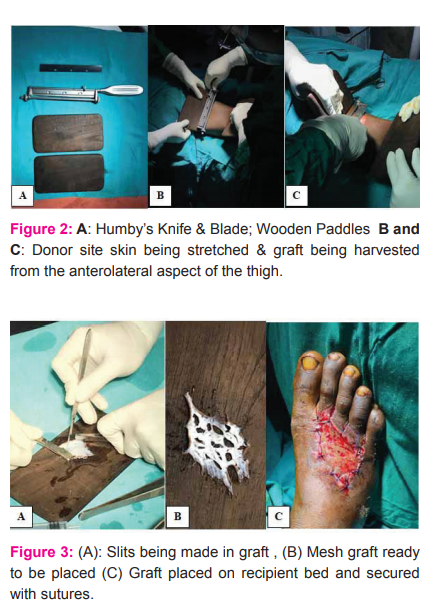
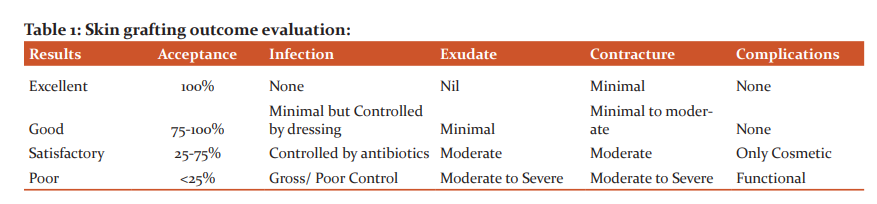
The site used for harvesting graft was the anterolateral aspect of the thigh. The split-thickness skin graft was harvested using a Humby’s knife. Multiple slits were made in the graft using a knife to give it a ‘mesh-like’ appearance. Skin grafting was done as per the standard method. The grafted area was covered with saline-soaked gauze and an adequately tight dressing with sufficient padding was done (Figure 2A, B and C) and Figure 3A, B and C).
Evaluation of wound healing
For group A and group B patients, the wound assessment was done using “Bates Jensen Wound Assessment Tool (BJWAT)”.9, 10 This tool assesses the wound based on 13 points, namely: size, depth, exudation, necrosis, skin discolouration, granulation tissue, epithelium formation, etc. The wounds are scored between 13 and 65, where a decrease in the score means healing. A score of 13 indicates the complete healing of the wound. The wounds in these two groups (A & B) were evaluated using BJWAT on enrolment (Week 0) and then on 1st, 3rd, 5th, 7th, and 9th week of the intervention (Table1).
Group C patients were evaluated initially (Week 0) using BJWAT. After skin grafting the wounds were assessed clinically for graft acceptance, signs of infection, exudation, graft contracture, or any other complications. The below-mentioned table was created for this purpose. The evaluation was done on enrolment (Week 0), on the 5th day (Week 1), followed by 3rd, 5th, 7th, and 9th-week post-graft.
Evaluation of Functional and Cosmetic Outcome
Functional outcome evaluation was done using the QuickDASH score 11 for hand injuries and Foot and Ankle Ability Measure (FAAM) score12 for foot injuries, at 3 and 6 months. Both these scales are well recognized and accepted internationally with a high-reliability index for evaluation of functional outcomes in traumatic injuries of hand and foot, respectively. The scales consist of a subjective questionnaire with graded responses. Patients have to select the most appropriate response as per their recent past experiences of day to day activities.
All statistical analysis was done by Statistical Package for Social Sciences (SPSS) version 26.
Results
-
In the present study, the mean age in dressing group (A), PRP group (B), and skin grafting group (C) was 33.4 ±15.26, 29.8 ±17.07, and 34.5 ±16.33 years respectively. There was no significant difference in age distribution in all three groups. (p>0.05) Out of a total of 30 patients, 26 were male while 04 were female, making the male: female ratio 6.5:1.
-
The majority of the patients in this study were students: 10 (33.33%) followed by employees in industrial setups: 8 (26.3%) and farmers: 8 (26.3%).
-
On evaluating the mode of injury amongst patients, road traffic accidents were found to be the major mode of trauma, with 12 patients (40%), followed by industrial accidents in 8 patients (26.6%) and farming accidents in 8 patients (26.6%).
-
As per side involvement, predominantly the injuries were on the right hand or right foot: 19 (63.3%)
-
In associated local injuries, a majority of the cases had fractures of metatarsals, metacarpals, or phalanx: 22 (73.3%). Associated injuries elsewhere in the body included fractures of radius-ulna in 10 (33.3%) patients, followed by fractures of tibia-fibula in 7 (23.3%) patients.
-
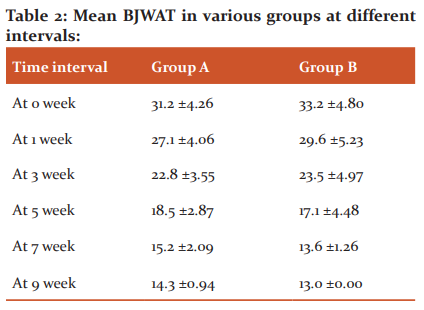
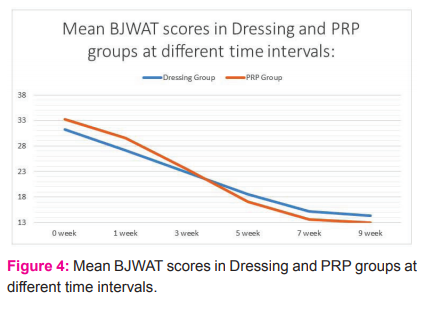
Wound size pre-treatment, in the majority of the wounds, was in the range of 6-10 cm2. The pre-treatment mean BJWAT scores were 31.2 ±4.26, 33.2 ±4.80, and 32.2 ±4.52, in dressing group, PRP group, and skin grafting group, respectively.
-
The mean BJWAT score in dressing group (A) pre-treatment was 31.2 ±4.26 and at 9-week post-treatment was 13.3 ±0.94. There was a statically significant reduction in BJWAT score pre-treatment to 9 weeks post-treatment. (p<0.05) Similarly, the mean BJWAT score in the PRP group (B) pre-treatment was 33.2 ±4.80 and at 9 weeks post-treatment was 13.0 ±0.00. This reduction was also statistically significant. (p<0.05)
-
The observed mean BJWAT scores in the dressing group and PRP group at various time intervals are as follows ( Table 2 and Figure 4):
In skin grafting group (C), 80% of patients achieved ‘excellent’ outcomes, followed by 10% ‘good’ and 10% ‘satisfactory’ by 9 weeks.
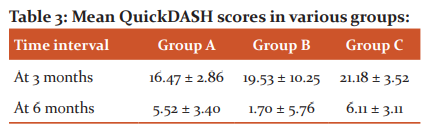
Functional outcome of hand injuries was evaluated by QuickDASH scores, and the scores for the three groups were as follows Table 3:
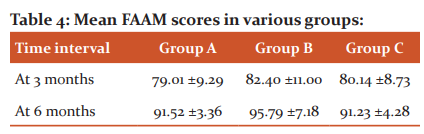
Foot injuries were evaluated for the functional outcome by Foot and Ankle Ability Measure (FAAM) scores and the results for the three groups are as follows ( table 4):
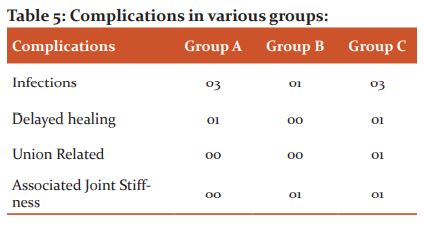
The following complications were observed in the study (Table 5):
Discussion
Demographics
In the present study, on comparing the mean age in the three groups, there was no significant difference in age distribution. (p>0.05) Also, there was no gender difference when the three groups were compared statistically. (p>0.05) With a male: female ratio of 6.5:1, the lower number of females in this study may be attributed to the fact that males are still the predominant bread earning and outgoing members of the rural and sub-urban society, where the study is based.21 This causes males more exposure to road traffic accidents and workplace hazards related to industrial and agricultural types of machinery. El-Sayed et al. 13 worked on the usefulness of platelet-rich plasma (PRP) (study) in treating foot wounds, in comparison to regular dressings (control). They noted the age range of 31 to 66 years (mean = 49±5.06 years). Soumya Ghosh et al.14 assessed wound healing in open hand injuries and found 31.13 years as the mean age with a range of 18-45 years. Predominantly, males were more affected (male: female = 2.3:1), similar to the finding of this present study.
There was no difference when the three groups were compared statistically concerning the occupation. (p>0.05) The majority of the patients in this study were students: 10 (33.33%)followed by industrial setup employees: 8 (26.6%). The fact that the majority of patients in both these groups had to travel for work or studies, combined with the poor traffic control might be a contributing factor towards more injuries due to road traffic accidents. An important part of the study group was formed by farmers: 8 (26.6%). On evaluating the mode of injury, road traffic accidents were found to be the major mode with 12 patients (40%), followed by industrial accidents in 8 patients (26.6%) and farming accidents in 8 patients (26.6%). Two third of road traffic accidents occurring in India have victims within the age range of 15-44 years. 15 This is similar to the age groups found in our study. An official report states that a total of 46044 road traffic accident cases were noted in India in the year 2018, with the highest number of road accident-related deaths in the world.16 The industrial employees’ work with heavy types of machinery, came with a work hazard of industrial accidents and injuries to hand and foot. Farmers use types of machinery like thresher machines, sharp farming tools, and knives, making them prone to traumatic injuries. There was no significant difference in the mode of injury amongst the three groups (p>0.05).
As per the side involved in the current study, predominantly the injuries were on the right hand or right foot: 19 (63.3%). Since the dominant extremity is more prone to injuries, the majority of right-sided dominance can be observed from the study. But on comparing the three treatment groups, there was no statistically significant difference observed (p>0.05).
Wound characteristics& healing
The majority of the wounds in patients, 5 (50%) in dressing group(A), 6 (60%) in PRP group (B), and 6 (60%) in skin grafting group (C), were in the size range of 6-10 cm2, indicating no significant statistical difference amongst three groups. (p>0.05)The mean BJWAT scores before treatment in dressing group (A), PRP group (B), and Skin grafting group (C) were 31.2 ±4.26, 33.2 ±4.80, and 32.2 ±4.52respectively. There was no significant difference in BJWAT scores on the distribution of patients in all three groups indicating similar nature of wound characters in all 3 groups (p>0.05).
The comparison of mean BJWAT score in the PRP group (B) and dressing group (A) at different intervals shows no significant difference in the two groups till 5 weeks. (p>0.05) But after 5 weeks, wounds in Group B heal quickly as compared to Group A with statistical significance up till 9 weeks. (p<0.05)By the BJWAT scale, a score of 13 is the minimum and this value indicates complete healing of the wound. By the 7th week of treatment 9 (90%) patients in the PRP group (B) had healed, while the dressing group patients required up to 9 weeks or more to heal completely. This fact adds to the evidence in support of PRP’s role in accelerated wound healing. El-Sayed et al.13 found the duration for the healing of wounds to be 12 wks in 82.5% of the dressing (control) group and 97.5% of the PRP (study) group. Use of PRP proved to be efficacious with fewer complications like wounds getting infected, exudation, pain, and failed or delayed healing.
Martinez-Zapata et al.17 found similar results of higher total healing in PRP cases in comparison to the control group. Carter et al.18 performed a meta-analysis on wound care and concluded that PRP leads to more number of complete healing than other treatment modalities. Villella et al. 19 also documented the same. Thimmanahalli et al.20 studied the efficacy of platelet-rich plasma use in augmentation of skin grafting in comparison to other popularly used techniques like suturing, glueing or use of staples. They found that the use of PRP showed a swift and superior healing rate, with prompt graft take. Complications like haematoma formation, oedema of graft, exudation, need for frequent change of dressings, and hospital stay was evidently to a smaller extent with PRP. No side effects were observed with the study group. Such combinations of treatment protocols were not used in the present study.21
The outcome in the skin grafting group was evaluated as per table 1. The excellent outcome in the skin grafting group (C) at 1 week after treatment was 0% and at 9 weeks was 80%. This shows the statistically significant difference in group C. (p<0.05)The final results in Group C shows, out of total 10 patients, 80% were with excellent outcome, followed by the good outcome in 10% patients. This indicates that 80% of grafts were properly taken up by 9 weeks and did not have any complications such as contractures, infections, or dehiscence.
Complications
Infection was the most common complication affecting 3 (30%) in the dressing group, 1 (10%) in the PRP group, and 3 (30%) patients in the skin grafting group. PRP treatment has been documented to reduced local wound infection caused by Staphylococcus aureus, Group A streptococcus, and Neisseria gonorrhoeae. 21 Similar observations are seen in the present study. Other complications noted were delayed healing, delayed or mal-union, and associated joint stiffness.
Functional Outcome
In Hand: The comparison of mean QuickDASH scores in dressing group, PRP group, and skin grafting group at 3 months after treatment shows no statistically significant difference. (p>0.05) While, the comparison of mean QuickDASH scores at 6 months, shows PRP group (B) (1.70 ±5.76) had better functional outcome compared to dressing group (A)(5.52 ±3.40) and skin grafting group (C) (6.11 ±3.11) at 6 months with statistically significant difference (P<0.05). The best functional results were obtained in the PRP group, followed by the dressing group. The skin grafted wounds on the hand showed maximum compromise in terms of the function of the hand.
In Foot: Similar results were obtained in foot wounds also, as determined by mean FAAM value. The comparison of mean FAAM scores in dressing group, PRP group, and skin grafting group at 3 months after treatment shows no statistically significant difference. (p<0.05) At 6 months, the best result was obtained in the PRP group (B) (95.79 ±7.18), followed by similar results in dressing group (A) (91.52 ±3.36) and skin grafting group (C) (91.23 ±4.28).(p<0.05) This is probably because activities expected in the foot as per the FAAM criteria require relatively less mobility and fine actions of the foot as against hand functions.
Conclusions
This study supports that platelet-rich plasma infiltration at wound edges is noted to be the best modality for wound management in hand and foot, from the point of rate of healing, control of infection, and function of the part involved. Ease of procedure and relatively acceptable results places debridement followed by serial sterile dressing at second for management of traumatic hand and foot wounds. The skin grafting group is noted to have similar results as the dressing group in terms of control of infection and function of the part. Enhanced rate of healing with fewer complication rates, as offered by platelet-rich plasma treatment, leads to the reduced hospital stay and overall cost of treatment for patients. This modality can also be proceeded with on an out-patient basis. Long term functional outcome is also found to be superior to other modalities. Hence it can be concluded that platelet-rich plasma provides a safe and effective treatment option for traumatic wounds of hand and foot.
Conflict of Interest: None
Funding: nil
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors, editors, and publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
IEC Approval Letter Number: DMIMS(DU)/IEC/2018-19/7396
References:
-
Hollander JE, Singer AJ. Laceration management. Ann Emerg Med. 1999 Sep 1;34(3):356-367.
-
Singer AJ, Hollander JE, Quinn JV. Evaluation and management of traumatic lacerations. N Engl J Med 1997 Oct;337(16):1142-1148.
-
Park K. Park's textbook of preventive and social medicine. Bhanot Publishers, 2015. 23rd edition.
-
World Health Organization. Global status report on road safety 2015. WHO; 2015 Dec 17.
-
Singh J, Gupta G, Garg R, Gupta A. Evaluation of trauma and prediction of outcome using TRISS method. J Emerg Trauma Shock 2011 Oct;4(4):446.
-
Notley DA, Martin DR, Hill M. Evaluation and management of traumatic wounds. Relias Media. 2015 March 1. Available at https://www.reliasmedia.com/articles/134664-evaluation-and-management-of-traumatic-wounds
-
Werner SL, Plancher KD. Biomechanics of wrist injuries in sports. Clin Sports Med 1998 Jul;17(3):407-20.
-
Shrivastava S, Mahakalkar C, Tayde S, Mehmood M, Gupta A. Developing ideal solution for acute wound treatment by regenerative medicine. J Regen Med 2016;5:2: 21-24.
-
Bolton L, McNees P, van Rijswijk L, de Leon J, Lyder C, Kobza L, et al. Wound outcomes study group, Wound-healing outcomes using standardized assessment and care in clinical practice. J Wound Ostomy Continence 2004;31(2):65-71.
-
Harris C, Bates-Jensen B, Parslow N. Development of a pictorial guide for training nurses. Wound Care Canada 2009;7(2):34.
-
Wong JY, Fung BK, Chu MM, Chan RK. The use of Disabilities of the Arm, Shoulder, and Hand Questionnaire in rehabilitation after acute traumatic hand injuries. J Hand Ther 2007;20(1):49-56.
-
Goldstein CL, Schemitsch E, Bhandari M, Mathew G, Petrisor BA. Comparison of different outcome instruments following foot and ankle trauma. Int J Foot Ankle 2010 Dec;31(12):1075-80.
-
Abd El-Mabood ES, Ali HE. Platelet-rich plasma versus conventional dressing: does this really affect diabetic foot wound-healing outcomes? Egypt J Surg 2018;37(1):16.
-
Ghosh S, Sinha RK, Datta S, Chaudhuri A, Dey C, Singh A. A study of hand injury and emergency management in a developing country. Int J Crit Illn Inj 2013 Oct;3(4):229.
-
Sharma N, Kumar AA. Road accidents in India: Dimensions and issues. [Accessed on 2018 Dec 14]. Available from: http://www.teriin.org/library/files/Road_Accidents_in_India.pdf
-
Road accidents in India. [online] [Accessed on 2020 Oct 10]. Available from: https://morth.nic.in/sites/default/files/Road_Accidednt.pdf
-
Martinez-Zapata MJ, Martí-Carvajal AJ, Solà I, Expósito JA, Bolíbar I, Rodríguez L. Autologous platelet-rich plasma for treating chronic wounds. Cochrane Database Syst Rev 2012; 10:89–92.
-
De Leon MJ, Driver VR, Fylling CP, Carter MJ, Anderson C, Wilson J, et al. The clinical relevance of treating chronic wounds with an enhanced near-physiological concentration of PRP gel. Adv Skin Wound Care 2011; 24:357–368.
-
Villela V, Falanga A, Brem H, Ennis W, Wolcott R, Gould L, Ayello E. Role of PRP and maintenance debridement in the treatment of difficult-to-heal Chronic wounds. Ostomy Wound Manage 2010; 6(3):2–13.
-
Thimmanahalli GU, Kumar M. Efficacy of autologous platelet-rich plasma over conventional mechanical fixation methods in split-thickness skin grafting. Int Surg J 2018 Dec 27;6(1):108-13.
-
Li H, Hamza T, Tidwell JE, Clovis N, Li B. Unique antimicrobial effects of platelet?rich plasma and its efficacy as a prophylaxis to prevent implant?associated spinal infection. Adv Healthc Mater 2013;2(9):1277-84.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





