IJCRR - 13(1), January, 2021
Pages: 31-40
Date of Publication: 05-Jan-2021
Print Article
Download XML Download PDF
Efficacy of Unani Formulation in Cervical Ectopy (Quruhal Rahim) - An Open Observational Study
Author: Shamim Ansari, Wajeeha Begum, Kouser Fathima Firdose
Category: Healthcare
Abstract:Introduction: Cervical ectopy (quruhal rahim) is a benign and common gynaecological condition. About 80-85% of women suffer from Cervical Erosion. Clinically the patient may present with vaginal discharge, low backache, contact bleeding in the form of post-coital bleeding or intermenstrual bleeding, dyspareunia, etc. Cervical erosion is diagnosed by per speculum examination. Considering these facts methi, alsi,babuna, nakhuna, Karam Kala, has been selected to evaluate the efficacy in the form of Abzan in Quruhal Rahim.
Objective: To evaluate the efficacy of Abzan in Quruhal Rahim with Unani formulation.
Methods: Clinically diagnosed patients (n=30) with Married women between the age group of 18-45yrs. Having symptoms of vaginal discharge, normal or inflammatory changes in pap smear were included and patients with malignancy, Pelvic inflammatory disease, systemic illnesses & sexually transmitted disease, oral contraceptive Pills and Intrauterine contraceptive device, pregnancy and lactation were excluded. After menses use daily one time for sitz bath for 15minuts for 21 days. Cervical ectopy by arbitrary grading scale and SF-12 for Quality of life were health-related quality of the life is measured by SF-12 Questionnaire to provide easily interpretable scales for physical and mental health.
Result: Vaginal discharge mean score before and after treatment is 2.37\?0.57 and0.367\?0.49 respectively with p< 0.0001. In cervical erosion, grading means score before and after treatment is 1.7\?0.65 and 0.47\?0.58 respectively with a p< 0.0001. Highly significant improvement is found in subjective and objective parameters.
Conclusion: This data suggests that the test drugs were safe, effective in improving and relieving symptoms of cervical erosion. Further, research in a larger sample size for longer duration is recommended.
Keywords: Quruhalrahim, Cervical ectopy, Abzan, Arbitrary grading scale, SF-12 for QOL, Vaginal discharge
Full Text:
INTRODUCTION
Cervical erosion is also known as cervical ectopy. It is a benign lesion and a common gynaecological condition seen in outpatient departments.1,2 About 80-85% of women suffer from cervical erosion3. It is the commonest finding in routine pelvic examinations during the fertile age group11. Pathologically cervical erosion is a condition where squamous epithelium of the ectocervix is replaced by the columnar epithelium of the endocervix.3 The exposed columnar epithelium looks red because of the blood vessels just below the surface.4 A single layer of glandular cells that reside in close association with the underlying vascular cervical stroma appear. It is thin and vascularized epithelium fragile tissue. With easy access to the blood and lymphatic systems, there are decreased mucosal barriers to sexually transmitted infections (STIs), including HIV. Prior observational epidemiological studies have suggested that cervical ectopy can increase the risk of acquiring diseases like chlamydia trachomatis, human papillomavirus, and cytomegalovirus, but not Neisseria gonorrhea.5
The common causes of ectopy are trauma by multiple childbirths, tampon use of intrauterine contraceptive device chemicals, infections, hormones (oral contraceptive pills) or carcinoma etc. Cervical ectopy is more common in women of lower socioeconomic groups, poor general hygiene, early marriage and multiple pregnancies.6
Clinically, the patient may present with vaginal discharge, low backache, contact bleeding in the form of post-coital bleeding or intermenstrual bleeding, dyspareunia, etc.7 Cervical erosion is diagnosed by per speculum examination. It reveals a bright red area surrounding and extending beyond the external os in the ectocervix. The outer edge is demarcated. It may be smooth or having small papillary folds. It is neither tender nor bleeds to touch.7 It is asymptomatic and physiological then needs no treatment but when it is symptomatic and infected then the treatment is needed.3,7 Cryo cauterization, electrocoagulation and cautery with laser is the treatment of choice. Side effects like prolonged excessive mucoid discharge per vagina, seldom cervical stenosis, accidental burns, bleeding and recurrence are associated with this treatment6. In classical Unani literature which is caused by external factors such as wound due to trauma, instrumentation, a drug which is caused by external factors such as wounds due to trauma, instrumentation, drug-induced i.e use of haad drugs in the form of humool, or internal factors like difficult labour or mismanagement of labour, sometimes, it may be because of acute yellow bile causing gradual erosion of cervix due to its acute nature or inflammation and rupture of pustules.,8,9 In symptoms like backache, pelvic pain, abnormal vaginal discharge, excessive tiredness etc. Use of (relaxant) drugs is harmful while qabiz (astringent) drugs are beneficial in its treatment.8-10,
Unani system of medicine has several drugs available for healing of cervical ectopy as a local treatment in the form of sitzbath, which are safe and cost effective. In present study research drug comprises of Methi (Trigonella foenum graeceum) 5gms, alsi (Linum usitatissimum) 5gms, babuna (Matricaria chaemomilla) 3gms, nakhuna ((Trigonella uncata) 5gms, karmkalla ka dant’hal (Brassica oleracea)10gms Joshanda is prepared in 2 lots of warm water. After menses use daily one time forsitz bath for 15minuts for 21 days.11 In unani system of medicine various drugs with medicinal properties like munzij, muhallilawram (anti-inflammatory), jaali (detergent), muqawiebadan, mushil ( laxative), mujaffif, mudammilquruh, dafi-i-taffun, mullayan, mussakinetc are used locally to treat this disease.
Materials and Methods
Study design: An open observational study
Study duration: One and a half years from March 2019 to January 2020
Study centre: OBG Dept. National Institute of Unani Medicine Hospital, Bangalore.
Sample size: 30 patients
Ethical clearance No.: Ethical clearance was obtained from the institutional ethical committee vide no NIUM/ IEC/2017-18/013/ANQ/05; and CTRI registration done vide no.CTRI//2019/03/024426.
Informed consent: all participants gave written informed consent before study
Drugs Identification: was done at FRLHT Bengaluru. with an acc. No. 5510-5514
Participants
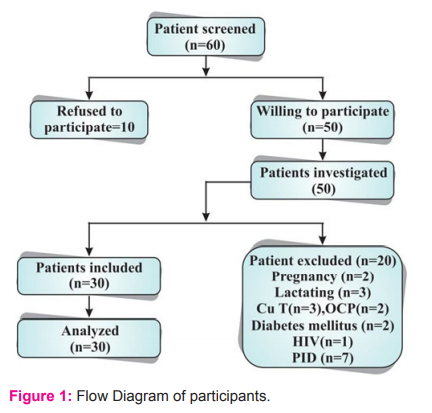
Total 60 patients were screened for the study, 10 patients refused participation and 20 patients didn’t meet the inclusion criteria, hence were excluded. 30 patients were allocated in- an open observational study.
Selection criteria
Married women between the age group of 18-45 yrs. Having symptoms of vaginal discharge, low backache, dyspareunia, post-coital bleeding, normal or inflammatory changes in pap smear were included and patients with malignancy, PID, systemic illnesses like Hypertension, diabetes mellitus & STIs, OC Pills and IUCD’s, pregnancy and lactation were excluded.
Study procedure
The patients fulfilling the inclusion criteria were enrolled after explaining the study in detail and receiving informed consent. In each patient, history was evaluated and a complete physical examination including breast, abdominal examination and per vaginal examination was performed. Personal details, history, clinical features and investigations were recorded in the Case record form structured for the study.
Criteria for selection of drug
The research drug possesses properties like muhallilewaram, mujaffif, mudammilequruh, dafi-i- ta’ffun,qabid, musakkin,12-17 properties. Moreover, pharmacological studies show that research drug exhibit antimicrobial, anti-inflammatory, antioxidant, anti-cancer, anti-ulcer, analgesic, hepatoprotective wound healing activities.13,14,18-20 Further methi, alsi, nakhoona, baboona, karamkallacontains flavonoids, saponins (glycosides), alkaloids (terpenoids, steroids) arachidonic acid, ethanol, histamine, leukotrienes, polysaccharides, saponins (glycosides), carbohydrates, tannins, triglisoraletc13,14,18 which are considered as the active principle of anti-ulcer activity. Flavonoids are a group of the polyphenolic compound having anti-ulcerogenic, anti-inflammatory, anti-bacterial, antioxidants properties4 which provide strength to the mucosal barrier & promote the ulcer to heal fast.20 The wound healing activity of Unani formulation as abzan might protect against microbial invasion by providing better tissue formation. Further, it enhances the rate of wound healing & tissue epithelization.4 Thus, research Unani formulation is anticipated to be effective in the healing of cervical ectopy and relieving the associated symptoms.
Method of preparation
The best quality of methi, alsi, babuna,nakhuna, and karmkalla was provided by the pharmacy of NIUM and was further authenticated by FRLHT Bengaluru. with an acc. No. 5510-5514. All the drugs were finely powdered. Drugs were weighed and mixed. The powdered drugs were dispatched in plastic self-lock bags. To avoid any confusion regarding dosages one lock bag was used to dispatch 28gm of the drug for a single day which was to be used daily for one measure for sitz bath. So every patient was given 7 packets of the drug for one week at each visit and continued for 3 weeks. Treatments were given locally.
Initial assessment and laboratory screening
Baseline Laboratory investigations like haemoglobin percentage, total leucocyte count, differential leucocyte count, erythrocyte sedimentation rate, Veneral Disease Research Laboratories test and random blood sugar were done to exclude general diseases. Ultrasonography of pelvis was done to exclude pelvic pathology. Pap smear was done to exclude genital malignancy in each case. Assessment of the extent of erosion was graded as 0, 1, 2 and3; as follows. Grade 0: No erosion Grade 1: covering 1/3rdof cervix Grade 2: from 1/3rd to 2/3rd area of the cervix, and Grade 3: overs 2/3rd of the cervix. The assessment was done before treatment, at .each follow up during treatment and after treatment. Patients were also enquired for any side effects during the trial. Assessment of Health-related quality of life (HRQol) was assessed by the SF-12 questionnaire. Assessment of low backache is done by using the Visual Analogue Scale (VAS). Assessment of vaginal discharge was graded from 0 to 4 grade: score: 1-No discharge; 2- Mild ( No staining or moistness of undergarments); 3-Moderate (stain on undergarments); Score:4- severe (using pads). Dyspareunia and post-coital bleeding were based on the arbitrary four-point scale (0= None,1=Mild,2= Moderate, 3= Severe ). Treatment was subsequently started in patients fulfilling the inclusion criteria.
Intervention
Joshanda of methi (Trigonella foenum graceum) 5gms, alsi (Linum usitatissium graceum) 5gms, babuna (Matricaria chaemomilla) 3gms, nakhuna (Trigonella uncata) 5gms, karmkalla ka danthal (Brassica oleracea) 10gms was prepared by soaking the drugs in 400ml of water for the whole night. Next day in the morning the soaked drugs with water was boiled until it was concentrated to 180 ml. Abzan were prepared according to the standard method of preparation. It was used for 15minuts daily for 21 days after menses. Assessment of erosion and health-related quality of life (HRQol) was done at baseline, each follow up during treatment (weekly) and after treatment (once in 15 days for a month). Patients were also enquired for any side effects during the trial. Patients were advised to maintain personal hygiene and avoid intercourse during the treatment.
Subjective parameters: Vaginal discharge, low backache, contact bleeding, dyspareunia
Objective parameters:
(Direct visual assessment of the appearance of cervix, healing of erosion and vaginal discharge).
Outcome measures:
Primary outcome measure: changes in white discharge and low backache.
Secondary outcome measure: Improvement in cervical ectopy grading and SF-12 (12 items short-form survey) Health Questionnaire score ( Figure 1).
Statistical analysis
Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5 % level of significance. The Statistical software namely SPSS 22.0, and R environment ver.3.2.2 were used for the analysis of the data and Microsoft Word and Excel have been used to generate graphs, tables etc.22,23
RESULTS AND DISCUSSION
The present study entitled “Efficacy of Abzan with Unani formulation in Quruhal Rahim - An open observational study” was effective in the healing of cervical erosion and relieving the symptoms. In the present study, it was demonstrated that complete healing of cervical ectopy was achieved in 56.7% of patients with a mean of 1.7±0.66 & 0.47±.57before and after respectively. Vaginal discharge was improved in 63.3% of patients with a mean of 2.37±0.56 and 0.37±0after treatment respectively. While it persists in a mild form in 36.7%. Low backache was relieved in 90% patients, and remains 10% in a mild form, with mean of 1.93±0.37 and 0.1±0.36. Highly significant improvement in vaginal discharge and low backache was might be due to healing of cervical ectopy, which causes relief in these symptoms. No adverse effect of research Unani formulation was reported during the study.
Demographic characteristics
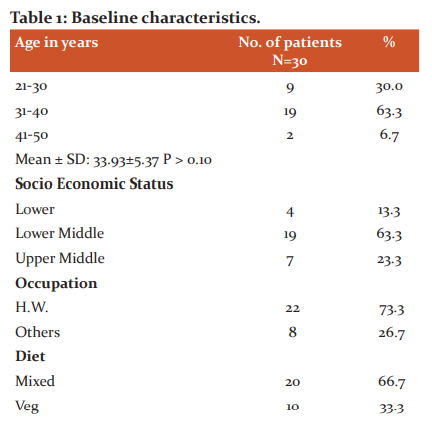
Age: Majority of the patients (63.3%) were in the age group of 31-40 years & remaining 30% were in 21-30 years and 6.7% in 41-50 years of age. Hashmi S et al.24and Mirza S et al25Patil P et al. 26Latafat T et al.27reported 40% and 44% in two groups in 31-35 yrs., reported 39.2% in 31-40 yrs, reported 40% &37.8% in 26-30 yrs. respectively. The result of present study correlates with the above studies. Evidence suggests that cervical ectopy is common in women of reproductive age group.4,7 Mean±SD of the age of patients was 33.93±5.37, which is by the study of Jindal M et al.2 who reported 31.32 and 33.7 in two groups, Al- Kaseer reported28 27.1 ± 5.9, Cekmez Y et al.29 reported 34.4±4.3.
Socioeconomic status: In the present study, 23.3% of patients belong to an upper-middle-class, 63.3% to lower middle class and 13% to the lower class. Hashmi S et al.24 reported 43.3% of patients in the upper-lower, 36.6% in the upper middle, 16.6% in the lower-middle and 13.3% in the lower class. Mirza S et al.25reported 42.2% of patients in the upper lower class, 40% in the lower middle, 11.1% in the upper middle & 6.7% in the upper class. Shivanna et al. 30reported 72% and 75% patients respectively from low Socioeconomic status. Gautam A et al.31 reported majority of the patients belong to lower middle class. Bengal V. B. et al.32 reported that maximum patients having cervical ectopy belong to low socioeconomic class, low literacy level, poor personal hygiene and poor health awareness. Literature report says that low socio-economic status predisposes to poor nutrition, poor personal hygiene leading to infection which may cause cervical ectopy.32,33
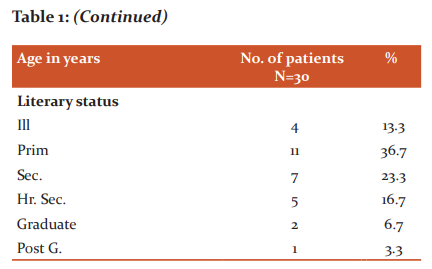
Literary Status: Most of the patients had low educational level i.e.; 36.7% patients had primary school education, while 13.3% were illiterate, 23% & 16.7% had education up to secondary and higher secondary school while graduate and postgraduate are 6.7% and 3.3 % respectively. Mirza S etal.25reported 20% illiterate, 33.3% had middle school education, 10% each in primary school and high school & 13.3% graduate. Hashmi S et al.24 reported44.44% illiterate, 20% had middle school education & 13.3% had education in each primary, secondary and higher secondary. Gautam A et al.31reported 40% of the patients had a high school education. Al-Kaseer et al.28 reported low educational level among patients of cervical ectopy.
Occupation: In this study housewife are more affected than the working class. Out of 30 patients, 73.3% of patients are of housewife affected with cervical erosions whereas 26.7% are working women.
Dietetic habit: In this study out of 30, 20(66.7%) patients are of mix diet. Whereas 10(33.3 %) are vegetarian. In the Unani system of medicine, importance has been given to dietetics in health and disease.34Unaniphysicians mentioned certain foods which are to be taken and to be avoided according to age, season, place, and mizaj of the person. The temperament of meat is har when consumed in excessive quantity; it causes increase production of khilte dam and can lead to amrazedamvi. As, mentioned earlier that cervical erosion with cervicitis is a damvi marz,35 it may be assessed that non-vegetarian diet has its impact on this disease as per the mizaj and akhlat theory.
Mizaj: Most of the patients, 86.7 % possessed damwimizaj, while 13.3% had balghamimizaj, none of the patients had safrawi or saudawimizaj, which agrees with the studies of Hashmi S et al.24 reported 66.67 % patients with damwimizaj, Mirza S et al.25 reported 53.3% with damwimizajMoreover, it coincides well with the theories of eminent Unani Scholars in the etiopathogenesis of quruh, who states that hararat & ratubat are an essential component of ufunat which forms an inflammatory swelling and when it get secondarily infected, it results in rupture of this swelling which in turn leads to ulcer formation.10,36.
Vaginal discharge
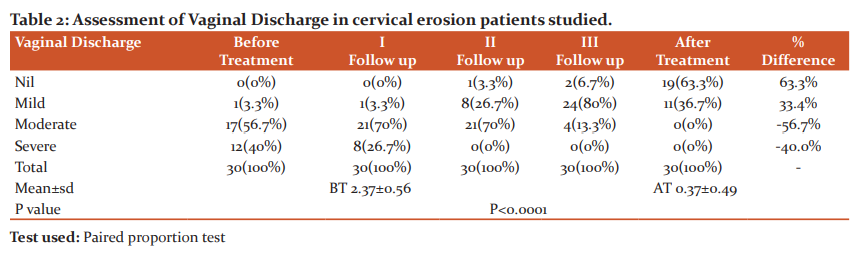
At baseline, all patients were complaining of vaginal discharge. During treatment, on 1st& 2nd follow up, it persists in 96.3% and was absent in 3.3% patients respectively. After treatment, it persists in 36.7% with mild discharge. & was absent in 63.3%.At baseline, vaginal discharge was mild, moderate & severe in 3.3%, 56.7% & 40% patients respectively. During treatment, on 1st follow up vaginal discharge was mild & moderate and severe in 3.3%, 70% and 26.7% patients respectively, whereas none of the patients had severe vaginal discharge; on 2nd follow up, the vaginal discharge was not present in 3.3% and 26.7% and 70% patients had mild and moderate vaginal discharge respectively. After treatment, the vaginal discharge was mild in 36.7% & absent in 63.3% of patients, though no patient had a moderate and severe vaginal discharge. After treatment, vaginal discharge with mean of 2.37±0.57 and 0.367±0.49 before and after intervention with P<0.001, considered as highly significant, which is consistent with the study of Gupta P et al.,37 Monroy OL38 & Anees S, 39 studies who reported vaginal discharge in 100% patients before treatment and relief in 86.6% after treatment. Cekmez Y et al.29reported vaginal discharge in 91.9% of patients with complete relief in 89.5%. Kamini D3 reported 93.45% and Hashmi S et al.24reported 100% improvement in vaginal discharge. Moreover, research drug possesses muhallilewaram, Daffi-i- tafun, anti-microbial, anti-fungal, anti-viral activities, which might resolve the inflammation after removing the infection and thus improves the vaginal discharge (Table.2).14,16,17,19,40-43
Low backache
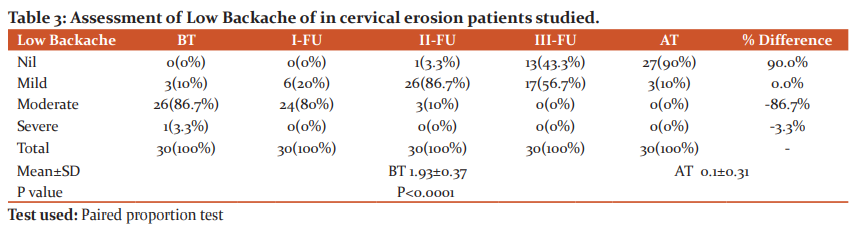
After treatment, compared to baseline low backache was relieved in 90% of patients with a mean of 1.93±0.37 and 0.1±0.36 before and after intervention respectively, with P<0.0001 considered as highly significant. Anees S 39reported 100% patient’s with complaining of low back pain and relief in 66.7%. Mirza S et al.25 reported 53.3%, Hashmi S et al.24 reported 30%, Kamini D3 reported 64 %, and Al-Kaseer et al.28 reported 65% improvement in low backache. low backache at baseline, after treatment was nil, mild, moderate, and severe, ie 90%, 10%,0%,0% respectively with P<0.001, considered as highly significant, which is following the studies of Kamini D et al.3 reported1.26±0.4 and 0.46±0.4, Sharma P et al.44reported 1.90±0.60 and 0.95±0.60 & Gautam A et al.31reported 1.12±0.169and 0.75±0.619 as Mean ±SD of low backache before and after treatment. Moreover, research drug possess muhallilewaram, musakkin, anti-inflammatory, analgesic, sedative activities which might resolve the inflammation and hence improves low backache (Table 3)14,16,17,19,40-43
 Dyspareunia
Dyspareunia
The Unani formulation was most successful in managing white discharge as all 30 patients presenting with vaginal discharge were having no discharge after the treatment. Other associated symptoms of cervicitis like low backache, lower abdominal pain, and dyspareunia were significantly relieved. Pharmacological studies reported that methi, alsi, babuna, nakhunaand karamkalla12 are proved for antimicrobial effect that may have inhibit the growth of organism and also these drugs are having anti-inflammatory property.,18,40,45 The improvement in these symptoms is most probably because of the effect of the test drugs having musaffikhoon, muhallil, dafetaffun, qabiz, mujaffifqurooh properties and baridwayabismizaj.46 As discussed earlier in etio-pathogenesis zoefequwateghazia is one of the main causes of saylanurrahim that leads to this disease and baridwayabismizaj of drugs tone up the quwateghazia of rahim10 and thereby rectifying the quality and quantity of khilte dam. Further, astringent drugs have been reported to decrease the secretions, which may have an inhibitory effect.
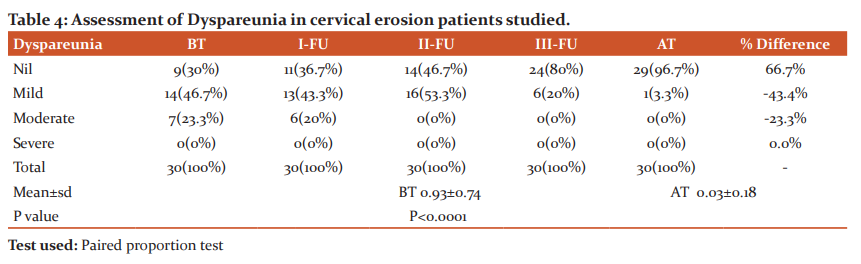
Table 4 shows dyspareunia in 70% of patients with mild and moderate 46.7% and 23.4% respectively. Whereas 30% of patients are free of dyspareunia. In the first follow-up of treatment, 36.7% are free with dyspareunia in mild and 20%in moderate dyspareunia patients. Whereas in second follow up 46.7% of patients were free of dyspareunia whereas 53.3% were having mild dyspareunia. Whereas in third follow up it is improved to 80% with dyspareunia free and 20% with mild Dyspareunia. The mean is 0.93±0.734and 0.03±0.18 before and after treatment respectively with p<0.0001 which is highly significant. After treatment, 96.7% of patients are free of this symptom with a % difference of 66.7, and 3.3% with mild dyspareunia with a% difference of -43.4.
Contact bleeding
In this study out of 30 patients, 25(83.4%) had contact bleeding. with mild in 14(46.7%), moderate in 9(30%) and severe in 2(6.7%) patients. In first follow up of treatment one severe case of contact bleeding responded well. Whereas in second follow up 43.3% are free of contact bleeding. Whereas 46.7% had a mild type and 6.7% had moderate and 3.3% has severe contact bleeding. In third follow up 70% got relieved totally from contact bleeding and only 26.7% had mild contact bleeding and 3.3% had moderate bleeding in patients of cervical erosion. The mean is 1.27±0.83 and 0.03±0.18 before and after intervention with p<0.0001 which is highly significant. After treatment, 96.7% of patients are free of contact bleeding and 3.3 % with mild contact bleeding. This show the effect of abzan of Unani formulation as mentioned in Unani literature (Table 5).
 Cervical ectopy grading: At baseline, cervical ectopy was observed in 100% patients, which remains in 43.3% of patients after treatment. Cervical ectopy was in grade I in 40% patients, grade II in 50% & grade III in 10%; during treatment, After treatment, on 1st follow up, 40% patients had cervical ectopy in grade I, 3.3% in grade II and none of the patient had cervical ectopy in grade III; Thus, cervical ectopy was reduced in 43.3% and cured in 56.7% patients with P=0.0054, considered as highly significant. The mean is 1.7±0.66 and 0.47±0.58 before and after intervention with p<0.0001 which is highly significant. Shivana S et al.30reported healing of cervical ectopy in 60% patients after 7 days, 30% after 14 days and 10% after 21 days of treatment. Sharma P et al.44reported improvement in 65.85% patients, Cekmez Y et al.29reported in 95.9% patients after 6weeks. Gautam A et al31reported improvement in 53.4%patientsafter 7days. Hence, complete healing of cervical ectopy as observed in 20% patients only after 2 weeks of treatment. Moreover, research drug possesses mussakin, muhallil- i- auram mullayan, mujaffif, mudammillequruh, qabid, antiulcer, antioxidant & wound healing activities, which might be helpful in the healing of cervical erosion (Table 6).14,16,17,19,40-43.
Cervical ectopy grading: At baseline, cervical ectopy was observed in 100% patients, which remains in 43.3% of patients after treatment. Cervical ectopy was in grade I in 40% patients, grade II in 50% & grade III in 10%; during treatment, After treatment, on 1st follow up, 40% patients had cervical ectopy in grade I, 3.3% in grade II and none of the patient had cervical ectopy in grade III; Thus, cervical ectopy was reduced in 43.3% and cured in 56.7% patients with P=0.0054, considered as highly significant. The mean is 1.7±0.66 and 0.47±0.58 before and after intervention with p<0.0001 which is highly significant. Shivana S et al.30reported healing of cervical ectopy in 60% patients after 7 days, 30% after 14 days and 10% after 21 days of treatment. Sharma P et al.44reported improvement in 65.85% patients, Cekmez Y et al.29reported in 95.9% patients after 6weeks. Gautam A et al31reported improvement in 53.4%patientsafter 7days. Hence, complete healing of cervical ectopy as observed in 20% patients only after 2 weeks of treatment. Moreover, research drug possesses mussakin, muhallil- i- auram mullayan, mujaffif, mudammillequruh, qabid, antiulcer, antioxidant & wound healing activities, which might be helpful in the healing of cervical erosion (Table 6).14,16,17,19,40-43.
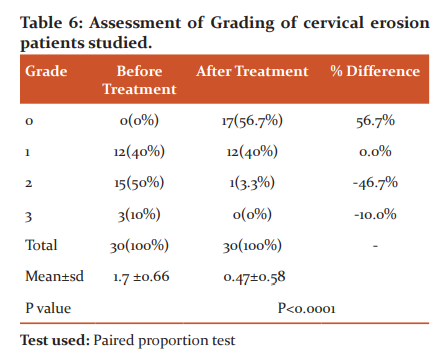
Interpretation: significantly decrease in cervical erosion Grading after treatment.
QOL by SF-12 score: Cervical erosion with its symptoms has a broad impact on HRQoL and puts a heavy economic burden on society.47 The mean± SD before the intervention was 382.73± 52.33 and after it was 910.17±56.30 with mean difference 0f 910.17 and p-value <0.0001. It shows strongly significant improvement in the quality of life (Table 7).
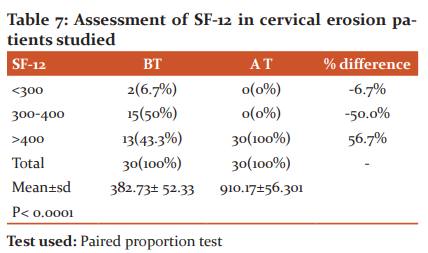
Interpreatation: Significant improvement in Quality of life as assessed by SF-12.
Primary outcome measures
Vaginal discharge: the mean of vaginal discharge before and after treatment is 2.37±0.57and 0.37±0.49 respectively with a P<0001. Improvement in vaginal discharge was noted in 90% patients; while it persists in 10% patients after 2 weeks of treatment; Anees S31 reported 86.6% after 1 week, Jindal M 2 reported 100% and 92% in two groups after 4-6weeks of treatment (Table 8).
Low backache: The mean± sd of low backache before the intervention was 1.93±0.37and after it was 0.1±0.36 with mean difference 0f 90.0% and p-value <0.0001. Absence of low backache was noted in 90% patients, where it was in mild in 10% of patients after 3 weeks of treatment, which correlates with the study of Jindal M 2 reported relief in 96% & 76% in two groups after 4-6weeks of treatment (Table 3).
Dyspareunia
The mean is 0.93±0.74and 0.03±0.18 before and after treatment respectively with p<0.0001 which is highly significant. This study shows dyspareunia is absent in the 96.7% of patients with mild in 3.3%. In the first follow-up of treatment, 36.7% are free with dyspareunia 43.3 in mild and 20%in moderate had dyspareunia. Whereas in second follow up 46.7% of patients were free of dyspareunia whereas 53.3% were having only mild dyspareunia. In third follow up in80% were dyspareunia free and 20% with mild Dyspareunia. After treatment, 96.7% of patients are free of this symptom with a % difference of 66.7, and 3.3% with mild dyspareunia with a% difference of -43.4. It shows that Unani formulation having muhallileawram, jail, mussakinealam etc. properties helps in relieving pain.
Contact bleeding
The mean is 1.27±0.83 and 0.03±0.18 before and after intervention with p<0.0001 which is highly significant. In this study patient with contact bleeding, mild in 14(46.7%), moderate in 9(30%) and severe in 2(6.7%) patients. In first follow up of treatment one severe case of contact bleeding responded well. In the second follow up43.3% are free of contact bleeding. Whereas 46.7% had a mild type and 6.7% had moderate and 3.3% has severe contact bleeding. In third follow up 70% got relieved totally from contact bleeding and only 26.7% had mild contact bleeding and 3.3% had moderate bleeding. After treatment, 96.7% of patients are free of contact bleeding and 3.3 % are with mild contact bleeding with % difference of 80.0%. This show the effect of abzan of Unani formulation as mentioned in Unani literature.
Hence, marked improvement in outcome measures with just 3 weeks of intervention with research Unani formulation as the topical application was due to the effect of research drug which possesses muhallilewaram, mujaffif, mudammilequruh, dafi-i-ta’ffun, qabid, musakkin, 12,13,14,15,16,17 properties. Moreover, pharmacological studies show that research drug exhibit antimicrobial, anti-inflammatory, antioxidant, anti-cancer, anti-ulcer, analgesic, hepato protective wound healing activities.13,14,18,19,20 Further methi, alsi, nakhoona, baboona, karamkalla contains flavonoids, saponins (glycosides), alkaloids (terpenoids, steroids) arachidonic acid, ethanol, histamine, leukotriens, polysaccharides, saponins (glycosides), carbohydrates, tannins, triglisoral etc,13,14 which are considered as the active principle of anti-ulcer activity. Flavonoids are a group of a polyphenolic compound having anti-ulcerogenic, anti-inflammatory, anti-bacterial, antioxidants properties4 which provide strength to the mucosal barrier & promote the ulcer to heal fast.21 The wound healing activity of Unani formulation as abzan might protect against microbial invasion by providing better tissue formation. Further, it enhances the rate of wound healing & tissue epithelization.4
Thus, research unani formulation was effective in the healing of cervical ectopy and relieving the associated symptoms. Moreover, a significant improvement would be expected if the duration of treatment was at least 6-8 weeks. Hence, it can be inferred that research Unani formulation shows potent wound healing action, the recovery of the wound might be due to the presence of chemical constituents which might favour wound healing action. Hence, it serves as an effective alternative in patients with cervical ectopy, particularly in those patients who are either not willing for cryotherapy or in whom cryotherapy is contraindicated.
Complete healing of cervical ectopy was observed in56.7% patients & no improvement in 43.3% patients after 3 weeks of treatment. The mean is 1.7±0.65 and 0.47±0.58 before and after intervention with p<0.0001 which is highly significant. Hashmi S et al.24 reported cure in 26.66% patients after 9 weeks of treatment. Shivanna et al.30 reported in 60% patients after 1week and in 40% after 3 weeks of local application of albothyl solution. Jindal et al.2 reported 92% & 76% respectively in two groups (electrocautery/ cryocautery) after 4-6weeks. Cekmez et al.29reported in 95.9 % of patients after 6 weeks of cryocautery.
The eight domains of SF-12 measures are as follows: physical functioning role: role limitations due to physical health, role limitation due to emotional problems, energy /fatigue, emotional wellbeing social functioning, pain general health.47 The mean± sd before the intervention was 382.73± 52.33 and after it was 910.17±56.30 with mean difference of 910.17 (p<0.0001). It shows strongly significant improvement in the quality of life. Cervical erosion with its symptoms has a broad impact on HRQoL and puts a heavy economic burden on society (Table 7). Hence the Unani formulation makes a strongly significant change in SF-12 score hence improvement in the quality of life.
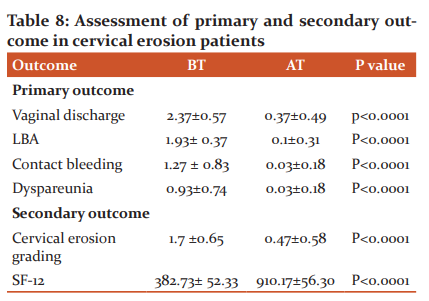
Interpretation; significant reduction in primary and secondary outcome parameters.
Strength of the study: This study was first of its kind; where treatment was given as abzan form which directly affects the eroded cervical area.
Limitations of the study: Small sample size, short duration of intervention, short follow up, colposcopy was not done during the study.
Future recommendation:
-
Use of research unani formulation as abzan for a longer duration (6-8 weeks) on the large number of patients with long follow up for better therapeutic outcome.
-
To conduct RCT’s with abzan of research formulation with standard treatment i.e.r electrocautery or cryo cautery.
-
References:
-
Kumari R.C, Singh BK. Role of Udumbaradi Tail in the management of a vaginal discharge due to Cervical erosion: A case report. Int J Res Ayur Pharm 2013; 4(4) 631-33.
-
Jindal M, Kaur S, Sharma S, Gupta KB, Pandotra P. What is better: cryocautery or electrocautery for cervical erosion? Int J Reprod Contracept Obstet Gynecol 2014; 3(3):715-19.
-
Kamini D, Meena.P. Kampillakadighrita in Garbhashaya Greeva Gata Vrana (Cervical Erosion). IJARP 2012;3(2):203-09.
-
SolankiSK,Sharma S. Role of Kshara Karma in the Management of Cervical Erosion. Ayu Ayur Phram Int J Alli Sci 2016;5(6):77-82.
-
Kartik K,Venkatesh , Uvin S. Assessing the relationship between cervical ectopy and HIV susceptibility: implications for HIV prevention in women. Am J Reproduct Immunol 2013; 69:68-73.
-
Yogesh M, Hetal B, Shachi P. Effect of Udumber-Sar in GarbhashayaGrivamukhagataVrana (Cervical erosion)- A case study. Int J Appl Ayur Res 2017 Oct;3(4):781-84.
-
D.C.Dutta. Text Book of Gynecology 7th Edn. New Delhi: Jaypee Brothers Medical Publishers(P)LTD ;2016. Pg. 217-218.
-
Khan A. Al Akseer (Urdu trans. by Kabeeruddin). 1sted. New Delhi: Idarae Kitabul Shifa; 2011:788-90.
-
Razi ABZ. Al HawiFilTib. Vol ΙΧ. New Delhi: CCRUM; 2001:10,12,24,25,36,42 ,47,50,
-
IbnSina. Al QanoonFilTib (Urdu trans. by Kantoori GH).Vol ΙΙΙ. New Delhi: Idarae Kitabul Shifa; 2010:1092,125-126.
-
Qamari MH. Ghana Mana. 1sted. New Delhi: Markazi Council Barai Tehqeeq Tibbe Unani; 2008: 414-415.
-
Halim MA. MufradateAzizi. New Delhi: Central Councill Research for Unani Medicine, 2009. p.49.
-
Swaroop A, Jaipuriar AS, Gupta SK, Bagchi M, Kumar P, Preuss HG, Bagchi D. Efficacy of a novel fenugreek seed extract (Trigonellafoenum-graecum, Furocyst TM) in polycystic ovary syndrome (PCOS). Int J Med Sci 2015; 12 (10): 825.
-
Umer KH, Zeenat F, Ahmad W, Ahmad I, Khan AV. Therapeutics, phytochemistry and pharmacology of Alsi (Linumusitatissimum Linn): An important Unani drug. J Pharmacog Phytochem 2017; 6 (5):377-83.
-
Khan ZJ, Khan NA, Naseem I, Nami SA. Therapeutics, phytochemistry and pharmacology of Tukhm-e-Katan (Linumusitatissimum L.). Int J Adv Pharm Med Bioallied Sci 2017 Mar; V. 2017(2017):1-
-
Rashid N, Dar PA, Ahmad HN, Rather SA. Alsi (Linum Usitatissimum (Linn.): A potential multifaceted Unani drug. J Pharmacog Phytochem 2018; 7(5):3294-300.
-
Hakim A. Tajudlin. Ahmed G. Jahan N. Evaluation of anti-infllammatory activity of the pods of iklil-ul-Malik (Astraogalushamosus. Linn). Indian J Nat Prod Reso 2010; (I): 34-37.
-
Jabeen A, Khan AA, Alam T, Maaz M, Mohmad SH. Flaxseed/Tukhm-e-katan (Linum Usitatissimum Linn): A Review. J Pharm Sci Innov 2014 oct;3(5):401-09.
-
Umer KH, Zeenat F, Ahmed W, Khan VK, Theraputics phytochemistry and pharmacology of Iklilul Malik (Astragalus hamosus Linn) A natural unani remedy. Int J Herb Med 2017 May;5: 1-4.
-
Khan MA. Asmaul Advia (Edited hy S. Z. Rehman). Aligarh: Publication Division. AMU: 2002:45
-
Gur CS, Onbasilar I, Atilla P, Genc R, Cakar N, Gurhan ID et al. In vitro growth stimulatory and in vivo wound healing studies on cycloartane-type saponins of Astragalus genus. J Ethnopharmacol 2011;134: 844-50.
-
Bernard Rosner (2000), Fundamentals of Biostatistics, 5th Edition, Duxbury, page 80-240
-
Suresh K.P, Chandrasekhar S. Sample Size estimation and Power analysis for Clinical research studies. J Human Reproduction Sci 2012;5(1): 7-13.
-
Hashmi S, Begum W, Sultana A. Efficacy of Sphaeranthusindicus and cream of Lawsoniainermis in cervical erosion with cervicitis. Eur J Integr Med 2011Aug; 3: 183-85.
-
Mirza S, Naaz SA, Alim SM, Rahman A. Analgesic, anti-inflammatory and anti-microbial activities of Irsa (Irisensata): A clinical study on the patients of Iltehabe Unqur-Reham (Cervicitis). IJPPR 2015; 3(4): 66-72.
-
Patil P, Sharma P. Colposcopic evaluation of cervical erosion in symptomatic women. Int J Reproad Contracept Obstet Gynecol 2017 jun; 6(6): 2207-11.
-
Latafat T, Siddiqui MMH, Jafri SAH. A Clinical study of Marham dakhlion on chronic cervicitis and cervical erosion. Ancient Sci life. 1992;11(3-4):158-62.
-
Al-Kaseer EA. Epidemiological characteristics of women with cervical erosion in Al-Sader city, Baghdad, Iraq. J Fac Med Baghdad 2010; 52(2): 157-58.
-
Cekmez Y, Sanlikan F, Gocmen A, Vural A, Turkmen SB. Is cryotherapy friend or foe for symptomatic cervical ectopy. Med Princ Prac 2016;25: 8-11.
-
Shivanna BS, Shivanna L, Kulkarni P. Comparative study of the efficacy of cryosurgery and Albothyl® solution in the management of cervical erosion in a rural hospital. J Dental Med Sci 2014 Sep;13 (9):106-09.
-
Gautam A, Rajan S, Rajan S, Sharma E. A clinical study of Kusthadi Varti in Karnini Yonivyapada w.s.r. to cervical erosion. Int J Curr Res 2017; 9(12): 62140-143.
-
Bangal VB, Patil NA, Gavhane SP, Shinde KK. Colposcopy guided management of cervical erosions in Rural population. Sch J App Med Sci 2014; 2 (1):261-65.
-
Koteswari M, Rao N, Renuka IV, Devi CP. A study of Pap smear examination in women complaining of leucorrhea. IOSR-JDMS 2015; 14(1/IV): 37-42.
-
Zulkifle M, Ansari AAH, Shakir M, Kamal Z, Alam T. Management of non-healing leg ulcers in Unani system of medicine. Int Wound J 2012; 366-72.
-
Qadry JS. Pharmacognosy. 16thed. New Delhi: JS. Offset Printers; 2014: 170.
-
Ibn Rushd. Kitabul Kullyat. (Urdu trans.). New Delhi: CCRUM; 1980. p.79- 81. 84-5,286,304-310.
-
Gupta P, Sharma S. Clinical evaluation of the efficacy of Kashara Karma with ApamargaKashara and Jyatyaditailapichu in the management of cervical erosion (Karniniyonivyavada). WJCPMT 2015; 1(3): 43-49.
-
Monroy OL, Aguilar C, Lizano M, Talonia FC, Cruz RM, Zavaleta LR. Prevalanceof human papillomavirus genotypes and mucosal IgA anti-viral responses in women with cervical ectopy. J Clin Vir 2010; 47:43-48.
-
Anees S, Mustafa S. Clinical study for the efficacy of Unani formulation in the management of vaginal discharge associated with cervicitis (Iltehabe unqurrehm). IABCR 2017; 3(4): 127-29.
-
Tanvir A, Izharul H, Aisha P, Nazamuddin M, Shaista P. Hulba (Trigonella foenum graecum): The common Indian spice full of medicinal values. Int J Preclin Pharm Res 2014; 5 (1):41- 6.
-
Anju. Idris M. Methi (Trigonella fenum graceum): A Multifunctional Herbal Drug. JHMR 2018; 3:1-8.
-
Dharajiya D, Jasani H, Khatrani T, Kapuria M, Pachchigar K, Patel P. Evaluation of antibacterial and antifungal activity of fenugreek (Trigonella foenum graecum) extracts. Int J Pharm Pharm Sci 2016; 8(4): 212-17.
-
Miraj S, Alesaidi S. A systemic review study of the therapeutic effects of Matricaria Recutita chamomile (chamomile ). Electr Physic 2016 sep;8(9):3024
-
Sharma P, Sharma S, Nariyal V. A clinical study to evaluate the efficacy of Snuhi Kshara and Dhatakyadi Tail Pichu in the management of Karnini Yonivyapadw. s.r to cervical erosion. Int Ayur Med J 2016; 4 (9): 2793-98.
-
Hussain SM. Herbal Unani Medicine all India; Unani Tibbi Conference New Delhi 53
-
Kabeeruddin M. Makhzanul Mufradat. New Delhi. Aijaz publication house: 2007.
-
Larson CO, Schlundt D, Patel K, Hargreaves M, Beard K. Validity of the SF-12 for use in a low-income African American community-based research initiative (REACH 2010). Prev Dis Public Health Res Pract Pol 2008; 5 2(2): 01-11.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





