IJCRR - 13(1), January, 2021
Pages: 80-83
Date of Publication: 05-Jan-2021
Print Article
Download XML Download PDF
An Anatomical Study of the Acromian Process of the Scapula and its Clinical Implications
Author: Saurjya Ranjan Das, Manoj kumar Dehury, B Santa Kumari
Category: Healthcare
Abstract:Background: The acromion process of scapula projects perpendicularly from the lateral part of the spine of scapula. It is important because of its morphometric variations. It is associated with many ailments of the shoulder joint. The morphometric of acromion plays a vital role in impingement syndrome and the pathogenesis of rotator cuff disease.
Objective: The aim of the study was to measure and record the morphometric values and the morphology of the acromion process of the scapula.
Methods: The study was carried out on 72 dry adults human scapula of unknown sex and age. The acromion length, acromion breath, acromio coracoids distance, and the acromio glenoid distance was measured with the help of a digital vernier calliper. The morphology of the acromio process was also noted.
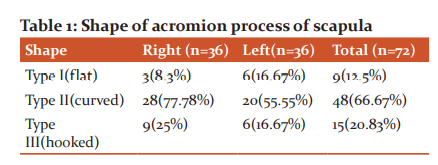
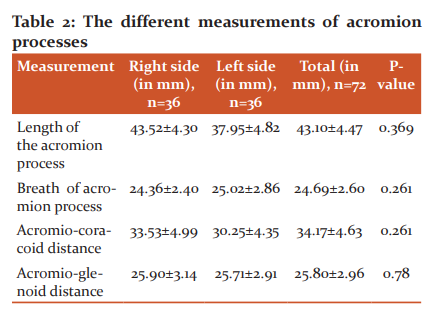
Result: The type II(curved) acromion was found to be the highest 48 cases (66.67%) followed by (hooked)type III in 15 cases (20.83 %). and the minimum is type I (flat ) in 9 cases (12.5%) The mean acromial length was 43.10\?4.47 acromial width was 24.69\?2.60. The mean acromio coracoids distance was 34.17\?4.63 and acromio glenoid distance was 25.80\?2.96.
Conclusion: The result of the present study will help the orthopaedics surgeons to treat the various pathology of the shoulder joint. It is of great interest of radiologists to interpret the MRI reports, Physiotherapists to mobilize to shoulder joint, Anthropologists to study the bipedal gait.
Keywords: Acromion, Morphometry, Rotator cuff diseases coracoids, Hooked
Full Text:
Introduction
The acromian process of scapula projects perpendicularly from the lateral end of the spine of the scapula. The acromian process has a tip medial and lateral borders with a dorsal and ventral surface. The crest of the spine of scapula becomes continues with the lateral border of the acromian. The medial end is short with a small oval facet for articulation was the lateral end of the clavicle to form acromio- clavicular synovial joint. The tip of the process gives attachment to the coroco acromial ligament. Thus the under the surface of anterior one-third of the acromial process, the coracoacromial ligaments and the coracoids process together form the coracoacromial arch which gives protection and stability to be shoulder joint.1
This arch prevents the upward dislocation of the shoulder joint and the subacromial bursa is present below this arch. The arch is fairly a non-elastic structure and the subacromial bursa, tendons of rotator cuff muscles and the long tendon of biceps passes beneath the arch.2 The rotator cuff is formed by the fusion of the tendons of the supraspinatus, sub scapularies, infraspinatus and tares minor. So when there is any pathology that causes, narrowing of the space, leads to impingement.
The study of morphometry of the acromial process is important as it is commonly involved impingement syndrome of the shoulder joint. The factor responsible for the syndrome can be classified into anatomical and functional. The anatomical cause includes the variations in shape and inclinations of the acromial and functional when there is the thickening of the rotator cuff due to chronic inflammation.3,4 Morphologically the acromial process is classified into three types by Bigliani et al.5
-
Type I (Flat)
-
Type II (Convex)
-
Type III (Hooked)
The morphometric knowledge of the variations of the acromian must be kept in mind during surgery of the shoulder joint. It will help the orthopaedic surgeons while doing surgical repair around the shoulder joint.6 Therefore the present study aimed to record the various dimensions and morphology of the acromial process of the scapula.
Material and Methods
The present study was carried out on 72 dry adult scapula of unknown sex and age from the medical colleges of eastern Odisha. The bones having external deformities were discarded and the bones with the intact acromial process were included. All the scapula were cleaned and labelled. The following measurement was taken with the help of digital vernier callipers and recorded in millimetres.
-
The maximum length of the acromial process (Anterior-Posterior distance along the long axis)
-
Maximum breath of acromial process (Distance between medial and lateral borders at the midpoint of acromial process)
-
Acromio coracoids distance (Distance between the tip of acromian and tip of the coracoid process.
-
Acromio glenoid distance (Distance between the tip of acromio to the supraglenoid tubercule.
-
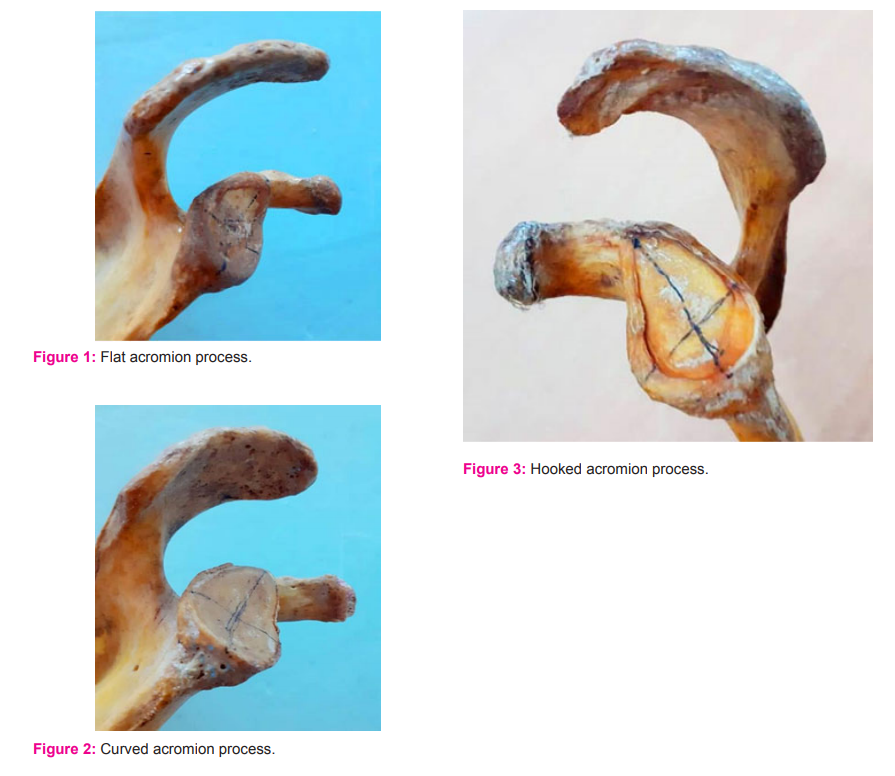
The type of acromion were classified into 3 types by Bigliani et al.
-
Flat (Type I)-figure. 1
-
Curved (Type II)-figure. 2
-
Hooked (Type III)-figure. 3
The above data were then statistically analysed using Microsoft excels software. The mean value, percentage and standard deviation were used to analyze the data. The ‘p’ value was obtained by using unpaired’ test. The difference was considered to be statistically significant if ‘p’ value was less than 0.05.
Results
In the present study of 72 dry scapulae it was found the shape of the acromial process was maximum in 48 cases (66.67%) was type II(curved) and the minimum is the type I (flat ) in 9 cases (12.5%) and hooked type III(hooked) in 15 cases (20.83 %). All the measures were tabulated in table 1.
The average length of the acromian process in the right side is 43.52 mm and that of the left side is 37.95mm. The mean value of acromial length in total samples is 43.10 mm. The mean value of acromial breath in total samples is 24.69 mm. The average breath of acromian process in the right side is 24.36 mm and that of the left side is 25.02 mm. The acromial coracoid distance average is 34.17 mm in total samples with 33.53mm on the right side and 30.25 mm on the left side.
The mean acromial glenoid distance was found to be 25.80 mm in total samples with 25.80 mm and 25.71mm in right and left side respectively. All the measures were tabulated in table 2.
Discussion
The morphometry measurements of the acromial process were closely associated with shoulder impingement and rotator cuff tear. The variations in the morphology of the acromial process play a vital role in shoulder girdle pathology. It is believed that the hooked acromial (type II) was mostly involved in rotator cuff lesions7. This can be explained by the fact that the size of subacromial space is decreased in hooked acromial which frequently leads to impingement of the rotator cuff.2
The scapula undergoes significant change during the evolution of the upper extremity due to increased functional demands of the prehensile limb. The spine of the acromial process of the scapula is increased during the development from the pronograde to the orthograde. This change is due to the progressive distal migration of the part of the insertion of the deltoid muscle with the acquisition of a tree limb.
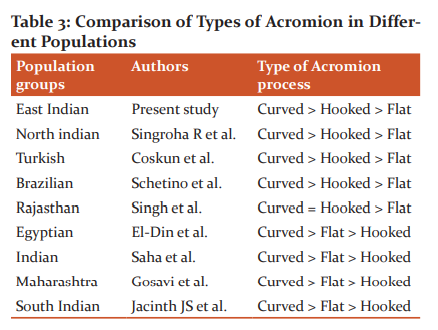
In the current study, the frequency of shape acromion process was highest for Type II (Curved) followed by type III (Hooked) and a very low incidence of Type I (Flat) scapulae. The findings were similar to Coskun ‘et al’.8Schetino ‘et al’.9 and Singhora ‘et al’10. However, high incidence of Type II, followed by Type I and less number of Type III acromion process was observed by El-Din et al.11, Saha et al.12 and Gosavi et al.7. All the measures were tabulated in table 3.
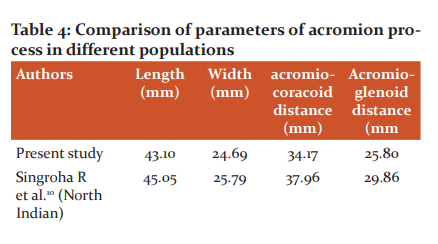
In the present study, we found that the mean value of acromion length, acromion width as 43.10 mm and 24.69 mm respectively which is similar to the studies done by Gosavi et al.7 where the mean length of the acromion was 43.7 mm and the mean width was 22.87 mm. and Singh et al. were the mean values of acromion length and acromion width as 46.1 mm and 23.2 mm respectively.2 Similar studies done by Coskun et al. and Singroha R et al. had reported the acromion length as 44.7 mm and 45.05mm respectively and acromion width as 23.60 mm and 25.79mm respectively.
The current findings of acromial length and breath are less than the studies done by Mansur et al13, El-Din et al11 and Paraskevas et al2 but more than the studies done by Sitha ‘et al’14.The acromio-coracoid distance and acromion glenoid distance in the current study found to be 34.17 mm and 25.80 mm respectively which is very similar to the studies done by Vinay G ‘et al’15 in which the acromio-coracoid and acromio glenoid distance was 34.05mm and 30.05mm respectively. The present study data shows lesser values compared to the studies done by Mansur ‘et al’ and Singh ‘et al’ but higher than the studies done by Gosavi ‘et al’, El-Din et al and Coskun et al. All the measures were tabulated in Table 4.

Conclusion
The acromial process plays a vital role in the stability and formation of the shoulder joint. The study of anatomical variation of the acromial process will help the surgeons to treat rotator cuff pathologies and shoulder impingement syndrome. It is also important in forensic investigations and racial determination thus helpful for forensic exports and anthropologist. It will also hold physiotherapist to mobilize the frozen shoulder and to increase its mobility.
References:
[1] Singh J, Pahuja K, Agarwal R. Morphometric parameters of the acromion process in adult human scapulae. Indian J Basic Appl Med Res 2013; 8(2): 1165-70.
[2] Paraskevas G, Tzaveas A, Papaziogas B, Kitsoulis P, Natsis K, Spanidou S. Morphological parameters of the acromion. Folia Morphologica 2008; 67(4): 255-60.
[3] Mansur DI, Khanal K, Haque MK, Sharma K. Morphometry of the acromion process of Human Scapulae and its Clinical Importance Amongst Nepalese Population. Kathmandu Univ Med J 2012; 38(2): 33-36.
[4] Edelson JG, Taitz C. Anatomy of the coraco-acromial arch. Relation to degeneration of the acromion. J Bone Joint Surg Br 1992; 74: 589–594.
[5] Bigliani LU, Morrison DS, April EW. The morphology of the acromion and rotator cuff impingement. Orthop Trans 1986; 10: 228.
[6] Gupta C, Priya A, Kalthur SG, D Souza AS. A morphometric study of the acromion process of the scapula and its clinical significance. Chrismed J Health Res 2014;1:164-9.
[7] Gosavi S, Jadhav S, Garud R. Morphometry of acromion process: A study of Indian scapulae. Int J Pharma Res Health Sci 2015;3(5):831-5.
[8] Coskun N, Karaali K, Cevikol C, Demirel BM, Sindel M. Anatomical basics and variations of the scapula in Turkish adults. Saudi Med J 2006;27(9): 1320-5.
[9] Schetino LPL, Sousa RR, Amâncio GPO, Schetino MAA, Almeida-Leite CM, Silva JH. An anatomical variation of acromions in Brazilian adult’s scapulas. J Morphol Sci 2013;30(2):98-102.
[10] Singroha R, Verma U, Malik P, Rathee SK. Morphometric study of the acromion process in scapula of the north Indian population. Int J Res Med Sci 2017;5:4965-9.
[11] El-Din WAN and Ali MHM. The patterns of the Acromion process and Glenoid cavity in Egyptian scapulae. J Clin Diag Res 2015;9(8): AC08-AC11.
[12] Saha S, Vasudeva N, Paul S, Gautam VK. Study of acromial morphology in Indian population. Rev Arg de Anat Clin 2011;3(2):84-8.
[13] Mansur DI, Khanal K, Haque MK, Sharma K. Morphometry of Acromion Process of Human Scapulae and its Clinical Importance amongst Nepalese Population. Kathmandu Univ Med J 2012;38(2):33-6.
[14] Sitha P, Nopparatn S, Aporn CD. The Scapula: Osseous Dimensions and Gender Dimorphism in Thais. Siriraj Hsop Gaz 2004;56(7):356-365.
[15] Vinay G, Sivan Sheela. Morphometric study of the acromion process of the scapula and its clinical importance in South Indian population. Int J Anat Res 2017; 5(3.3):4361–4364
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





