IJCRR - 13(2), January, 2021
Pages: 33-38
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
Effectiveness of Toys in Relieving Acute Stress Measured by Heart Rate Variability in Young Adults
Author: Husrav Sadri, Shailaja S. Moodithaya
Category: Healthcare
Abstract:Introduction: The responses of the human body to stress are well documented. Usage of toys like slime and fidget-spinners has been a recent trend among the public to mitigate the harmful effects of stress on health. Objective: This study aims to evaluate the effectiveness of slime and fidget-spinners in relieving acute stress in young adults. Methods: Thirty healthy subjects were studied. Each subject underwent phases of rest, acute stress using mental arithmetic, and stress with simultaneous usage of either slime or fidget-spinner toys. The power spectrum of short term heart rate variability (HRV) was analysed in all three phases. The values obtained were compared using the Wilcoxon signed-rank test. A p-value< 0.05 is considered statistically significant. Results: Average heart rate, total power, low-frequency power (LF), high-frequency power (HF) and the LF/HF ratio were significantly raised in the mental stress phase compared to the resting phase. No statistically significant differences were found when comparing these parameters of a subject in mental stress to a subject using an either toy, except a significant increase in LF (normalised units) in the fidget-spinner experiment. Conclusion: The present study noted that usage of either toy (slime or fidget-spinner) produced no significant change in HRV parameters in a stressed subject. Based on these findings, these toys may not be advocated for the relief of acute stress since they have no significant effect on their autonomic parameters in young adults. Further studies may use parameters other than HRV to assess stress levels in an individual.
Keywords: The autonomic nervous system, Mental arithmetic, Mental stress, Power spectrum, Stress relief, Sympathovagal balance
Full Text:
The National Institute of Mental Health, USA, states that stress is a response of the human body to any demand placed upon it.1 Acute stress is known to increase heart rate and blood pressure transiently, through the action of the autonomic nervous system.2,3 The effects of stress may be objectively perceived by using quantifiable surrogate markers which respond to stressors. The autonomic nervous system regulates the effect of stress on the heart through the sympathetic and parasympathetic systems, the balance of which may be measured using heart rate variability or HRV.4 HRV is the variation of instantaneous heart rate and the series of intervals between successive peaks of the R-waves on an electrocardiogram (ECG). Analysing the power spectrum gives us various parameters like total power, low-frequency power (LF), and high-frequency power (HF). The ratio of LF/HF is the indicator of the balance between the sympathetic and parasympathetic nervous systems.
Several studies have demonstrated that HRV is the best tool to quantify mental stress based on autonomic function and sympathovagal balance, denoted by the LF/HF ratio. LF/HF ratio reliably rises when the subject is under stress, and that frequency domain measures consistently supported the idea that during stress there is a general depression of HRV and displacement of sympathovagal balance towards sympathetic activation due to elevation of LF, which accounts for sympathetic and parasympathetic system activation, and depression of HF, which is associated with the parasympathetic system only.5,6
Due to greater recognition being given to the various detrimental effects of mental stress on human health, the focus is now on attempting to counteract it before health is impacted adversely. Various techniques and methods have been employed for this purpose, including yoga and aerobic exercise, music, and exposure to nature.7-9 In 1993, a lady by the name of Catherine Hettinger, who suffered from myasthenia gravis, created the prototype of the fidget-spinner as a means of bonding with her daughter. The palm-sized spinners consist of a ball bearing which sits in a three-pronged plastic device which can then be flicked and spun around. She applied for a patent, which lapsed in 2005, after which small manufacturers marketed the toy as a therapeutic tool for children with attention deficit hyperactivity disorder (ADHD), anxiety, and autism, to help them focus and relieve stress. Nearly ten years later, the publicity surrounding the toy and its purported uses grew rapidly, creating a trend of using it as a stress-relief toy among both adults as well as children.10,11
While such toys have been extensively touted to provide immediate relief from stress, the public opinion has not yet been backed up by any significant research. This study is, as such, the first of its kind as it attempts to objectively evaluate the impact of such toys on the physiological markers of acute stress. The objectives of this study were to evaluate the effectiveness of and to compare the levels by which slime and fidget-spinners relieve acute stress by assessing heart rate variability in young adults.
MATERIALS AND METHODS
Pre-experiment protocols
The study was conducted from April to June 2019 on 30 male and female healthy students between the age of 18 and 22 years. Students having any history of autonomic or cardiovascular dysfunction, or those students who were on any medication that might alter autonomic or cardiovascular function were excluded from the study. The experimental protocol was performed only after obtaining approval from the Institutional Ethics Committee (INST.EC/EC/033/2019-20). Written informed consent was obtained from all participants. All subjects were requested to refrain from strenuous physical activity for at least 24 hours before recording, and not consume any caffeinated/non-caffeinated beverages for 2 hours before recording. After taking a brief history, the participants underwent the following experimental protocol:
-
Height was measured by a wall-mounted stadiometer to the nearest 0.1 cm. The subjects were instructed to stand erect, without shoes, and with their hands by their sides. Weight was measured to the nearest 100 gm using electronic weighing machine. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
-
Resting Blood pressure was recorded using a non-invasive intermittent automated blood pressure monitoring device – Omron IA2 model.
Assessment of Heart rate variability
Heart rate variability (HRV) measurements were performed in three sessions in a quiet, temperature-controlled room (23±1°C). The three sessions included are i) baseline, ii) during mental stress task iii) during mental stress task with toy exercise. Following 15 minutes of rest, Lead II Electrocardiogram (ECG) was recorded in the sitting position for 5 minutes in each session. The arm leads were placed on the shoulders to minimize interference with HRV when the subject played with the toy in the third session.
Baseline recording
Initially, the baseline ECG of the subject was recorded for five minutes (from time t=0 minutes to t=5 minutes). The subjects were asked to sit still and not move their limbs when the ECG was being recorded. This instruction was maintained across sessions.
Mental stress test
For five minutes after baseline recording (from t=5 minutes to t=10 minutes), ECG was recorded while mental stress was being concurrently induced in the subject using mental arithmetic. The mental arithmetic protocols commonly followed are variations of the serial subtraction of seven tests which is frequently used as an assessment tool in clinical practice to evaluate the ability of an individual to concentrate.12 This was done by instructing the subject to quickly subtract the number seven serially from a random three- or four-digit number, and verbally state the next number in the series.13,14 For example, if the subject was given the number 589, he would have to give answers as 582, 575, 568, and so on. In an attempt to build up stress in the subject, the investigator constantly encouraged them to answer faster, and randomly changed the starting number of the series. If the subjects gave an incorrect answer, they were informed and told to correct themselves before proceeding. A break of three minutes (from t=10 minutes to t=13 minutes) was given between this session and the next in an attempt to bring the autonomic function back to baseline.
Intervention with toy
Once stress has been induced in the subject, one of two toys (either slime or a fidget-spinner) was given at random to the subject. The subject was instructed to play with the toy moving only his hands, and keeping the rest of the body as still as possible as they simultaneously performed the mental stress task described above, and the ECG continued to be recorded for five minutes (from t=13 minutes to t=18 minutes). The ECG recording was then analyzed for HRV indices.
Analysis of recordings
Heart rate was obtained by R-R interval for which Lead II ECG was recorded using a bio amplifier data acquisition module, Powerlab 26T (AD Instruments, Australia). ECG was recorded at a sampling rate of 1000Hz. Raw recordings were manually edited to eliminate ectopics and artefacts above 5% and 2% respectively. From the obtained raw ECG data, the power spectrum of HRV was analyzed using HRV module of Lab Chart V7 (AD Instruments) based on non-parametric Fast Fourier Transformation. The power spectrum was expressed as total power in absolute units, LF (0.04-0.15Hz), HF (0.15-0.4Hz), LF normalized unit (LFnu), HF normalized unit (HFnu) and LF/HF ratio. In the power spectrum, the LF reflects cardiac sympathetic activity while the HF is a surrogate of cardiovagal function and therefore the ratio of LF to HF indicates sympathovagal balance.4,6
Statistical analysis
Mean and standard deviation of the anthropometric parameters as well as baseline blood pressure was calculated. Indices of heart rate variability (HRV) among the three sessions were presented as the mean and standard error of the mean. The variables were tested for normality of distribution, and the skewed data were compared using non-parametric tests. Wilcoxon signed-rank test was used to compare the various components of HRV. All the data were analyzed using IBM SPSS Statistics (version 20). A p-value < 0.05 is considered statistically significant.
Results
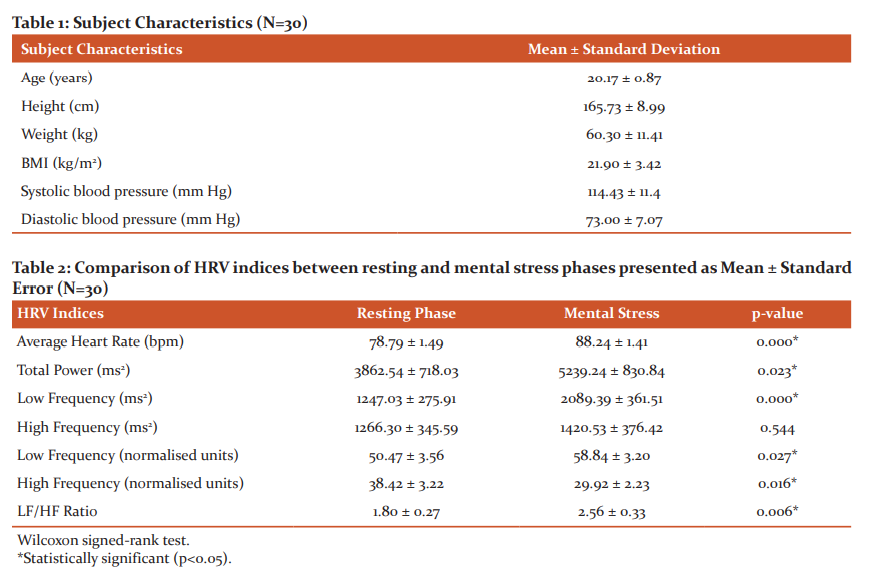
ECG data were collected for 36 subjects of whom only 30 were utilised since the software was unable to analyse the HRV indices of the other 6. The mean age of the participants was 20.17±0.87 years, with a mean body-mass index (BMI) of 21.90±3.42 kg/m2. The subjects’ basic data, including age, height, weight, BMI, and blood pressure are given as mean ± standard deviation in Table 1. The HRV indices were described in terms of mean ± standard error. Histograms were plotted and it was found that each variable did not have a normal distribution. Thus, variables were compared using a non-parametric, Wilcoxon signed-rank test. A p-value < 0.05 is considered to be statistically significant.
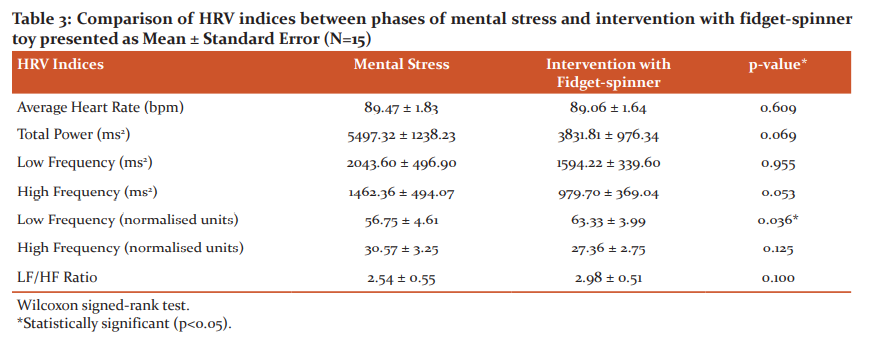
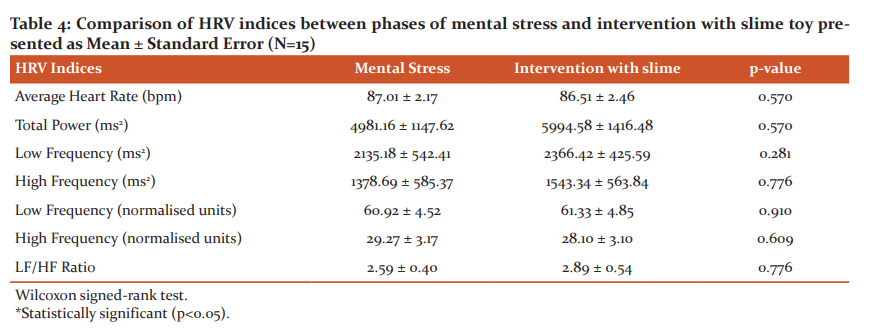
First, HRV indices of subjects in the resting and mental stress phases of the experimental protocol were compared (Table 2). As is evident from the table, differences in all the variables were found to be statistically significant, except the absolute values for high frequency. Tables 3 and 4 show the comparisons made between mental stress phase and the phase of intervention with fidget-spinner and slime toys respectively. None of the comparisons was statistically significant except the normalised low-frequency values in the fidget-spinner experiment.
Discussion
The amount of mental stress faced by an individual in today’s world is indisputably detrimental to the health of the individual. There are various ways of identifying and subsequently quantifying the amount of stress an individual may perceive including, but not limited to galvanic skin response (electrodermal activity) and skin temperature. However, the best known physiological marker of acute stress is widely known to be heart rate variability derived from an electrocardiogram since it gives information about instantaneous changes in heart rate which is used as a surrogate for autonomic function.15
While the heart rate of a subject appears to be regular clinically, there are a remarkable amount of minute variations between individual heartbeats. These variations can be found by analysing the RR-intervals recorded on an ECG, from which one may derive the heart rate variability power spectrum. The power spectrum consists of total power, low frequency (LF), high frequency (HF), each of their normalised units (LFnu and HFnu respectively) as well as the LF/HF ratio. The various parameters of the power spectrum give extensive data regarding the autonomic status of the individual using the beat-to-beat variations in heart rate as the basis for variation in autonomic function.10-12
The present study evaluated the differences between HRV power spectrum parameters between the resting phase and the phase of mental stress-induced by mental arithmetic. Predictably, the mean absolute LF and mean LFnu both increased significantly during the phase of mental stress as compared to the resting phase. This depicts that the sympathetic nervous system was activated in the phase of mental stress.12,13 The mean absolute HF showed an increase from resting phase to the phase of mental stress, but this increase was not statistically significant. Nonetheless, the mean HFnu values decreased significantly from the resting phase to the phase of mental stress, indicating that parasympathetic action was substantially dampened during the phase of mental stress. These findings are consistent with the consensus on the effect of mental stress on heart rate variability, which is to say that the stressor (in this case verbalised mental arithmetic) decreases the RR interval, pushing the frequency of RR into the LF band, increasing the LF power and simultaneously decreasing the HF power leading to an ultimate statistically significant increase in LF/HF ratio.9,14,16 Such a shift to sympathetic predominance is also seen in hypertensive patients and may be associated with increased risk of cardiac mortality as well as predict an increased risk of cardiac events.17
Attempting to intervene in the induced mental stress with a toy (either fidget-spinner or slime) has shown a relative decrease in the mean values of average heart rate, an increase in mean total power, LF, and LFnu from the phase of mental stress. In the fidget-spinner toy, a decrease was seen in mean absolute HF while the slime toy showed an increase; in both toys, absolute HF was reduced, and the mean LF/HF ratios were increased as compared to the phase of mental stress. Considering these values alone, it could be said that the toys potentiated the stress created in the subject. This is a surprising finding, considering that the toys were expected to alleviate the mental stress faced by the subject. However, none of these comparisons is statistically significant (except LFnu in the fidget-spinner experiment) and it would therefore be misguided to draw such conclusions based on this data. Furthermore, it is futile to compare the slime and fidget-spinner toys since both have shown that they do not decrease the induced stress at all but rather insignificantly increase it.14,15
Since this study appears to be the first of its kind, there is no other data to compare these findings. Based on this study, it could be inferred that slime and fidget-spinner toys have no significant effects on the physiological markers of stress. Nevertheless, it cannot be disallowed that these toys have any impact on the effects of acute stress; they may act by placebo or by mechanisms that this study has not taken into account. It is entirely possible that the sample size of this study is very small, and has thus not given significant results.16,17 Further studies with larger experimental groups are needed to verify the findings of this study. Other parameters assessing stress levels in an individual, both before and after intervention with these toys also need to be included in further studies; they may encompass a wide variety of tools ranging from stress questionnaires to salivary cortisol secretion.
Conclusions
The heart rate variability parameters of subjects responded significantly to the induction of acute mental stress by mental arithmetic, although the present study noted that an attempted intervention with either toy (slime or fidget-spinner) produced no significant change in the same parameters. It would thus seem that further studies are required to verify these findings, perhaps with larger sample sizes as well as evaluation of other mechanisms by which these toys may act, which this study has not accounted for. Firm conclusions regarding the effectiveness of these toys may only be drawn when all possible avenues of investigation have been exhaustively explored.
Acknowledgements and Funding:
This work was supported by the Indian Council of Medical Research – Short Term Studentship (grant number 2019-00774). The authors would like to thank the subjects for their wholehearted participation as well as Dr. Krishna Bhat U for aiding with the statistical analysis.
Conflict of Interest: The authors have no conflicts of interest to declare.
Contribution of Authors:
-
Husrav Sadri : Conceptualisation, data collection, data analysis, writing
-
Dr. Shailaja S. Moodithaya : data analysis, writing
References:
-
National Institute of Mental Health (US). 5 Things You Should Know About Stress. Bethesda: National Institute of Mental Health; 2019.
-
Yaribeygi H, Panahi Y, Sahraei H, Johnston TP, Sahebkar A. The impact of stress on body function: A review. EXCLI J. 2017; 16:1057–1072.
-
Brotman DJ, Golden SH, Wittstein IS. The cardiovascular toll of stress. Lancet 2007 Sep; 370(9592):1089-100.
-
Patil K, Singh M, Singh G, Anjali SN, Sharma N. Mental Stress Evaluation using Heart Rate Variability Analysis: A Review. Int J Public Ment Health Neurosci 2015 Apr; 2(1):10-16.
-
Castaldo R, Melillo P, Bracale U, Caserta M, Triassi M, Pecchia L. Acute mental stress assessment via short term HRV analysis in healthy adults: A systematic review with meta-analysis. Biomed Signal Process Control 2015 Apr; 18:370-377.
-
Malik M, Camm AJ, Bigger JT, Breithardt G, Cerutti S, Cohen RJ, et al. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur Heart J 1996; 17(3):354–81.
-
Jackson EM. Stress Relief: The Role of Exercise in Stress Management. ACSMs Health Fit J 2013 May;17(3):14-19.
-
Gäbel C, Garrido N, Koenig J, Hillecke TK, Warth M. Effects of Monochord Music on Heart Rate Variability and Self-Reports of Relaxation in Healthy Adults. Complement Med Res 2017 Feb;24(2):97-103.
-
Brown DK, Barton JL, Gladwell VF. Viewing nature scenes positively affects the recovery of autonomic function following acute mental stress. Environ Sci Technol 2013 Jun; 47(11):5562-5569.
-
Williams A. The Hour’s Hot Toy Has a Long History. The New York Times. 2017 May 14; Sect. ST:9
-
Luscombe R. As fidget spinner craze goes global, its inventor struggles to make ends meet. The Guardian. 2017 May 05.
-
Karzmark P. Validity of the serial seven procedure. Int J Geriatr Psych 2000 Aug; 15(8):677-679.
-
Deepak A, Deepak AN, Nallulwar S, Khode V. Time Domain Measures of Heart Rate Variability during Acute Mental Stress in Type 2 Diabetics: A Case-Control Study. Natl J Physiol Pharm Pharmacol 2014; 4(1):34-38.
-
Bernardi L, Wdowczyk-Szulc J, Valenti C, Castoldi S, Passino C, Spadaccini G, et al. Effects of controlled breathing, mental activity and mental stress with or without verbalization on heart rate variability. J Am Coll Cardiol 2000; 35(6):1462-1469.
-
Palanisamy K, Murugappan M, Yaacob S. Multiple physiological signal-based human stress identification using non-linear classifiers. Elektronika ir elektrotechnika 2013; 19(7):80-5.
-
Wang X, Liu B, Xie L, Yu X, Li M, Xhang J. Cerebral and neural regulation of cardiovascular activity during mental stress. Biomed Eng Online. 2016; 15 Suppl 2:160.
-
Patil SS, Gnanajyothi. A study of heart rate, blood pressure and heart rate variability at rest, in normotensive and hypertensive adult male subjects. Int J Cur Res Rev 2015 Sep; 7(18):11-14.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





