IJCRR - 13(2), January, 2021
Pages: 85-89
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
The Study of Anti-inflammatory and Analgesic Effects of Oral Serratiopeptidasein Postoperative Patients in a Tertiary Care Hospital
Author: C. Khanwelkar, Kartik Peethambaran, S. A. Jadhav
Category: Healthcare
Abstract:Introduction: Oral proteolytic enzymes like serratiopeptidase are very commonly used by clinicians either alone or in combination with non-steroidal anti-inflammatory drugs for analgesia and anti-inflammatory and wound healing purpose in postoperative patients. Objective: To study the effect of serratiopeptidase and diclofenac in postoperative patients. Methods: Three groups (n= 20) of postoperative patients having clean surgical wound were treated with diclofenac 50 mg twice a day (BID) and serratiopeptidase 10mg three times a day (TID) + Diclofenac 50 mg BID for one week. The third group was not given any analgesic- anti-inflammatory drug. The pain and inflammation at the site of the wound were assessed by VAS and Asepsis score on 1st and 7th day. Results: No difference in analgesic and anti-inflammatory effects were found in both treatment groups (p> 0.05). Patients in the no-treatment group had relief of inflammation comparable to both treatment groups. Patients from no treatment group did not require analgesic for pain relief. Conclusion: Addition of serratiopeptidase did not potentiate the analgesic and anti-inflammatory effects of diclofenac. In clean surgical wounds, use of analgesic anti-inflammatory drugs should be as per need and not on regular basis.
Keywords: Serratiopeptidase, Diclofenac, Analgesic, Anti-inflammatory, Postoperative, Surgical wound.
Full Text:
Introduction
Oral preparations of proteolytic enzyme serratiopeptidase are routinely marketed in India, either isolated or as a fixed-dose combination with non-steroidal anti-inflammatory drugs (NSAID) like aceclofenac, diclofenac. They are widely prescribed by physicians and surgeons for producing analgesia and anti-inflammatory effect and to reduce oedema associated with trauma, surgery, dental procedures, respiratory tract infection, parotitis, arthritis, etc.1,2
Serratiopeptidase is a proteolytic enzyme obtained from non-pathogenic bacteria Serratia E-15 species belonging to Enterobacteriaceae family. It is produced in the intestine of silkworm which causes a breakdown of cocoon walls. It has a very large molecular weight, 45000-60000 daltons.3,4 Naturally large molecular weight proteins, when given orally, are degraded by proteolytic enzymes in the gastrointestinal tract and not absorbed intact. Therefore, it is doubtful that serratiopeptidase retains its structure after absorption and enters the plasma intact. There are very few studies suggesting oral bio-availability of serratiopeptidase.5 Only one study has shown the presence of this enzyme in high concentration in the abscess, in carrageenin induced paw oedema in rodents.6 Thus though the pharmacokinetic data of serratiopeptidase is still unproven but many studies have suggested its very good analgesic and anti-inflammatory role in dental surgeries.7,8 Serratiopeptidase like other oral enzymes were shown to have a good effect in osteoarthritis.9
Serratiopeptidase is not yet listed in any official drug compendium, pharmacopoeia.10 Therefore, it was worthwhile to study the analgesic and anti-inflammatory effect on the surgical wound in postoperative patients in surgery wards in a tertiary care hospital.
Material and Methods
The study was conducted in the general surgery ward of Krishna Hospital, Karad, Maharashtra. Approval of protocol and permission of Ethics Committee of Krishna Institute of Medical Sciences, Karad, was taken before starting the study (Ref. No. KIMSDU/IEC/09/20188). Total 60 adult postoperative patients of either sex, having clean surgical wound were enrolled after they gave volunteer informed consent. All patients were given all information of study protocol when surgery was planned and consent was taken before the surgery.
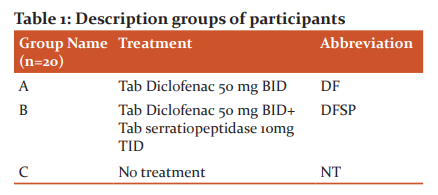
Patients who had emergency surgery, complication during surgery, malignancies, uncontrolled diabetes mellitus or any serious co-morbidity were not included in the study. Pregnant, lactating women were also excluded. Patients already receiving corticosteroids, NSAIDs or any oral enzyme preparation were excluded from the study. The patients were assigned randomly to either of the three study groups on their first postoperative day (Table 1). Each group had 20 participants. Following the treatment, the schedule was given to the respective group for 7 days.
Statistical Methods
The recorded data was processed and analyzed utilizing the Social Sciences Statistical Package (SPSS) for ANOVA and students paired ‘t’ tests. The expectation threshold of the analysis was held at 95 per cent, which suggested that the "p" will be less than 0.05 level of significance. A 10 point Visual Analog Scale (VAS) for the pain analysis was used to evaluate the intensity of pain10. A wound assessment method, ASEPSIS, was used that enhances the outcomes including reproducibility of the wound's sepsis evaluation by assigning points especially within the 1st week of wound development as well as clinical implications of infections.
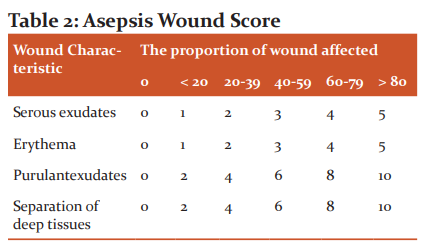
In Group C no treatment with any analgesic or anti-inflammatory drug was given for 7 postoperative days, but if the patient needs rescue NSAID treatment was decided to be given. The severity of pain was assessed by asking the patient to mark the level of pain on the visual analogue scale (VAS), for 1st and 7th postoperative day11. The inflammation and status of healing of surgical wound were assessed by measuring, Asepsis Wound Score as given in Table 2 12.
Asepsis score was calculated for each patient on 1st and 7th postoperative days. Mean of asepsis scores of each group was calculated for day 1 and 7. The difference between asepsis scores on 1st and 7th day was taken as a measure of wound healing and reduction in inflammation. The mean values of VAS score and Asepsis score of each group on day 1 and day 7 were compared by applying student’s paired ‘t’ test, and significance was calculated. The differences in VAS score and differences in Asepsis scores of all three groups were compared by applying ANOVA. Comparison of reduction in pain and reduction in inflammation between Group A & B, Group A & C and Group B & C was done by using student’s paired ‘t’ test.
Results
The two scales VAS and Asepsis used for the scoring of pain and sepsis of wound were statistically analyzed. The mean visual analogue scale (VAS) was correlated according to age in Groups. The mean VAS score was decreased very highly significantly (p<0.0001), on 7th postoperative day as compared to 1st day, in all three groups A, B and C (Table 3).
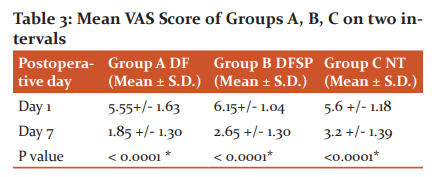
P-value as per student’s paired ‘t’ test. * indicates very highly significant
Mean Asepsis Score was decreased very highly significantly (p< 0.0001) on 7th postoperative day as compared to that on 1st postoperative day in all three groups A, B and C. (Table 4)

The mean of reduction in VAS and Asepsis score between 1st and 7th day was calculated for each group. These means of three groups were compared by applying ANOVA. There was no significant difference in a mean reduction in the asepsis score of all three groups (p= 0.06). There was a statistically significant difference in a mean reduction of VAS score when three groups were compared by ANOVA (p< 0.005) as shown in Table 5.
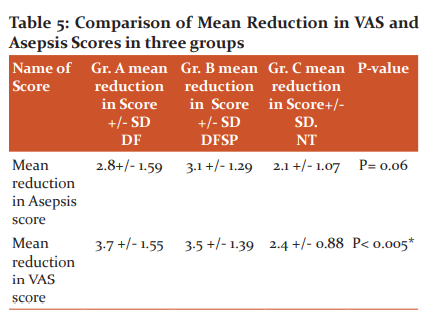
P-value by ANOVA.* indicates highly significant.
Reduction in VAS and Asepsis scores was compared between individual groups in pairs by applying student’s paired ‘t’ test. The reduction in both VAS and Asepsis scores in group A (Diclofenac) and group B (diclofenac + serratiopeptidase) was not statistically different (p> 0.05). The reduction in asepsis score of group A, as well as that of B, was not statistically different from that of group C (No treatment group) and p> 0.05. The reduction in pain indicated by the reduction in VAS score was statistically significantly higher in group A(Diclofenac) and group B (Diclofenac+ Serratiopeptidase) as compared to that in group C (No treatment group).
Discussion
The present study was aimed to evaluate the efficacy of serratiopeptidase and diclofenac in reducing pain and inflammation at the surgical wound site in postoperative patients. Total of 60 patients was distributed in three groups: A, B, C (n= 20). Group A patients received oral diclofenac 50 mg BID, group B patients received oral diclofenac 50 mg BID and oral serratiopeptidase 10 mg TID. In both these groups, treatment with respective drug was started on the first postoperative day and was continued till 7th postoperative day. The group C was not given any analgesic or anti-inflammatory treatment unless needed. No patient in this group required rescue analgesia or anti-inflammatory drug, though diclofenac 50 mg BID was kept as a rescue if the patient complains of intolerable pain.
Our results indicate that there was no added analgesic or effect produced by serratiopeptidase when it was combined with diclofenac. Isolated diclofenac treatment produced equivalent analgesic activity as that produced by diclofenac and serratiopeptidase combined treatment (p> 0.05). No patient in the no-treatment group (Group C) demanded analgesia during 7 postoperative days, that shows pain in clean surgical wounds is tolerable most times. In our study, it was very much obvious that in both the treatment groups, the reduction in VAS score was significantly more than the no-treatment group. Therefore, we suggest that analgesic should be given in postoperative patients having clean surgical wound as per need and if the pain is intolerable for the patients and not regularly.
The reduction in asepsis score was comparable in all three groups and there was no significant statistical difference, p>0.05 (Table 6). In no-treatment group i.e. group C, also reduction of asepsis score was similar to treatment groups, i.e. groups B and C. These results suggest that addition of serratiopeptidase has not enhanced the anti-inflammatory effect of diclofenac. It is also suggested that in clean surgical wounds neither diclofenac nor serratiopeptidase can enhance wound healing, and anti-inflammatory drugs should be given if there is excessive inflammation at the wound site.
Many studies, particularly involving dental procedures, have suggested that serratiopeptidase reduces inflammation, pain and trismus following dental procedures2,7,13,14. Many studies, particularly involving dental procedures, have suggested that serratiopeptidase reduces inflammation, pain and trismus following dental procedures. In a study including postoperative orthopaedic patients anti-inflammatory, analgesic and wound healing effects of trypsin–chymotrypsin combination was found to be significantly higher than serratiopeptidase.15 Serratiopeptidase have shown significant anti-inflammatory effect and mild analgesic effect of in patients with upper and lower limb trauma.16 Our results are not in agreement with the results of these studies.
In the study of Rath et al.17, they have shown improvement in wound healing by topical application of serratiopeptidase – metronidazole in full-thickness wounds in rabbits. Thus serratiopeptidase may be beneficial by topical application. In a case report, serratiopeptidase was reported to increase the spread of infection after dental surgery.18 In a study in hysterectomy, caesarian section and episiotomy wounds, much-delayed healing was seen in patients treated with serratiopeptidase 10 mg TID. In this study, patients treated with the only serratiopeptidase required more NSAIDs for getting pain relief.19 In a study in rabbits it was concluded that serratiopeptidase could not improve and rather caused the delay in oral wound healing.20
There is a lack of pharmacokinetic data about oral administration of serratiopeptidase. Only a few studies show the presence of serratiopeptidase in serum after oral administration in human and animals.2,5 One questionnaire-based study has shown that the use of serratiopeptidase and other oral proteolytic enzymes with or without NSAIDs is influenced by marketing skills of medical representatives and pharmaceutical companies. The same study has shown that the cost of treatment using a combination of serratiopeptidase and NSAID is approximately 5 times more than compared to isolated NSAID treatment.21
Thus looking towards these facts and results of our and many other clinical studies, we suggest that use of oral proteolytic enzymes for analgesic, anti-inflammatory and wound healing purpose in clinical practice should be avoided until it is included by official drug compendia. Use and availability of such drugs having unproven efficacy should be regulated by strict actions by the drug controlling authorities.
Conclusion
The results suggested that the addition of serratiopeptidase has not enhanced the anti-inflammatory effect of diclofenac. It is also suggested that in clean surgical wounds neither diclofenac nor serratiopeptidase can enhance wound healing, and anti-inflammatory drugs should be given if there is excessive inflammation at the wound site. Addition of serratiopeptidase did not potentiate analgesic and anti-inflammatory effect of diclofenac. In clean surgical wounds, use of analgesic anti-inflammatory drugs should be as per need and not regularly.
Funding source: Krishna Institute of Medical Sciences “Deemed To Be “University, Karad, Maharashtra.
Conflict of Interest: None
Acknowledgement: We are grateful for the support to the Department of Pharmacology, Krishna Institute of Medical Sciences, Karad-415339, Maharashtra, India.
References:
-
Moslemi N, Khorsand A, Torabi S, Shahnaz A, Shayesteh YS, Fekrazad R. Periosteal releasing incision with diode laser in guided bone regeneration procedure: a case series. J Lasers Med Sci 2016;7(4):259.
-
Tiwari M. The role of serratiopeptidase in the resolution of inflammation. Asian J Pharma Sci 2017;12(3):209-215.
-
Nakahama K, Yoshimura K, Marumoto R, Kikuchi M, Lee IS, Hase T, et al. Cloning and sequencing of Serratia protease gene. Nucleic Acids Res 1986;14(14):5843-5855.
-
Nirale NM, Menon MD. Topical formulations of serratiopeptidase: development and pharmacodynamic evaluation. Ind J Pharm Sci 2010;72(1):65.
-
Dallas P, Rekkas D, Choulis NH. HPLC determination of serratiopeptidase in biological fluids. Pharmazie 1989;44(4):297.
-
Moriya N, Nakata M, Nakamura M, Takaoka M, Iwasa S, Kato K, et al. Intestinal absorption of serrapeptase (TSP) in rats. Biotech Appl Biochem 1994;20(1):101-108.
-
Mouneshkumar CD, Suresh KV, Patil MR, Desai R, Tauro DP, Shiva Bharani KN, et al. Comparison of clinical efficacy of methylprednisolone and serratiopeptidase for reduction of postoperative sequelae after lower third molar surgery. J Clin Expt Dentistry 2015 Apr;7(2):e197.
-
Santhoshkumar M. The emerging role of serratiopeptidase in oral surgery: literature update. Asian J Pharm Sci 2018;11(3):19-23.
-
Klein G, Kullich W. Short-term treatment of painful osteoarthritis of the knee with oral enzymes. Clin Drug Invest 2000;19(1):15-23.
-
Mathew JR, Sivasubramanian K. Letter to Editor-Use of oral enzyme preparations: Is there any evidence? Ind J Plastic Surg 2004;37(1):80.
-
Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain 1997;72(1-2):95-97.
-
Harish Patel BN, Kumar P, Kailas CT, Chandrasekhar RL. A study on wound asepsis score for skin closure in surgical procedures. Int J Surg 2019;3(1):61-64.
-
Sivaramakrishnan G, Sridharan K. Role of Serratiopeptidase After Surgical Removal of Impacted Molar: A Systematic Review and Meta-analysis. J Maxillofac Oral Surg 2018;17(2):122-128.
-
Basheer SA, Mohan GM, Vijayan S. Efficacy of medication on postoperative pain, swelling & Trismus after impaction of Mandibular third molar. Int J App Dental Sci 2017;3(3):96-99.
-
Chandanwale A, Langade D, Sonawane D, Gavai P. A randomized, clinical trial to evaluate efficacy and tolerability of trypsin: chymotrypsin as compared to serratiopeptidase and trypsin: bromelain: rutoside in wound management. Adv Therap 2017;34(1):180-198.
-
Garg R, Aslam S, Garg A, Walia R. A prospective comparative study of serratiopeptidase and aceclofenac in upper and lower limb soft tissue trauma cases. Int J Pharmacol Pharm Technol 2012;1(2):11-16.
-
Rath G, Johal ES, Goyal AK. Development of serratiopeptidase and metronidazole based alginate microspheres for wound healing. Artif Cells Blood Substit Immobil Biotechnol 2011;39(1):44-50.
-
Rajaram P, Bhattacharjee A, Ticku S. Serratiopeptidase–A cause for spread of infection. J Clin Diag Res 2016;10(8):ZD31.
-
Koltsakidou Α, Katsiloulis C, Εvgenidou Ε, Lambropoulou DA. Photolysis and photocatalysis of the non-steroidal anti-inflammatory drug Nimesulide under simulated solar irradiation: Kinetic studies, transformation products and toxicity assessment. Sci Total Env 2019;689:245-257.
-
Garg S, Garg A, Shukla A, Dev SK, Kumar M. A review on Nano-therapeutic drug delivery carriers for effective wound treatment strategies. Asi J Pharm Pharmac 2018;4(2):90-101.
-
Shah SA, Nerurkar RP. Evaluation of prescribing trends and rationality of the use of oral proteolytic enzymes. Ind J Pharm 2013;45(3):309.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





