IJCRR - 8(4), February, 2016
Pages: 13-18
Date of Publication: 21-Feb-2016
Print Article
Download XML Download PDF
HISTOMORPHOLOGICAL SPECTRUM OF SKIN ADNEXAL TUMORS AT A TERTIARY CARE HOSPITAL - A RETROSPECTIVE STUDY
Author: Nirali Amin, Smita Shah, Shreedhan Prajapati, Hansa Goswami
Category: Healthcare
Abstract:Background: Skin adnexal tumors (SAT) are a large and diverse group of benign and malignant tumors which exhibit morphological differentiation towards one of the different types of adnexal epithelium present in normal skin: pilosebaeceous unit, eccrine and apocrine. The aim of this study was to recognize various histomorphology of skin adnexal tumors, their frequency, age and site distribution. Methods: It was a retrospective study of 50 cases of skin adnexal turmors, diagnosed on histopathological examination over a period of 3 years (January 2012 to December 2014) in the Department of Pathology, B.J. Medical college, Ahmedabad. Histopathological examination was done on Formalin fixed, Paraffin embedded tissue sections stained with Haematoxylin and Eosin. Special histochemical stains like PAS stain and Reticulin stain were also used, wherever required. Results: Skin adnexal tumors were most common in the age group of 31 to 40 years (38%, 19/50). Male to female ratio was 1:1.27. The head and neck region was the most common site affected (60%) with 32% cases located on the face. 98% cases were benign and only a single case (2%) was malignant. The sweat gland tumors formed the largest group involving 70% of cases followed by hair follicle tumors followed by sebaceous gland tumors. Nodular hidradenoma was the most common benign tumor. Sebaceous carcinoma was the only malignant adnexal tumor reported in our study. Conclusion: Skin adnexal tumors are relatively rare. Benign adnexal tumors are far more common than their malignant counterparts. There is slight Female preponderance. Face is the commonest site for occurrence of SATs. Nodular hidradenoma is the most frequently encountered tumor among all SATs. Histopathological examination is mandatory in their diagnosis as they have very wide spectrum and frequency of differentiation along different lines in the same lesion.
Keywords: Skin adnexal tumor, Nodular hidradenoma, Sebaceous carcinoma, PAS stain
Full Text:
INTRODUCTION Skin adnexal tumors (SAT) are a large and diverse group of benign and malignant neoplasms which exhibit morphological differentiation towards one of the three different types of adnexal epithelium present in normal skin: pilosebaeceous unit, eccrine and apocrine [1]. SAT may display more than one line of differentiation (hybrid/composite tumors), rendering precise classification of these neoplasms difficult [1]. These tumors are derived from multipotential undifferentiated cells present within the epidermis or its appendgeal structures.
Adnexal tumors arising from the skin are usually missed clinically as most of the SATs present as asymptomatic papules or nodules. Anatomic location, number and distribution of lesions provide important clue but histopathology is invaluable in confirmation of the diagnosis. Diagnosis of skin adnexal tumors is possible by performing an elliptical skin biopsy, submitting for haematoxylin and eosin (HandE) staining and histochemistry.
Most SAT are benign, but a malignant counterpart of every SAT has been described [1]. Malignant skin adnexal tumors are rare, locally aggressive and have the potential for nodal involvement and distant metastasis with a poor clinical outcome. Therefore establishing a diagnosis of malignancy in SAT is important for therapeutic and prognostic purposes [1]. The aim of the current study was to recognize various histomorphology of skin adnexal tumors, their frequency, age and site distribution.
MATERIALS AND METHODS The data for this retrospective study was obtained from Department of Pathology of a tertiary care hospital, from January 2012 to December 2014. The tumors were subjected to meticulous gross and microscopic examination. The histopathological examination was done on formalin fixed paraffin embedded tissues. Haematoxylin and Eosin stained sections were examined and few special stains like PAS and reticulin were performed wherever required. Age and gender prevalence, comparison of clinical diagnosis, site of involvement with biopsy diagnosis were done.
RESULTS During the study period, 50 adnexal tumors of skin were diagnosed on histopathological examination (Table 1). Benign adnexal tumors constituted 98% (49/50) cases and only one case of malignant adnexal tumor (2%) was noted. In the present study, skin adnexal tumors were observed in all age groups ranging from 3 to 80 years (Table 2). However, the highest incidence was observed in the age group of 31-40 years followed by age groups 11-20 years and 41-50 years. The Male: Female ratio was 1:1.27. The head and neck region was the most common site affected followed by lower limb and upper limb (Table 3). In head and neck region, face was the most common site followed by scalp.
The neck region was least affected site. The sweat gland tumors formed the largest group involving 70% of cases followed by the hair follicle tumors, followed by sebaceous gland tumors. Amongst the benign tumors, nodular hidradenoma was the most common tumor representing 16% of all cases. A single case of Sebaceous carcinoma was the only malignant adnexal tumor reported in our study.
Benign tumors were observed in age ranging from 3-80 years and a single case of sebaceous carcinoma was noted in a person at 42 years of age. Sweat gland tumors were all benign and included nodular hidradenoma, chondroid syringoma, eccrine spiradenoma, syringocystadenoma papilliferum, eccrine poroma, hidradenoma papilliferum, syringoma, cylindroma, tubular adenoma and ceruminous adenoma.
Among 3 sebaceous gland tumors, 2 were benign and the remaining one was malignant. Sebaceous naevus was the only benign lesion encountered in this study. Sebaceous carcinoma was seen in 1(2%) patient. All hair follicle tumors in this study were benign and included trichofolliculoma, trichoepithelioma, pilomatrixoma and proliferating trichelemmal tumor. Comparison of observations from the present study and other published studies is shown in Table 4.
DISCUSSION Adnexal tumors of the skin, though rare have been recognised from the later part of 19th century [4]. We also observed that adnexal tumors of skin appear to be relatively uncommon tumors. They are thought to have a genetic basis. Mendelian inheritance and P53 mutations are important contributing factors [3]. The histogenesis of these tumors are from either primary epithelial germ cells or pluripotential cells or cells of pre-existing structure [5]. Skin adnexal tumors have a wide range of age distribution. In our study, commonest age group was 31-40 years and Male: Female ratio was found to be 1:1.27; Head and neck region was the most common site of occurrence.
All these findings were consistent with the results with the study by Radhika et al [5]. Incidence of benign tumors was more as compared to malignant cases. This finding was consistent with other studies. Benign tumors showed smooth borders, absence of ulcers, presence of adnexae and absence of necrosis. The occurrence of benign tumors in our study was 98% and 2% (Only one case) was malignant. Nair et al observed that tumors of sweat gland differentiation were most common followed by hair follicle tumors and then sebaceous glands tumors [6].
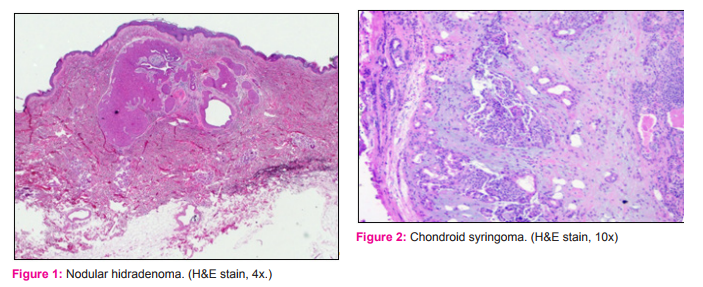
The present study showed similar results with sweat gland tumors constituting the largest group (70%), followed by hair follicle tumors (24%) and sebaceous gland tumors (6%). Nodular hidradenoma (Figure 1) was the most frequently encountered benign sweat gland tumor in the present study. Similar observations were reported by Radhika et al [5]. Histopathologically most of these tumors are circumscribed and solid with few showing cystic change. Tumor is composed of varying sizes of tubules and papillary projections lined by inner cuboidal and outer myeoepithelial cell layer. Solid portions of the tumor show nodules comprised of clear and polygonal cells [2].
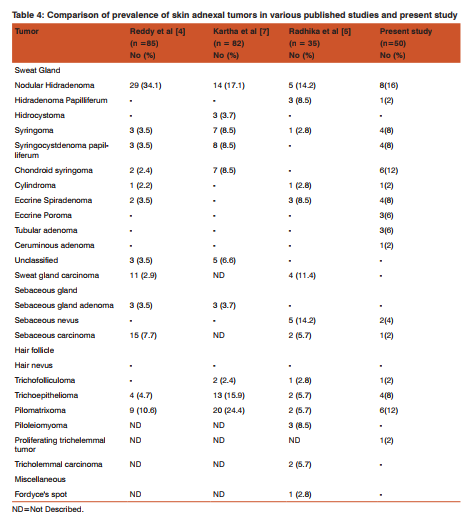
Chondroid syringomas usually present as well circumscribed lobulated masses centered in deep dermis or subcutaneous fat, with prominent chondroid or myxoid stroma, tubulo-alveolar structures lined by epithelial- myoepithelial cell bilayer, ducts lined by single layer of epithelium, nests of polygonal cells and sometimes keratinous cysts. (Figure 2) Syringomas are characterized histologically by interweaving nests, cords and small cysts that are located in the upper half of the dermis. They are enmeshed in a dense collagenous stroma without any epidermal contact.
The ducts of syringoma are composed of 1- 2 layers of cuboidal cells rarely showing clear cell change. Tadpole appearance is quite common in syringoma (Figure 3). Syringocystadenoma papilliferum (Figure 4) is a rare adnexal neoplasm. We observed 4 cases in our study. Microscopically there are papillary projections with squamous epithelial lining and ductal invaginations. These ductal structures are lined by inner columnar and outer cuboidal cells [2]. Cylindroma (Figure 5), Hidradenoma papilliferum (Figure 6) and Ceruminous adenoma were the least common sweat gland tumors in the present study accounting for single case of each. Cylindroma is a benign basaloid tumor that has a mosaic architecture.
They are solitary or multiple. Histologically these are circumscribed non encapsulated dermal nodules composed of islands and cords of basaloid cells surrounded by a thick hyalinized, Periodic acid-Schiff (PAS) positive basement membrane. Not a single case of malignant sweat gland tumor was observed in the present study. Sebaceous naevus was the common sebaceous gland tumor observed by us. However this tumor was not documented in other published studies [4]. Sebaceous nevus histologically consists of zones of epidermal hyperplasia with small foci of sebaceous glands, miniature hairs and minimal numbers of ducts or glands.
In the present study we reported only one case of malignant adnexal tumor- sebaceous carcinoma. Microscopically, sebaceous carcinoma revealed irregular epithelial lobules with an infiltrative growth pattern in the dermis. Lesional cells demonstrated marked cytologic atypia, mitotic activity and focal sebaceous differentiation (Figure 7). In pilomatrixoma, the histopathological hallmark is that of basaloid lobules which are contiguous with eosinophilic ghost cells or shadow cells (Figure 8).
Dystrophic calcifications are usually present. Trichoepithelioma histologically is a symmetric lesion that contains a mixture of epithelial elements ranging from hair germs associated with capillary mesenchymal bodies to small horn cysts, to lace like reticular basaloid structures to mature hairs. Tricofolliculoma and Proliferating trichelemmal tumor were observed as single case of each in our study. Malignant hair follicle tumors were not observed in this study.
CONCLUSION We conclude that skin adnexal tumors are relatively rare. Benign adnexal tumors are far more common than their ma lignant counterparts. Sweat gland tumors are most common among all skin adnexal tumors. There is slight Female preponderance. Head and neck are frequent sites for occurrence of these tumors, among which face is the commonest site. Nodular hidradenoma is the most frequently encountered tumor among all skin adnexal tumors. Skin adnexal tumors cannot be diagnosed on clinical grounds only and histopathological diagnosis plays a major role in diagnosing these tumors.


References:
1. K O Alsaad, N AObaidat, D Ghazarain, Skin adnexal neoplasms-part 1: An approach to tumors of pilosebaceous unit, J Clin Pathol 2007; 60: 129:44
2. W Klein, E Chan, J T Seykora, Tumors of epidermal appendages,DE Elder (Ed) Lever’s Histopathology of the Skin9thedn. Philadelphia, PA: Lippincott Williams and Wilkins, 2005, 867-926.
3. Perez MI, Robins P, Biria S, Roco J, Siegel E, Pellicer A. P53 oncoprotein expression and gene mutations in some keratoacanthomas. Arch Dermatol 1997;133:189-93.
4. M K Reddy, A J Veliath, S Nagarajan, A L Aurora, A clinicopathological study of adnexal tumors of skin, Indian J Med Res 75, 1982, 882-9
5. K Radhika, B V Phaneendra, N Rukmangadha, M K Reddy A biopsy confirmed skin adnexal tumors: experience at a tertiary care teaching hospital, Journal of Scientific Research, 2, 2013, 132-138
6. P S Nair, A clinico-histopathological study of skin appendageal tumors, Indian Journal of Dermatology,Venerology and Leprology, 74 (550), 2008
7. Kartha CC, Shankar SK, Bhuyan UN. Benign mixed tumor of skin–a histopathologic study of 7 cases. Indian J Pathol Microbiol 1980;23:1-6
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





