IJCRR - 13(2), January, 2021
Pages: 29-32
Date of Publication: 16-Jan-2021
Print Article
Download XML Download PDF
Relationship between Thyroid Disorder and Abnormal Menstrual Bleeding
Author: Anjana Chaudhary, Baljeet Kaur Bhatia
Category: Healthcare
Abstract:Introduction: Menstrual disorders pose a huge burden on gynaecology OPD, accounting for approximately 20 % of attendance of OPD. Thyroid disorders are prevalent globally, and thyroid conditions are 10 times more prevalent in women than in men. Thyroid dysfunction can prompt menstrual problems and infertility. Thyroid autoimmunity is associated with different forms of thyroid dysfunction. Objective: To assess the relationship between thyroid disorder and abnormal menstrual bleeding. Methods: Study was conducted in 100 women (age 15-45 years) suffering with menstrual disorders. Women with complaints other than menstrual disorders were in the control category. Following demographic characteristics, general physical examination and pelvic examination were performed with special reference to thyroid dysfunction. Patients were subjected to routine investigations (to rule out coagulation defects) such as Hb, BT, CT and platelets. All patients were subjected to Electro Chemiluminescence assay for T3, T4 and TSH estimation in their serum. Results: Off all the kinds of menstrual irregularities, woman with amenorrhea, menorrhagia, oligomenorrhea, polymenorrhea and metrorrhagia were recorded. 55% of the cases in the study group were euthyroid while 45% of the cases were diagnosed with having thyroid disorder. In study group out of 45 cases having thyroid disorder of which 18 (18%) were overt hypothyroid and 11 (11%) were subclinical hypothyroid. Overt Hyperthyroid were 11 (11%) and subclinical hyperthyroid were 5% in the study group. Of the total 3 amenorrhea cases 2 (2%) were euthyroid while 1 case was hypothyroid. Out of 52 menorrhagia cases, 28 were euthyroid, 14(14%) were hypothyroid and 10 (10%) were hyperthyroid. 19 were oligomenorrhea cases of which 7 (7%) each were euthyroid and hypothyroidism while one case was hyperthyroid. Conclusion: Strong correlation of thyroid dysfunction with menstrual disorders has been observed. Morbidity due to thyroid dysfunction in women can be reduced if diagnosed timely and treated accordingly and unnecessary hormonal treatment and surgery can be avoided.
Keywords: Pelvic, Menstrual irregularities, Oligomenorrhea, Polymenorrhea, Metrorrhagia
Full Text:
INTRODUCTION
Menstruation is a natural phenomenon regarding the discharge of blood from the uterus through the vagina, taking place at extra or less regular monthly durations during the reproductive age of females[i].Menstrual disorders pose a huge burden on gynecology OPD, accounting for approximately 20 % of attendance[ii]. It has been described clinically in different ways, such as menorrhagia, metrorrhagia, menometrorrhagia, polymenorrhea, polymenorrhagia and oligmenorrhea[iii]. Normal cyclic period results from the arranged connection between the endomertium and its managing factors. Changes in both of these oftentimes brings about strange bleeding. It influences upto 33% of ladies of child bearing age[iv].
Thyroid hormones assume a significant part in reproductive physiology through direct impacts on the ovaries and by implication by communicating with sex hormone-binding globulin. Thyroid dysfunction can prompt menstrual problems and infertility[v]. The onset of thyroid disorders is growing with age, and 26% of premenopausal and menopausal women are reported to be diagnosed with thyroid disease[vi]. Thyroid disorders are prevalent globally, and thyroid conditions are 10 times more prevalent in women than in men[vii]. Since the 1950s, the effect of hypothyroidism on the menstrual cycle has been recognised, leading to changes in cycle length and blood flow[viii]. Menorrhagia is commonly observed in women with hypothyroidism. On the other hand, hyperthyroidism is associated with amenorrhea and oligomenorrhea, and the drop in flow is proportional to the magnitude of thyrotoxicosis[ix].
Thyroid autoimmunity has been shown to be associated with different forms of thyroid dysfunction. Operational intervention such as curettage and hysterectomy may be prevented through early diagnosis of thyroid dysfunction in patients with menstrual disorders and their management[x].
MATERIAL AND METHODS
The current research was performed in the Department of Obstetrics and Gynecology. 100 women each from the 15-45-year reproductive age group were chosen in study as well as in control group . The research group included women with menstrual disorders such as menorrhagia, oligomenorrhea, polymenorrhea, metrorrhagia, hypomenorrhea and amenorrhea and no detectable disease in the genital tract. Women with complaints other than menstrual disorders were in the control category. The research excluded patients with menstrual disorder with any known organic pathology, such as uterine fibroid, adenomyosis, tuberculosis, polyps, uterine malignancy, etc., and patients with intrauterine contraceptive device in utero.
Detailed demographic and personal history regarding age, parity, age of menarche, menstrual disorders and dysmenorrhea was taken. In women with menstrual complaints, general physical examination and pelvic examination were performed with special reference to thyroid dysfunction; in cases with a provisional diagnosis of AUB. To rule out the structural causes associated with menstrual irregularities, ultrasonography (USG-Abdomen and Pelvis with endometrial thickness) was performed. Patients were subjected to routine investigations (to rule out coagulation defects) such as Hb, BT, CT and platelets. All patients were subjected to Electro Chemiluminescence assay for T3, T4 and TSH estimation in their serum.
If TSH, T3, and T4 were within the normal range (TSH level = 0.39-6.16 μIU / ml, free T3 level = 1.4-4.2 pg / ml, and free T4 level = 0.8-2.0 ng / ml), patients were considered as euthyroid; when TSH was elevated with T3 and T4 below the normal range, they were classified as subclinical hypothyroidism. Overt hypothyroidism was diagnosed with high TSH and low levels of T3 and T4, subclinical hyperthyroidism with low TSH and normal levels of T3 and T4, and overt hyperthyroidism with low levels of TSH and high levels of T3 and T4.
Statistical analysis was done, for qualitative data to measure p value, Chi-square test and fisher exact test were used, and unpaired student t test and non-parametric Wilcoxon-Mann-Whitney test were used to statistically compare the quantitative data between two classes for T3, T4, TSH, and anti-TPO antibody values. The difference was deemed statistically significant with a p value of < 0.05.
RESULTS
Various parameters analyzed were
• Age
• Parity
• Menstrual irregularities
• Thyroid status
• Association of menstrual irregularities with thyroid dysfunction.
The study and control groups were comparable in respect of age
Of all the kinds of menstrual irregularities, 3 (3%) had amenorrhea, 52 (52%) had menorrhagia, 19 (19%) had oligomenorrhea, 15 (15%) had polymenorrhea and 11(11%) had metrorrhagia.
Table 1: Menstural Irregularities
55% of the cases in the study group were euthyroid while 45% of the cases were diagnosed of having thyroid disorder. While in control group 85% of the cases were euthyroid while 15% were having thyroid disorder
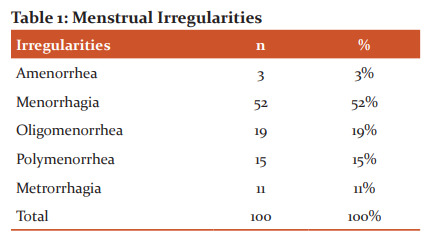
Table 2: Thyroid disorder in study and control group
In study group out of 45 cases having thyroid disorder of which 18 (18%) were overt hypothyroid and 11 (11%) were subclinical hypothyroid. Overt Hyperthyroid were 11 (11%) and subclinical hyperthyroid were 5% in study group. In control group one (1%) case was overt hypothyroid and 8 (8%) were subclinical hypothyroid, while 4 (4%) were over hyperthyroid and 2 (2%) ware subclinical hyperthyroid.
Thyroid anti TPO antibodies were present in 25 (25%) of the cases in study group as compared to 3 (6%) cases in control group. This difference was statistically significant (p<0.005).
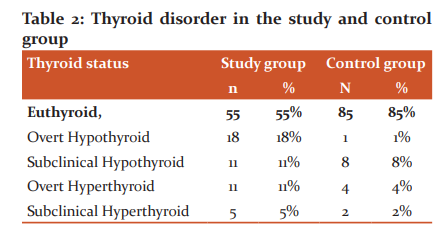
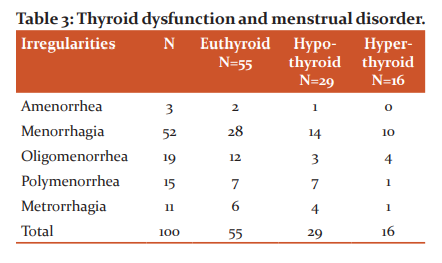
Table 3: Thyroid dysfunction and menstrual disorder
Of the total 3 amenorrhea cases 2 (2%) were euthyroid while 1 cases was hypothyroid. Out of 52 menorrhagia cases 28 were euthyroid, 14(14%) were hypothyroid and 10 (10%) were hyperthyroid. 19 were oligomenorrhea cases of which 7 (7%) each were euthyroid and hypothyrois while one case was hyperthyroid. Out of 11 metrorrhagia cases 6 (6%) were euthyroid, 4 (4%) were hypothyroid while 1 (1%) case was hyperthyroid.
DISCUSSION
Thyroid problems in general and hypothyroidism in particular is more commonly seen in women of reproductive age. Reproductive years and menopausal years are significantly influenced by the thyroid status of the women. Hypo and hyperthyroidism, both are associated with menstrual disturbances although hormonal and other biochemical aberrations are different9. Thyroid status of the women influences the menarche, pubertal growth and development, fertility and foetal development, menstrual cycles, postpartum period, reproductive years, and postmenopausal years.
In our study 53% of the cases were observed with menorrhagia which was most common complaint among the patients with menstrual disorders. Similar observations were seen in other studies f Pahwa et al[i] (50 %) and Padmaleela et al[ii] (50 %), where menorrhagia was the most common complaint. In the present study 55% were euthyroid in study group while 85% were euthyroid in control group. This shows the commonness of hypothyroidism and hyperthyroidism in patients with menstural problems is very nearly two times higher than in the control population. Kaur et al[iii] observed that 14% of the cases had hypothyroidism while in study by Pahwaa et al11 22 % cases of hypothyroidism and 76 % of euthyroidism were reported. Gowri et al[iv] observed 17.6 % women with hypothyroidism, 2.7 % with subclinical hypothyroidism, and 4.7 % with hyperthyroidism.
In the present study of the total 3 amenorrhea cases 2 (2%) were euthyroid while 1 cases was hypothyroid. Out of 52 menorrhagia cases 28 were euthyroid, 14(14%) were hypothyroid and 10 (10%) were hyperthyroid. 19 were oligomenorrhea cases of which 7 (7%) each were euthyroid and hypothyrois while one case was hyperthyroid. Out of 11 metrorrhagia cases 6 (6%) were euthyroid, 4 (4%) were hypothyroid while 1 (1%) case was hyperthyroid. Kaur et al13 observed that the patient with hyperthyroidism was found to have hypomenorrhea. Pahwa et al11 in their study observed that two hyperthyroid patients, both had menorrhagia. While Padmaleela et al.12 observed that among the hyperthyroid patients, 42.8 % had menorrhagia, 28.6 % had polymenorrhea, and 14.3 % had oligomenorrhea.
CONCLUSION
In this study strong correlation of thyroid dysfunction with menstrual disorders has been observed. Morbidity due to thyroid dysfunction in women can be reduced if diagnosed timely and treated accordingly and unnecessary hormonal treatment and surgery can be avoided.
Acknowledgement[D1]
Conflict of Interest: Nil
Source of Funding: Nil
References:
-
House S, Mahon T, Cavill S, editors. Menstrual hygiene matters. A resource for improving menstrual hygiene around the world. Module one: Menstrual hygiene –the basics. Available from URL: www.wateraid.org/~/media/Files/Global/MHM%20files/Compiled_L
-
Albers JR, Hull SK, Wesley RM. Abnormal uterine bleeding. Am Fam Physician. 2004 Apr 15; 69(8):1915-26.
-
Talukdar B, Mahela S (2016) Abnormal uterine bleeding in perimenopausal women: Correlation with sonographic findings and histopathological examination of hysterectomy specimens. J Midlife Health 7(2): 73-77.
-
Nicholson WK, Ellison SA, Grason H, Powe NR. Of ambulatory care use for gynecologic conditions; A national study. Am J Obstet Gynecol. 2001;184(4):523-30.
-
Poppe K, Glinoer D. Thyroid autoimmunity and hypothyroidism before and during pregnancy. Hum Reprod Update. 2003 Mar-Apr; 9(2):149-61.
-
Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, Braverman LE. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002 Feb; 87(2):489-99.
-
Cappola AR, Ladenson PW. Hypothyroidism and atherosclerosis. J Clin Endocrinol Metab. 2003 Jun; 88(6):2438-44
-
Bals-Pratsch M, De Geyter C, Müller T, Frieling U, Lerchl A, Pirke KM, Hanker JP, Becker-Carus C, Nieschlag E. Episodic variations of prolactin, thyroid-stimulating hormone, luteinizing hormone, melatonin and cortisol in infertile women with subclinical hypothyroidism. Hum Reprod. 1997 May; 12(5):896-904.
-
Manjeera LM, Kaur P. Association of thyroid dysfunction with abnormal uterine bleeding. Int J Reprod Contracept Obstet Gynecol 2018;7:2388-92.
-
Ajmani NS, Sarbhai V, Yadav N, Paul M, Ahmad A, Ajmani AK. Role of Thyroid Dysfunction in Patients with Menstrual Disorders in Tertiary Care Center of Walled City of Delhi. J Obstet Gynaecol India. 2016;66(2):115-119. doi:10.1007/s13224-014-0650-0
-
Pahwa S, Shailja G, Jasmine K. Thyroid dysfunction in dysfunctional uterine bleeding. J Adv Res Bio Sci. 2013;5(1):78–83.
-
Padmaleela K, Thomas V, Lavanya KM. Thyroid disorders in dysfunctional uterine bleeding (DUB) among reproductive age group women- a cross-sectional study in a tertiary care hospital in Andhra Pradesh India. Int J Med Pharma Sci. 2013;4(1):41–46.
-
Kaur T, Aseeja V, Sharma S. Thyroid dysfunction in dysfunctional uterine bleeding. Web Med Central Obstet Gynaecol. 2011;2(9):1–7
-
Gowri M, Radhika BH, Harshini V. Role of thyroid function tests in women with abnormal uterine bleeding. Int J Reprod Contracept Obstet Gynecol. 2014;3(1):54–57.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





