IJCRR - 12(23), December, 2020
Pages: 152-155
Date of Publication: 07-Dec-2020
Print Article
Download XML Download PDF
A Zone of Minimal Conflict: \"The Neutral Zone\" \? Case Series with 6 Month Follow Up
Author: Akanksha N Bhandari, Nilesh S. Bulbule, Amit K Jagtap, Trunaya Bhatlekar, Amit Nandi, Shalu Mondal
Category: Healthcare
Abstract:Introduction: The procedure of recording zone of minimal conflict tries to make a mandibular denture which is created by muscular function as well as is in harmonious relation with the adjoining perioral musculature.
Aim: This article aims to describe the step-wise procedure followed in patients with resorbed mandibular edentulous ridges to construct complete denture by recording the neutral zone to enhance the stability of the mandibular denture.
Methods: Detailed intraoral examination of the patients was done and coupled with the use of correct impression materials and techniques to record primary and secondary impressions were done. Neutral zone recording was done and mandibular denture fabrication was done accordingly.
Results: Resorbed ridges make prosthetic rehabilitation difficult but can be made successful by proper planning and treatment approach. Close adaptability to basal seat contributes to improved stability which is emphasized by this technique by the use of a close-fitting tray and a viscous impression material. Secondary impression was made with elastomeric impression material to capture the details of the tissues. Though this technique is not a new one and also involves extra clinical steps, it is of significant value.
Conclusion: The mandibular dentures which are constructed utilising the philosophy of neutral zone showed improved stability in resorbed lower ridges.
Keywords: Neutral zone, Resorbed mandibular edentulous ridge, Impression, Complete denture, Stability, Perioral musculature
Full Text:
INTRODUCTION
Whenever there is the loss of teeth and rehabilitation is planned it should be done in a way that allows efficient and comfortable functioning as well as be in harmonious relationship with the stomatognathic system and the temporomandibular joint.1 Loss of teeth can lead to multifactorial changes in the mouth like alveolar ridge resorption, expansion of the tongue, and looseness of muscle tone of the face.2 In case of the resorbed mandibular alveolar ridge, dental implants can impart better stability of mandibular complete dentures; however, it is not always feasible to provide dental implants due to systemic conditions, economical background or patient’s psychological condition.1
Neuromuscular control is said to be the major criteria for providing stability in mandibular complete denture because the available area for support is far less as compared to the maxillary support area. A very significant role in the stability of mandibular complete denture is played by the size, position of prosthetic teeth as well as the contours of the polished surface as they are likely to be affected to impaired forces from the tongue, lips and cheeks if placed in objection with the functioning of these structures.3 So there exists a space in the oral cavity when all the existing teeth are not present which is known as the Neutral zone/Potential denture space/Dead space/Zone of minimal conflict/Zone of equilibrium.3,4 This Neural zone has been defined as the potential space between the lips and cheeks on one side, and the tongue on the other that area or position where the forces between the tongue and cheeks or lips are equal.5
This technique of recording zone of minimal conflict is favourable for patients with multitudinous, unstable, unretentive mandibular complete dentures. The objective of this procedure is to place the teeth in such a way that the forces exerted by the tongue and the cheek muscles are balanced and the teeth remain in a safe, protected zone where it is dictated by the oral musculature that may vary from one patient to another.6 This article attempts to represent a simple yet effective method to attain the above qualities of the denture by using simple chairside dental materials and techniques which can be practised by every dental clinician.
CASE-1
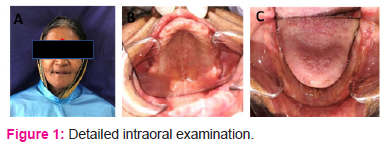
A female patient of age 55 came to the Department of Prosthodontics with a chief complaint regarding the inability to chew. She was completely edentulous since the past 7 years and detailed intraoral examination showed the presence of an atrophic edentulous mandibular ridge and moderately resorbed maxillary ridge (Figure 1).
Case 2
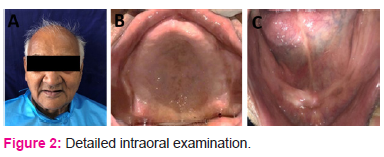
A male patient of age 70 years reported to the Department of Prosthodontics, with a chief complaint regarding chewing difficulty. He was completely edentulous since the past 11 years and the medical condition stated that he was diabetic and was on the medications for the same. The intraoral examination revealed that the patient had thin resorbed mandibular ridge (Figure2).
TREATMENT PLANNING
After the completely evaluating patient’s history, radiographs, and present clinical scenario different options of treatment were discussed with both the patients. They included pre-prosthetic surgeries such as bone augmentation and vestibulopathy for implant-supported overdenture and conventional complete denture. But, the patients were not keen to undergo any kind of surgical procedure and thus chose for a simple complete denture.
CLINICAL PROCEDURE
Preliminary impressions were made with impression compound for the edentulous upper arch and admix technique which used impression compound and green stick in the ratio of 3:7 by weight which was suggested by McCord and Tayson for edentulous mandibular arch 7 using a metal stock tray.(Figure 2A)
After disinfection of the impressions, the dental plaster was poured and primary casts were obtained.(Figure 2B)
Fabrication of custom impression tray using self-cure acrylic resin was done on preliminary casts and border moulding was done for mandibular ridge using All Green’s method using green stick compound8. A small amount of material was removed from the crest of the ridge to provide space for impression material during final impression technique. Application of tray adhesive was done and kept to dry for a while. Final impressions of the mandibular ridge were taken with light body polyvinylsiloxane(Figure 2C).
After disinfection of impressions; master casts were made using dental stone. (Figure 2D) Temporary denture bases were constructed using autopolymerising acrylic resin on the master cast. Followed by making occlusal rims of wax, jaw relation using tentative method & articulated (Figure 2E). After this procedure, new denture bases were made with acrylic stops in the molar region and the anterior region for moulding material while recording neutral zone (Figure 2F) at the same level of established vertical dimension.
The neutral zone recording for the mandibular ridge was done as follows. The mandibular temporary denture base along with the softened green stick was then placed in the mouth of the patient. This custom tray was adjusted to ensure that it was not overextended and also tried to maintain stability during the opening, swallowing, and speaking. The further patient was instructed to pronounce vowel sounds i.e. aaa, eee, ooo, talk, swallow, drink some water, sucking, smiling, licking the lips, whistling, and counting. The extra amount of compound was removed, followed by softening of material and placing back into the mouth of the patient and was asked to repeat the functional movements. After a few minutes, when the impression was set it was taken out from the patient’s mouth and reexamined.
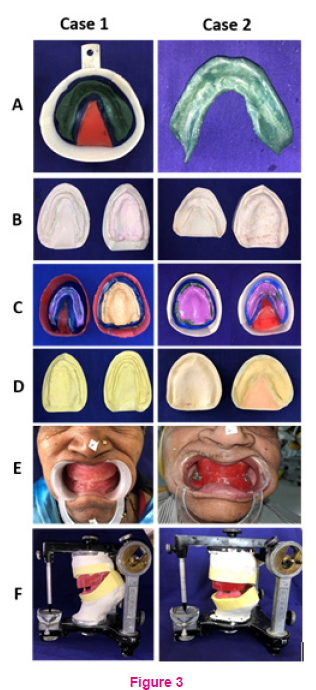
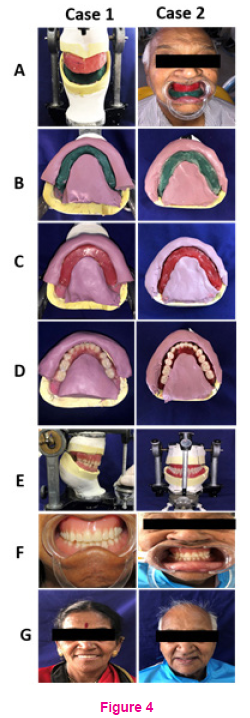
The internal and external groups of muscles of facial expression have been brought into action by this method. In doing so, reciprocal forces which act on the compound, will slowly mould it into a state of neutral balance and also become centrally still concerning all of the forces of complex nature which act on it (Figure 3A).
The impression of the neutral zone which was gained was then placed on the master model, cutting of location grooves was done on the model and then followed by covering with a putty index surrounding the impression on both the buccal and lingual sides (Figure 3B).
The denture base withholding the recorded neutral zone material was removed from the index, molten wax was allowed to flow to obtain wax rim according to the putty index and arrangement of prosthetic teeth was done following the same index (Figure 3C).
The prosthetic teeth were arranged within the matrices. Semi-anatomic teeth were chosen and the arrangement was done in laterally balanced occlusion scheme (Figure 3D). Nonanatomic teeth were chosen and arranged in monoplane articulation (Figure 3D). This was followed by checking of vertical dimension, centric relation, esthetics, and phonetics during wax denture try-in stage (Figure 3E).
After the try-in was considered to be satisfactory by the dentist, the dentures were processed, finished and inserted (Figure 3F).
Six months follow up was taken for both the patients and were evaluated for esthetic and phoneticevaluation,intraoral condition showed no mucosal changes and both patients were satisfied.
DISCUSSION
Creating secure and firm prosthesis is the ultimate aim for any clinician. Restoring the masticatory function and achieving esthetic satisfaction is cumbersome and difficult in cases having high degrees of ridge resorption. But this challenging condition is dealt with by meticulous attention to the small details and following the protocol properly. During this case, the preliminary impression was recorded using admix technique where impression compound and low fusing impression compound were mixed within the ratio of 3:7 by weight. By making use of low fusing green stick which has less compressibility of the tissues, better flow and handling characteristics it easier to record the details accurately.8
The border moulding was done by All Green’s method where the aim is to give maximum stability by covering maximum denture bearing area and selectively distributing the pressure over the complete denture bearing area. Firstly, the close contact of the custom tray tries to distribute maximum forces to the buccal shelf area. Second, the viscosity of the low fusing impression compound will try to remove any soft tissue folds as well as smoothen them over the lower jaw bone, thereby decreasing the possibility for decreased comfort which can arise from the “atrophic mucosal sandwiching” between the denture and the bone.9
This lower impression in the zone of minimal conflict was recorded so that the area where the denture may be placed is not subjected to unstrained destabilizing forces from the perioral musculature may be determined and so contributes to the stability of denture base.10 Arranging prosthetic teeth within the neutral zone helps us to attain two main points:
1. Artificial teeth don’t interfere with normal oral muscle function
2. Normal oral and peripheral structures may show muscular activity which may impart forces against the complete dentures and contribute to stability and retention of the prostheses.11
Recording neutral zone for the maxillary arch isn’t recommended as the amount of influence tongue has on maxillary dentures is relatively less than mandibular prosthesis with regards to stability. Also, the arrangement of the prosthetic lower teeth within this zone of minimal conflict guides to place the upper teeth within the same zone.10 Non-anatomic teeth chosen and articulated to monoplane occlusion scheme allowed the patient to clench in maximum intercuspation during functional, non-functional activities as well as assists in the stability of dentures.10
CONCLUSION
The philosophy of zone of minimal conflict is based on the factors that for every patient, there is a significant area within the denture space where the muscular function can allow proper seating of the denture and also forces which are created by the tongue are neutralized by the forces created by the perioral musculature.Thus this article describes a novel technique in managing patients with resorbed mandibular ridges by making potential use of this denture space area.
ACKNOWLEDGEMENT: The authors are grateful to the authors/editors/publishers of all those articles, journals, and books from where the literature for this article has been reviewed and discussed.
CONFLICT OF INTEREST: Nil
SOURCE OF FUNDING: Nil
References:
1.Kaira LS, Dabral E. Anthropoidal Pouch technique for highly resorbed ridges. NUJHS 2013;.3:128-31.
2.Asnani P, Chandu GS, Mishra SK. Neutral zone technique in complete denture- Case report. J App Dent Med Sci 2015;1(1):15-18.
3. Ahmad J. Neutral zone in complete dentures: systematic analysis of evidence and technique. Smile DentJ2011;6:8-12.
4. Beresin VE, Schiesser FJ.The neutral zone in complete dentures.The company, Saint 1973;1–150.
5.Ferro KJ. The glossary of prosthodontic terms, J Prosthet Dent 2017; 117:105-8.
6. Saravanakumar P, Thangarajan S, Mani U, Kumar VA. Improvised Neutral Zone Technique in a Completely Edentulous Patient with an Atrophic Mandibular Ridge and Neuromuscular Incoordination: A Clinical Tip. Cureus 2017; 9(4):1-12.
7. McCord JF, Tyson KW. A conservative prosthodontic option for the treatment of edentulous patients with atrophic (flat) mandibular ridges. Br Dent J1997;182:469-72.
8. Herekar M, Sethi M, Fernandes A, Kulkarni H.A physiologic impression technique for resorbed mandibular ridges. J Dent Allied Sci 2012; 2(2):80-82.
9. Daniel S, Daniel AY, Kurian N. A modified physiologic impression technique for atrophic mandibular ridges. J Health Res 2017;4: 204-8.
10. Manoj SS, Chitre V, Aras M. Management of Compromised Ridges: A Case Report. J Indian ProsthodontSoc 2011;11(2):125-9.
11.Beresin VE, Schiesser FJ. The neutral zone in complete dentures. J Prosthet Dent 1967;36(4):356–367.
12.Prasad A, Hegde C, Prasad DK.A Study To Evaluate And Compare Oral Stereognostic Ability And Oral Tactile Sensibility Of Satisfied And Dissatisfied Subjects Wearing Complete Denture Prosthesis.Int J CurrRes Rev2012;4(6):139-45.
13.Russell AF. The reciprocal lower complete denture. J Prosthet Dent 1959; 9:180–90.
14.Deepika K, Bhatnagar A, Singh A et al. Fabrication of complete dentures using neutral zone technique in a patient with severely resorbed alveolar ridges - a case report. Int J Health Sci Res 2018;8(4):227-232.
15.Barrenas L, Odman P. Myodynamic and conventional construction of complete dentures: a comparative study of comfort and function. J Oral Rehabil1989;16:457-65.
16.Alfano, Leupold. Using the neutral zone to obtain maxillomandibular relationship records for complete denture patients. J Prosthet Dent2001;85:621-3.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





