IJCRR - 8(6), March, 2016
Pages: 14-17
Date of Publication: 22-Mar-2016
Print Article
Download XML Download PDF
CORRELATION BETWEEN BMI AND ARTERIAL STIFFNESS IN MIDDLE AGED SUBJECTS
Author: Niruba R., T. Kannan Kumar, Subha K. C., Vijiyalakshmi
Category: Healthcare
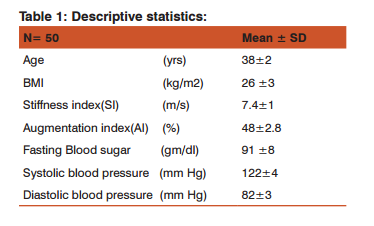
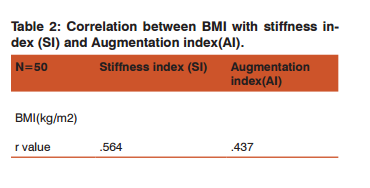
Abstract:Background: World wide prevalence of obesity has reached a pandemic proportion. Obesity and Arterial wall stiffness are independent predictors of cardiovascular diseases. We aimed to investigate how BMI affects arterial stiffness. Noninvasive method of measuring arterial stiffness can be applied to assess the elasticity of the vessel wall and reduce the cardiovascular morbidity. Study Design: Cross sectional observational study. Materials and Methods: Subjects n= 50 males, Age group 35-45 years. All participants had a sedentary life style, blood pressure and glycemic status were within normal limits. Subjects with history of peripheral vascular disease, smokers and any other illness that affects arterial compliance were excluded . Arterial stiffness was assessed from Augmentation index (AI) and stiffness index (SI). AI and SI was measured using IR1 model digital finger tip photo pulse plethysmograph. Results: Mean age = 38\?2 years, Mean BMI = 26\? 3, Mean Stiffness index = 7.4 \?1.4 m/s, Mean Augmentation index= 48 \?2.8 %.Pearson correlation was applied .BMI correlated positively with both augmentation index and stiffness index with r value is +0.437 and + 0.564 respectively. Conclusion: In our study both large and small artery stiffness were assessed. There was increase in arterial wall stiffness with increase in BMI. We conclude obesity affects arterial compliance, which might be the consequences of metabolic regulation, inflammatory pathways and other mechanisms
Keywords: BMI, Augmentation Index, Stiffness Index
Full Text:
INTRODUCTION In the present era, besides the genetic predisposition, adoption of sedentary lifestyle, lack of regular physical exercise, excessive intake of junk foods, stress of competitive world has made the environment conducive to the development of obesity (1). Obesity is associated with impaired function of the large arteries, which might be the consequence of metabolic regulation, inflammatory pathways, obstructive sleep apnoea or other mechanisms (2,3). Pulse wave analysis can measure stiffness index and augmentation index the surrogate markers of arterial stiffness (4).Thus Obesity and arterial wall stiffness are independent predictors for cardiovascular diseases. Thus correlating BMI and arterial stiffness can reduce the morbidity due to cardiovascular disease in overweight and obese individual. Aim: Assessment of vessel wall compliance among normotensive normoglycemic middle aged individuals and correlating it with their BMI. Study Design: Observational/cross sectional study.
MATERIALS AND METHODS: All participants gave a written informed consent to participate in this study. Institutional ethical committee clearance was obtained. Information details about sociodemographic characteristics, disease history, family history, alcohol consumption, cigarette smoking, drug intake and occupational history were obtained by a structured questionnaire. All participants had a sedentary lifestyle.
SUBJECTS Inclusion criteria: 50 healthy volunteers normoglycemic, normotensive males with no paternal or maternal history of diabetes, Age= 35- 45 yrs, Blood pressure = < 140/90 mmHg, Fasting blood sugar = 90-100 mg/dl.
Exclusion Criteria: Subjects with history of peripheral vascular disease, smokers, and any other illness that affects arterial compliance , subjects with family history of diabetes and hypertension were excluded from the study. Anthropometric measurements were taken. Height was measured using stadiometer and weight was measured using precalibrated weighing machine. Quetlet’s index was used to calculate Body mass index (weight/height in m2).Blood pressure was measured using a standard mercury sphygmomanometer. Fasting blood glucose was measured to rule out diabetic mellitus.
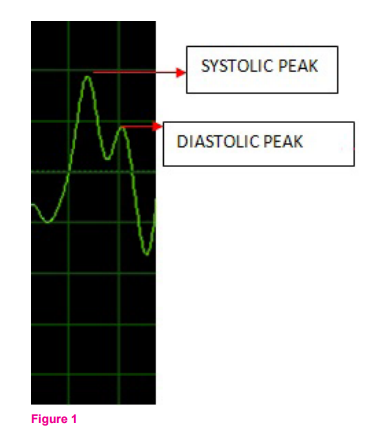
Recording of digital volume pulse (DVP): Digital volume pulse was recorded by in house built instrument IR1 model digital finger photoplethysmography (5). The signal from the instrument placed on the right index finger was digitalized by digital converter with a frequency of 100 Hz which was connected to the computer. DVP was analyzed by software virtual oscilloscope. Digital volume pulse contains 2 peaks: Fig-1 1. Systolic peak. 2. Diastolic peak. Initially Systolic peak is formed by pulse wave transmitted from the left ventricle to the finger directly.(5) Second peak or diastolic peak arises from pulse wave transmitted along the aorta to the small arteries in the lower body, from where they are again reflected along the aorta as a reflected wave (5) (fig-1).This path length is proportional to the subject’s height (h). Pulse transit time (PTT or ΔT) is the time interval between systolic peak and diastolic peak. It was measured by software image tool . Magnitude of systolic and diastolic peak were also measured .Stiffness index is based on the subjects height (6). Stiffness index and Reflective index were calculated by the following formulas.
Stiffness index (SIDVP) = Subject’s height (h).
Pulse transit time (ΔT).
Reflection index (RI) = Magnitude of diastolic peak (b) × 100.
Magnitude of systolic peak (a).
RESULT Statistical analysis was done Using SPSS Software version 16.0. The descriptive statistics of BMI, Blood sugar, Systolic blood pressure, Diastolic blood pressure are mentioned in table 1. Pearson correlation was applied. Correlation between BMI with stiffness index and reflective index was analyzed among study group and it showed a positive correlation with r value is +.564 and +.437 respectively (Table 2).
DISCUSSION Our study showed a positive correlation of BMI with stiffness index and reflective index. Indicating increased body weight affects the vessel wall compliance. Reduction of weight can improve the elasticity in vessels as stated in study by alvarez et al and Abate et al that after weight loss, the increased stiffness is reversed in parallel with reduction of heart rate which might be due to neural sympathetic over activity(7,8). Obesity is the risk factors for diabetes mellitus and cardiovascular disease, such as ischemic heart disease and stroke (9,10). Calculating body mass index (BMI) is the easiest way to evaluate overweight and obesity (9).
Non-invasive measurement of vascular wall elasticity is an important diagnostic tool which allows one to collect information on the functional status of the arteries and enables early detection of pathologies before the onset of clinical symptoms (11,12). Central blood pressure and measures of arterial stiffness have been shown to be powerful predictors of major cardiovascular events, independent of the traditional risk factors (13), The augmentation index (AI), gives us small artery stiffness (13), calculated from the difference between the first and second systolic peaks expressed as a percentage of the pulse pressure, and a measure of systemic stiffness(14) .
The stiffness index is a measure of pulse wave velocity (PWV) in large arteries. It is a measure of the timing of the diastolic relative to the systolic component of PWV in the large arteries (height divided by time between systolic and diastolic peaks (15). Augmentation index (AI), a measure of enhanced wave reflection, has been proposed as a bedside measure of aortic stiffness (16). Indeed, high levels of leptin have been documented in individuals with obesity and found to be correlated with reduction in arterial distensibility (17). In addition to hypothalamic receptors, receptors for leptin have been observed on the vascular endothelium and on smooth muscle cell (18,19). Accordingly, leptin can exert receptor-mediated influence on vessel tone and growth and, in cell culture, stimulate vascular smooth muscle proliferation and migration (20).
In addition, leptin induces oxidative stress in endothelial cells, and this action triggers the transcription of oxidant-sensitive genes that participate in atherogenesis. Peripheral Pulse Pressure, central Pulse Pressure and augmentation index, which provide additional information on wave reflection, are considered “surrogates” of arterial stiff- cness (21,22,23). O Brein et al stated strong association exits between Ambulatory arterial stiffness index (ASSI) and most reliable parameters of arterial stiffness like pulse wave velocity and augmentation index (24). In our study we measured stiffness index (SI) and augmentation index (AI) which can assess large and small artery compliance respectively by noninvasive measurement. Dolan and Hansen et showed that relation between stiffness index and cardiovascular mortality was linear (25,26).
A positive relationship has been demonstrated between type 2 diabetes mellitus and increased large artery stiffness (27). It is noteworthy that in individuals with obesity, increased aortic stiffness also may contribute to the development of cardiac hypertrophy, in addition to hypertension (28,29,30). We conclude that in subjects without hypertension and diabetes, BMI correlated with stiffness of the large artery (stiffness index) and small artery wall (Augmentation index). Indicating overweight and obesity can independently contribute to altered vessel wall compliance.
CONCLUSION Vessel wall compliance as measured by arterial stiffness is altered in obese and overweight individual. Implicaion of Study: To improve the vessel wall compliance Life style modifications on diet and exercise are mandatory for obese and overweight and prevent further progression to cardiovascular diseases.
ACKNOWLEDGEMENT Authors acknowledge immense help received from the scholars who’s articles are cited and included in references of this manuscript. The authors are grateful to the authors/ editors/ publishers of all those article journals and the books from where the literature of this article has been reviewed and discussed. I sincerely thank Professor Dr.K.N. Maruthy, for his extensive guidance in this research project. Source of funding : None Conflict of interest : None
References:
1. Brozak J and Keys A. The evaluation of leanness-fatness in man: norms and interrelationships. Food and agricultural organization of the United Nations. Dietary Surveys 1949; Vol-62(3):194- 206.
2. Jelic S, Bartels MN, Mateika JH, Ngai P, DeMeersman RE, Basner RC.Arterial stiffness increases during obstructive sleep apneas. Sleep 2002;25: 850–855.
3. Hall JE. The kidney, hypertension, and obesity. Hypertension 2003; 41:625–633.
4. I.S. Mackenzie, I.B. Wilkinson and J.R. Cockcroft. Assessment of arterial stiffness in clinical practice, Q J med 2002; 95:67–74.
5. G Sivagami, Milind Bhutkar, A Comparitive study of arterial stiffness indices between normotensive and hypertensive subjects-NJBMS,2014 : 4(3); pg-177-179.
6. Chen CH, Nevo E, Fetics B et al .Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure. Validation of generalized transfer function. Circulation 1997;95:1827-36.
7. Alvarez GE, Beske SD, Ballard TP, Davy KP: Sympathetic neural activation in visceral obesity. Circulation 106, 2002 : 2533– 2536.
8. Abate NI, Mansour YH, Tuncel M, Arbique D, Chavoshan B, Kizilbash A, Howell-Stampley T, Vongpatanasin W, Victor RG: Overweight and sympathetic overactivity in black Americans. Hypertension 2001;38: 379–383.
9. Garrow JS, Webster J. Quetelet’s index (W/H2) as a measure of fatness. Int J Obes 1985; 9: 147–153.
10. Krauss RM, Winston M, Fletcher RN, Grundy SM. Obesity: impact of cardiovascular disease. Circulation 1998; 98:1472–1476.
11. Oliver JJ, Webb DJ. Noninvasive assessment of arterial stiffness and risk of atherosclerotic events. Arterioscler. Thromb. Vasc. Biol. 2003; 23: 554–566.
12. Mattace-Raso F, Cammen T, Hofman A. et al. Arterial stiffness and risk of coronary heart disease and stroke. The Rotterdam Study. Circulation 2006; 113: 657–663.
13. Weber T, Auer J, O’Rourke M, et al. Arterial stiffness, wave reflections, and the risk of coronary artery disease. Circulation 2004; 109: 184–189.
14. Woodman RJ, Kingwell BA, Beilin LJ, Hamilton SE, Dart AM, Watts GF: Assessment of central and peripheral arterial stiffness: Studies indicating the need to use a combination of techniques. Am J Hypertens18 2005:249–260.
15. I.S. Mackenzie, I.B. Wilkinson, J.R. Cockcroft, Assessment of arterial stiffness in clinical practice, http://dx.doi.org/10.1093/ qjmed/95.2.67 67-74 , February 2002
16. Gary F. Mitchell, Yves Lacourcie`re, J. Malcolm O. Arnold, Mark E. Dunlap,Paul R. Conlin, Joseph L. Izzo, Jr ,Changes in Aortic Stiffness and Augmentation Index After Acute Converting Enzyme or Vasopeptidase Inhibition ,Hypertension. 2005;46:1111-1117.
17. Singhal A, Farooqi IS, Cole TJ, O’Rahilly S, Fewtrell M,Kattenhorn M, Lucas A, Deanfield J: Influence of leptin on arterial distensibility: A novel link between obesity and cardiovascular disease? Circulation 2002;106: 1919–1924.
18. Oda A, Taniguchi T, Yokoyama M: Leptin stimulates rat aortic smooth muscle cell proliferation and migration. Kobe J Med Sci,2001; 47: 141–150.
19. Sierra-Honigmann MR, Nath AK, Murakami C, Garcia-Cardena G, Papapetropoulos A, Sessa WC, Madge LA, Schechner JS, Schwabb MB, Polverini PJ, Flores-Riveros JR: Biological action of leptin as an angiogenic factor. Science ,1998;281: 1683– 1686.
20. Schafer K, Halle M, Goeschen C, Dellas C, Pynn M, Loskutoff DJ, Konstantinides S: Leptin promotes vascular remodeling and neointimal growth in mice. Arterioscler Thromb Vasc Biol , 2004;24: 112–117.
21. O’Rourke MF, Staessen JA, Vlachopoulos C, Duprez D, Plante GE. Clinical applications of arterial stiffness; definitions and reference values.Am J Hypertens. 2002; 15:426–444.
22. Van Bortel LM, Duprez D, Starmans-Kool MJ, Safar ME, Giannattasio C,Cockcroft J, Kaiser DR, Thuillez C. Applicationsof arterial stiffness, Task Force III: recommendations for user procedures. Am J Hypertens.2002; 15:445– 452.
23. Mackenzie IS, Wilkinson IB, Cockcroft JR. Assessment of arterial stiffness in clinical practice. QJM. 2002; 95:67–74. 24. O’ Brein E, Ambulatory blood pressure measurement: A trove hidden Gems? Hypertension 2006; 48:364-365
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





