IJCRR - 8(7), April, 2016
Pages: 38-41
Date of Publication: 12-Apr-2016
Print Article
Download XML Download PDF
UNILATERAL VARIATION OF THE RENAL VEIN AND TESTICULAR VEIN - A CASE REPORT
Author: Veena Vidya Shankar, Snigdha Das
Category: Healthcare
Abstract:Background: The right and left renal veins open into the inferior vena cava at right angle. The left renal vein is 3 times longer as compared to right. The right gonadal vein (testicular in male or ovarian in female) drains directly into inferior vena cava and left gonadal vein into left renal vein. Method: During the routine dissection teaching of posterior abdominal wall for first year MBBS students in the Department of Anatomy, MSRMC, Bangalore, we found the presence of double right renal veins along with variation in the termination of right testicular vein in an adult male cadaver aged 65 years. All the structures were carefully dissected, measurements noted and photographed using a digital camera. Observation: In the present case, two right renal veins (superior and inferior) were found to be draining into inferior vena cava separately and right testicular vein into inferior right renal vein Conclusion: This type of variation will help the radiologists for planning radiographic procedures; the surgeons for planning surgery to avoid intra and post-operative complications and the clinicians in recognition and protection of the variation..
Keywords: Additional renal vein, Renal transplantation, Testicular vein
Full Text:
INTRODUCTION Kidneys are a pair of excretory organs situated in the posterior abdominal wall. They are drained by renal veins. The arrangement of structures at the hilum of kidney from before backwards isrenal vein, renal artery and pelvis of ureter. Both the renal veins open into the inferior vena cava at right angle. The right renal vein lies posterior to second part of duodenum. The left renal vein is 3 times longer as compared to right. It lies posterior to splenic vein and body of pancreas at its origin, at the hilum, then crosses in front of the aorta before joining into inferior vena cava1 . Other than renal vein, any extra vein emerging out of hilum of kidney and draining separately into inferior vena cava is known as ‘additional vein’. The kidneys having this additional vein are classified as type 3 kidney. 14% cases have been reported to occur with additional renal veins.
These variations are ten times more common on the right side as compared to left side2 . The right gonadal vein (testicular in male or ovarian in female) drains directly into inferior vena cava and left gonadal vein into left renal vein1 .Right testicular vein draining into right renal vein instead of inferior vena cava has also been reported3 . Knowledge of these variations is important for the surgeons as well as for the radiologists in their daily practice. Embryology: During 5th week of development , venous system are arranged into 3 sets: vitelline veins draining blood from gut derivatives, umbilical veins carrying oxygenated blood from placenta to foetus and cardinal system of veins draining from body wall.
All the veins are bilaterally symmetrical and drain ultimately into sinus venosus. The cardinal system consists of anterior and posterior cardinal veins. The anterior and posterior cardinal veins join to form common cardinal vein which drains into right and left horn of sinus venosus on each side. The posterior cardinal vein appears in the mesonephric ridge. Following that the sub-cardinal and supra-cardinal veins appear ventro-medial and dorso-lateral to it respectively on each side4 .
The ‘renal collar’ is formed during the development of inferior vena cava as in the form of a circum aortic venous ring which is contributed anteriorly by sub-cardinal veins andinter-subcardinal anastomosis, posteriorly by supra-cardinal veins and inter-supra-cardinal anastomosis and on each side by supra-subcardinal anastomosis at 15mm stage of embryo5 . After the definitive positioning of metanephros the permanent venous pattern appears at 22mm stage of embryo. At around 8 weeks bilateral cardinal system of veins convert into unilateral right sided inferior vena cava right to aorta due to venous shifting to right side of body. In relation to it, two renal veins are present on each side (ventrally and dorsally).
One renal vein opens into the lateral part of renal collar and the other one towards the cranial part of supra-cardinal vein posteriorly in the right side. Following that there will be confluence of these two tributaries forming I single vessel which joins with the lateral portion of renal collar. Persistence of these tributaries leads to the formation of additional renal veins in the right side as observed in the present case. The right shifting of venous arrangement limits the retention of additional vein in the left side which would be required to reach across the aorta. The left renal vein develops from 3 sources: pre-aortic inter-sub-cardinal anastomosis, left subcardinal vein and left supra-subcardinal anastomosis.
This complex embryogenesis also limits the retention of additional left renal veins. Hence, presence of additional renal veins is more common in right side than the left side. Caudal parts of sub-cardinal veins give rise to gonadal veins. Gonadal veins drain into supra-sub-cardinal anastomosis. The right supra-sub-cardinal anastomosis and part of right sub-cardinal vein form inferior vena cava, so right gonadal vein drains into inferior vena cava. But in the present case, right testicular vein drained into right renal vein because here part of right supra-sub-cardinal anastomosis forms part of right renal vein.
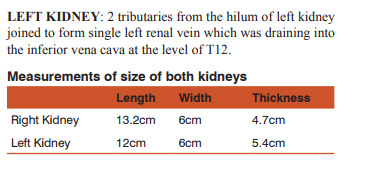
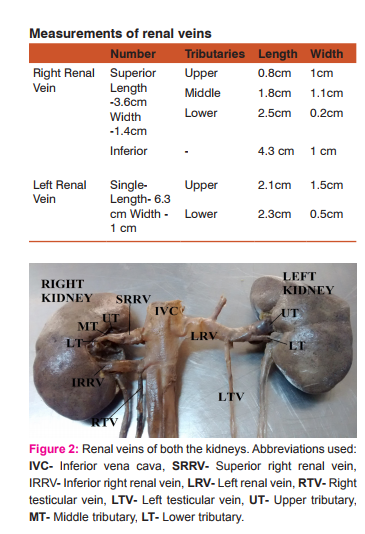
The left gonadal vein drains into left renal vein because left supra-sub-cardinal anastomosis gives rise to part of left renal vein6 . Method: During the routine dissection teaching of posterior abdominal wall for first year MBBS students in the Department of Anatomy, MSRMC, Bangalore, we found the presence of double right renal veins along with variation in the termination of right testicular vein in an adult male cadaver aged 65 years. All the structures were carefully dissected; measurements noted and photographed using a digital camera.
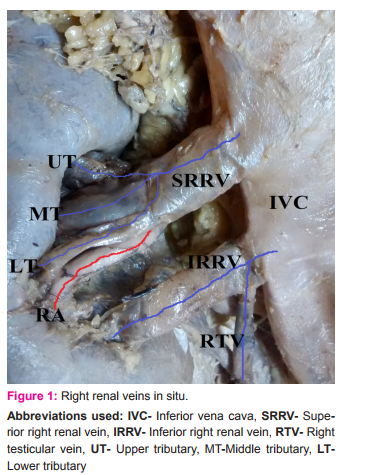
OBSERVATION RIGHT KIDNEY: Two right renal veins (named as superior and inferior right renal veins) were found to be terminating separately into inferior vena cava. Superior right renal vein: 3 tributaries (upper, middle and lower) from upper and middle parts of hilum of right kidney joined to form single superior right renal vein which was draining into the inferior vena cava at the level of termination of left renal vein (T12 level). Inferior right renal vein: From the lower part of hilum of right kidney it was draining into the inferior vena cava 1.5cm below the termination point of superior right renal vein running parallel to it. Right testicular vein was draining into inferior right renal vein at a distance of 0.8cm from the IVC instead of draining directly into it.
DISCUSSION In the present study we found double right renal veins draining separately into inferior vena cava. Another significant finding was right testicular vein terminating into inferior right renal vein instead of inferior vena cava. Incidences of presence of these similar additional veins were observed in 26% cases in the right side and 2.6% in the left side2 . Literature review showed that additional renal veins are common on right side(27.8%) as compared to left side(1%)7 . Several case reports have been reported with similar variations. Segmental branches of renal artery were found to be compressed between two right renal veins at the emergence of the veins at the hilum of right kidney8 . In a 50 years old male, double renal and testicular veins were observed bilaterally4 .
CLINICAL SIGNIFICANCE These variations as seen in the present case have practical importance in renal transplantation, renal and gonadal sur geries, uroradiology, gonadal or testicular colour Doppler imaging and other retroperitoneal therapeutic and diagnostic procedures9 .Veins and arteries of testes play an important role in their thermo-regulation that is essential for efficient functioning of the organs. Thus anatomical variations of renal and gonadal veins are very significant while performing surgery or radiology such ascendo-urological procedures, as lesions in them may cause severe back bleeding during and after surgery10. During renal transplantation both the recovery and implant surgeon should be aware of these anatomical variants of cadaver kidneys. The criteria to select a donor kidney suitable for transplantation may be based on the incidence of additional renal vein11.
If the inferior vena cava has been interrupted between additional veins, these veins may act as an alternate collateral route during surgery12.Knowledge of these variations of renal vascularanatomy are important during exploration and treatment of renal trauma, renal transplantation, renovascular hypertension, renal artery embolization, angioplasty or vascular reconstruction for congenital and acquired lesions, surgery for abdominal aortic aneurysm and conservative or radical renal surgery13.
CONCLUSION The knowledge of these venous anomalies are very important for the general and uro-surgeons approaching retro-peritoneal region especially during renal transplantation, physicians attending clinics, radiologists while performing investigations, as well as for anatomists for academic purpose.
ACKNOWLEDGEMENT The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of Funding: Nil Conflict of Interest: Authors declare that they do not have any conflict of interest ABBREVIATIONS USED: IVC- Inferior vena cava, SRRV- Superior right renal vein, IRRV- Inferior right renal vein, RTV- Right testicular vein, UT- Upper tributary, MTMiddle tributary, LT- Lower tributary.
References:
1. Sudeshna Majumder, Sibani Majumder, Hiranmoy Roy, Asis Kumar Ghoshal. A case of bilateral double renal veins. International Journal of Anatomical Variations.2013; 6:61-63.
2. Satyapal, K.S. Additional renal vein: incidence and morphometry. Clinical Anatomy.1995; 8:5-55.
3. Asala S., Chaudhary SC, Masumbuko-Kahamba N, Bidoms M. Anatomical variations of human testicular blood vessels. Annals of Anatomy.2001; 183(6): 545-9.
4. Verma R, Kalra S, Rana K. Malformation of Renal and Testicular Veins– A case Report. Journal of Anatomical Society of India. 2005;54(1): 29-31.
5. Williams et al: Gray’s Anatomy. In: Embryology and Development, 38thEdn; Churchill Livingstone, London. 1995; 324-326.
6. McClure and Butler. The development of Inferior Vena Cava. Am. J. of Anat. 1925; 35: 331-383.
7. Pick JW, Anson BJ. The renal vascular pedicle.An anatomical study of 430 bodyhalves.J Urol. 1940; 44: 411–434.
8. Dhar P. An additional renal vein.Clin Anat. 2002; 15: 64–66.
9. Sharmistha Biswas, J.C. Chattopadhyay, H. Panicker, J. Anbalaganand S.K. Ghosh. Variations In Renal And Testicular Veins –A Case Report. Journal of Anatomical Society of India.2006: 55(2):69-71.
10. Hoeltl W, Hrubi W, Aharinejad S. Renal vein anatomy and its implications for retroperitoneal surgery.1990;143:1108-1114.
11. Ross JA, Samuel E and Miller DR. Variations in therenal vascular pedicle (an anatomical and radiological study with particular reference to renaltransplant). Br.J.Urol.1961; 33:478-485.
12. Greweldinger, J, Coomaraswamy R, Luftchin S, Bosnaik MA. Collateral circulation through kidney after inferior vena cava ligation. N. England. J.Med.1969;258:541-542.
13. Sampaio, F. J. And Aragão, A. H. M. Anatomical relationship between the renal venous arrangement and the kidney collecting system. J. Urol., 144:1089-93, 1990.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





