IJCRR - 8(4), February, 2016
Pages: 19-24
Date of Publication: 21-Feb-2016
Print Article
Download XML Download PDF
SPECTRUM OF LESIONS IN URINARY BLADDER -A HISTOPATHOLOGICAL STUDY
Author: Pooja Y. Shah, Monika Nanavati, Ravi G. Patel, Hansa M. Goswami
Category: Healthcare
Abstract:Background: Diseases of the bladder, particularly inflammation (cystitis), constitute an important source of clinical signs and symptoms. Tumors of the bladder are an important source of both morbidity and mortality. Objectives: 1) To study the histopathological features of various lesions in bladder. 2) To study the frequency of different pathological lesions, particularly Papillary Urothelial Neoplasms in urinary bladder. Results: 35 cases of urinary bladder were received. Out of 35 patients, 27 were males and 8 were females with male to female ratio being 3.38:1.The spectrum of pathological lesions included inflammations, metaplastic lesions, cystic lesions and tumors. Out of 35 cases 12(34.28%) were Non neoplastic lesions and 23(65.71%) were Neoplastic lesions. Among the non neoplastic lesions cystitis (41.67%) was the most common finding. Others were non-specific inflammation due to various etiology, hydatid cyst, benign epithelial inclusion cyst and abscess. Most common age groups affected by the neoplastic lesions were 41-50 years and 61-70 years with male to female ratio being 2.29:1. Among the neoplastic lesions 19(82.60%) cases were of urothelial neoplasms, others being Squamous Cell Carcinoma, Poorly Differentiated Carcinoma with Neuroendocrine differentiation and Paraganglioma. Most common Urothelial neoplasm was Non invasive Papillary Urothelial Carcinoma, Low Grade (9 cases). Among all the bladder biopsies received there was no muscle layer in 3 cases (8.3%). Conclusions: Our study has revealed that the bladder tumors are the commonest lesions in the urinary bladder tissues received and Papillary Urothelial Neoplasms were the predominant tumor type.
Keywords: Bladder, Papillary urothelial neoplasms, Paraganglioma.
Full Text:
INTRODUCTION Diseases of the bladder, particularly inflammation (cystitis), constitute an important source of clinical signs and symptoms. Usually, however, these disorders are more disabling than lethal. Neoplasms of bladder pose biologic and clinical challenges [1]. Tumors of the bladder are an important source of both morbidity and mortality. It is the second most common malignancy seen by the urologist[2]. Various risk factors include cigarette smoking, industrial exposure to acrylamine, schistosoma hematobium, cyclophosphamide, artificial sweeteners and long-acting use of analgesics. How these influence to induce cancer is unclear, but a number of cytogenetic and molecular alterations are heterogeneous [3].
In general, the prevalence of bladder tumours in developed countries is approximately 6 times higher compared with that in developing countries. The most common type of bladder cancer in developed countries is urothelial carcinoma, derived from the uroepithelium, which constitutes more than 90% of bladder cancer cases in USA, France or Italy. However, in other regions (e.g. Eastern and Northern Europe, Africa, Asia) the relative frequency of urothelial carcinoma of the bladder is lower [4]. The relative frequency of histological subtype of bladder carcinoma depends on the clinical setting. About 90% of bladder carcinoma reported from the West is transitional cell type. In large series reported from Egypt, squamous cell carcinoma (SCC) accounted for 59– 73% of bilharzial bladder cases which are endemic areas for Schistosoma Haematobium[3].
Objectives:
1) To study the histopathological features of various lesions in bladder.
2) To study the frequency of different pathological lesions, particularly Papillary Urothelial Neoplasms in urinary bladder.
MATERIAL AND METHODS Source and Method of collection of data: This was a four years (January 2012 to October 2015) retrospective study conducted in histopathology section of Department of Pathology, B.J Medical College, Civil Hospital Ahmedabad, Gujarat from January 2012 to October 2015. All specimens of urinary bladder were included in the study. Patient’s age, sex and other details were retrieved from the request forms manually. The data was analyzed with emphasis on age, sex and histology. The surgical specimens were fixed in 10% formalin. Surgical specimens were examined grossly concerning the size and shape of material and were processed routinely. Light microscopic technique was used for diagnosis. Special stains and immunohistochemistry were applied, where ever required.
RESULTS Out of 35 cases, 12 (34.28%) were non neoplastic lesions and 23 (65.71%) were neoplastic lesions (Table 1). Among the non neoplastic lesions most common lesion was cystitis (41.67%), with 2 cases of cystitis glandularis (metaplasia), 1 of cystitis cystica, 1 of polypoid cystitis and 1 of eosinophilic cystitis. Cases of non specific inflammation constituted 4 cases (33.33 %) of non neoplastic lesions. Among them 2 were associated with trauma,1 with fistula and 1 with diverticulum. Among the other non neoplastic lesions there were Benign Epithelial Inclusion Cyst, Abscess and Hydatid Cyst, 1case (8.33%) of each.
Table 2 shows histopathological spectrum of non neoplastic lesions of urinary bladder. Among the neoplastic lesions most common was Papillary Urothelial Neoplasm 19 cases(82.60%) with 2 cases of Squamous Cell Carcinoma(8.69%),1 case of Poorly differentiated Carcinoma of Neuroendocrine Differentiation (4.35%) and 1 case of Paraganglioma(4.35%)[Table 3]. Among the urothelial neoplasms, most common were Papillary Urothelial Carcinoma, Low Grade with 9 cases(47.36%) [Table 4]. Most common age groups affected by the neoplastic lesions were 41-50 years and 61-70 years with male to female ratio being 2.29:1[Table 5]
DISCUSSION Cystoscopy is the primary diagnostic tool in the diagnosis of urinary bladder carcinoma. The histopathological study of the cystoscopic biopsy not only gives the diagnosis but also provides the additional information to the urologist that can have impact on the treatment. Out of 35 patients, 27 (77.14%) were males and 8(22.86%) were females with male to female ratio being 3.3:1.Among the neoplastic lesions out of 23 cases, 16(59.26%) were male and 7(40.74%) were females with male to female ratio being 2.28:1.Similar finding were seen in several studies of cystoscopic biopsy.[5-8] Bladder carcinoma is more common in elderly males. The most common age groups of presentation of neoplastic lesion of the bladder were 41-50 years and 61-70 years, followed by 51-60 years. This is similar to that reported in the existing literature [6,9,10]. Out of 35 cases 12(34.28%) were non neoplastic lesions most common being cystitis. Out of 5 cases of cystitis 2 cases were of Cystitis glandularis and 1 each of cystitis cystica, polypoid cystitis and eosinophilic cystitis.
Out of 4 cases of non specific inflammation 2 were associated with trauma, one with diverticula and another with fistula formation. One case was of Hydatid Cyst in the bladder which was also associated with hydatid cyst of liver and kidney. One case of epithelial inclusion cyst was there in our study.One case of abscess in the muscular wall was also there in our study. Out of 35 cases 23(65.71%) were neoplastic lesions. Among the neoplastic lesions urothelial neoplasms were most common consisting of 19(82.60%) cases. There was no detrusor muscle in 3(15.79%) cases of urothelial neoplasm to assess the muscle invasion. Laishram et al [6] could also assess only 83% cases for invasion and out of that 42.1% cases showed muscle invasion [6].Muscle invasion was seen in 26.31% cases of urothelial neoplasm in study done in Nepal [11].The same study showed 26.7% cases of invasive urothelial carcinoma. Other studies showed 35.8%, 27.2% and 26% of muscle invasion in urothelial carcinoma respectively [7,12,13]. Comparable to these, in our study 26.31% of Urothelial Neoplasms showed muscle invasion. About 70 % of all carcinomas of the urinary bladder are either non- invasive (pTa) or only minimally invasive (pT1) at the time of presentation[14].
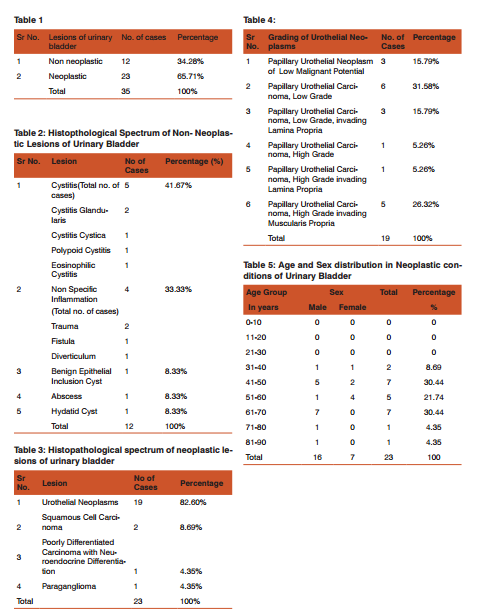
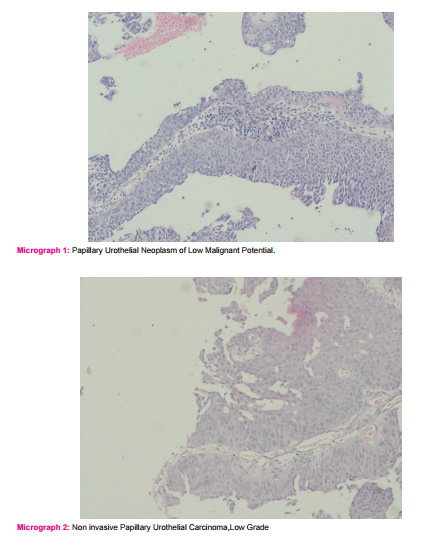
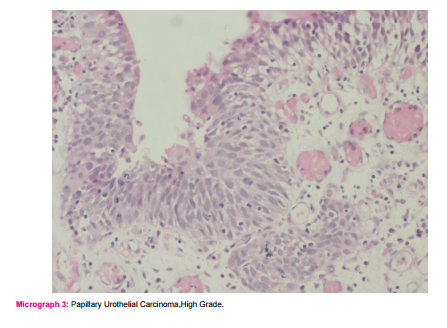
Correct histologic grading and tumor staging is crucial for proper and optimal patient management. The corner stone of bladder cancer diagnosis, treatment and staging is a high quality transurethral resection of the bladder tumor (TURBT) [15]. In our study most common urothelial neoplasm were Papillary Urothelial carcinoma,Low Grade consisting 9 cases out of 19 cases with 3 showing lamina propria invasion and in two cases biopsy were inadequate. There were 7 cases of Papillary Urothelial carcinoma, High Grade with 5 cases showing muscularis propria invasion, one showing lamina propria invasion and in one case biopsy was inadequate. In most analysis, less than 10% of low grade cancers invade, but as many as 80% of high grade TCC are invasive [17]. In our study 3 cases were of Papillary urothelial neoplasm of low malignant potential.
As compared to Matalka et al observations, their study showed 40% cases of high grade TCC and 60% of low grade TCC. In our study 47.36% of urothelial neoplasms were Low Grade(Micrograph 2),36.84% were High Grade(Micrograph 3) and 15.79% were with Low Malignant Potential(Micrograph 1). In our study there were only 2 cases of Squamous Cell Carcinoma. In contrast to the studies done in South East Asian countries and Western countries,
Nigeria has squamous cell carcinoma as the most common type of urinary bladder carcinoma. This is because of high frequency of association of squamous cell carcinoma with schstosomiasis [17]. However this pattern has been changing in Egypt in the last few years. There is decline in squamous cell carcinoma and increase in urothelial carcinoma [18]. In India there is only a focus of population infected by Schistosomia haematobium as compared to other countries[19]which explains lower incidence of Squamous cell carcinoma of bladder. Our study showed one case of Poorly Differentiated Carcinoma with Neuroendocrine Differentiation which was confirmed by IHC. Tumor was positive for NSE and negative for Chromogranin.
CONCLUSIONS Our study has revealed that the bladder tumours are the commonest lesions seen in the received specimens of bladder tissue and Papillary Urothelial Neoplasm was the predominant tumour type. Besides, other investigations, cystoscopic bladder biopsies help in the early diagnosis and treatment of various bladder lesions. This study documents a high frequency of urothelial tumor, mostly non invasive papillary urothelial neoplasm, low grade with a male preponderance in the age group above 40 years. Invasion to the muscle layer correlates with high grade tumor. Hence, inclusion of detrusor muscle in the cystoscopic biopsy is very important.
References:
1. Vinay Kumar, Abbas AK, and Fausto N. The lower urinary tract and male genital system. Robbins and Cotran. Pathologic basis of disease. 9th Edition. Philadelphia:Saunders 2004; 1026-1036.
2. Matalka et al. Transitional cell carcinoma of the urinary bladder: a clinicopathological study. Singapore Med J 2008; 49(10): 791.
3. Hasan SM et al. Frequency of transitional cell carcinoma in local suburban population ofkarachi. JLUMHS 2007; 83-85.
4. Beltran AL et al. Infiltrating urothelial carcinoma. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. IARC Press: Lyon 2004; 93-109.
5. Al- Samawi AS, Aulaqi SM. Urinary bladder cancer in Yemen. Oman Med J 2013; 28: 337-40.
6. Laishram RS, Kipgen P, Laishram S, Khuraijam S, SharmaDC. Urothelial tumors of the urinary bladder in Manipur: ahistopathological perspective. Asia Pacifi c Journal of CancerPrevention. 2012; 13: 2477-9.
7. Viadya S, Lakhey M, KC S, Hirachand S. Urothelial tumors ofthe urinary bladder: a histopathological study of cystoscopicbiopsies. J Nepal Med Assoc 2013; 52: 475-8.
8. Kumar UM, Yelikar BR. Spectrum of lesions in cystoscopicbladder biopsies- a histopathological study. Al Ameen J MedSci 2012; 5: 132- 6.
9. Stepan A, Simionescu C, Margaritescu C, Ciurea R. Histopathological study of the urothelial bladder carcinomas.Current health Science Journal 2013; 39:147-150.
10. Islam AHMT, Mostafa SN, Rahman M, Nahar Z. Role of ultrasound in the evaluation of urinary bladder neoplasm with histopathological correlation. Journal of Teachers Association TAJ 2008; 21:155-9.
11. Nepal Med Coll J 2014; 16(1): 9-12 Cystoscopic bladder biopsies: A histopathological studyPudasaini S,1 Subedi N,2 Prasad KBR,1 Rauniyar SK,1 Joshi BR,2 Bhomi K K 2
12. Biswas RR, Mangal S, Guha D, Basu K, Karmakar D. Anepidemiological study of cases of urothelial carcinoma ofurinary bladder in a tertiary care centre. Journal of KrishnaInstitute of Medical Sciences 2013; 2: 82-8.
13. Gupta P, Jain M, Kapoor R, Muruganandham K,Srivastava A, Mandhani A.Impact of age and gender on the clinicopathological characteristics of bladder cancer. Indian J Urol 2009; 25: 207-10.
14. I. Tosoni .U. Wagner, G Sauter. MEG Coff et al. Clinical Significance of Inter Observer Differences in the Staging and Grading of Superficial Bladder Cancer. BJU International 2000;85:48- 53.
15. Peter J Bostrom, Bas W.G. Van Rhijn, Neil Fleshner et al. Staging and Staging Errors in Bladder Cancer. European Urology Supplements 2010;9:2-9.
16. Mahesh Kumar U and B.R. Yelikar, Spectrum of Lesions in Cystoscopic Bladder Biopsies: A Histopathological study. Al Ameen J Medical Sci 2012;5 (2):132-136.
17. Felix AS, Soliman AS, Khaled H et al. The changing patterns of bladder cancer in Egypt over the past 26 years. Cancer Causes and Control 2008;19: 421-9.
18. Eble JN, Sauter G, Epstein JI, Sesterhenn IA, editors. World Health Organization of tumors- tumors of the urinary system and male genital organs. IARC Press, Lyon, 2004.
19. The global status of schistosomiasis and its control , L. Chitsulo, D. Engels, A. Montresor, L. Savioli, Acta Tropica 77 (2000) 41–51.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





