IJCRR - 9(7), April, 2017
Pages: 44-48
Date of Publication: 11-Apr-2017
Print Article
Download XML Download PDF
Occupational Exposure and Needlestick Injuries among Employees of a Tertiary Care Institute in Kashmir
Author: Anjum B. Fazili, Rohul J. Shah, Qazi M. Iqbal, Feroz A. Wani, Beenish M.
Category: Healthcare
Abstract:Background: Needlestick injuries are one of the important occupational hazards of health care workers which pose serious health consequences. The present study examines the prevalence of NSIs among the employees of a tertiary care institute.
Methods: This cross-sectional study was carried out for a period of six months at Sher-i-Kashmir Institute of Medical Sciences, Soura. All categories of the workforce participated in the study.
Results: Out of a total of 2763 employees studied the prevalence of NSIs was 39.19% NSIs were more common in males, doctors, nursing staff and employees belonging to high risk group and the differences were statistically significant.
Conclusion: NSIs are a common public health problem in this tertiary care institute. Proper awareness with regard to adoption of standard precautions coupled with proper working conditions will help in ensuring control of potential blood borne infections due to occupational exposure in this tertiary care institute.
Keywords: Needlestick injury, Occupational exposure, High risk, Blood and body fluid
Full Text:
INTRODUCTION:
Health care workers have increased risk of occupational exposure to blood and other body fluids. Needle stick injuries (NSIs) are major cause of blood borne infections transmitted among health care personnel. These preventable injuries expose workers to over different blood borne pathogens[1] and the most common being Hepatitis B, Hepatitis C and HIV.[2] Most exposures among HCWs are caused by percutaneous injuries with sharp objects contaminated with blood or body fluids which include needles, scalpels, lancets and broken glass. NSIs are therefore one of the potential occupational hazards for HCWs. Transmission of at least twenty different pathogens by injuries due to sharps instruments and needlesticks has been reported in the literature.[3,4]
Globally, more than 35 million HCWs face the risk of sustaining a percutaneous injury with a contaminated object every year.[5] American health workers suffer 800,000 to 1 million NSIs annually excluding those that go unreported.[4,6,7] More than 100,000NSIs occur in UK hospitals each year.[7,8] In India, it is not known exactly how many occupation related injuries occur each year, and as data are scarce, it is not possible to estimate an annual incidence[9,10].
An HCWs chance of contracting HIV after an HIV infected accidental NSI is 1 in 250, while the chance of contracting HBV after an accidental NSI is 1 in 20while the chances of contracting HCV after exposure to an HCV contaminated needle stick is 3.5 in 100[11] Although lower transmission rate is found for HIV <0.3%,[5] about 1000 HIV infections mostly in developing countries could occur every year worldwide among HCWs due to exposure to percutaneous injuries. This occupational acquisition of HIV represents a serious consequence of NSIs[5]. HCWs are at risk of the deadly Ebola virus disease which is an emerging infectious disease contracted through exposure to blood and body fluid of infected patients which may be through NSIs[12]. The same is true of Lassa fever[13].
With this background, the present study was undertaken up to know the extent of occupational exposure to needle stick injuries among health care personnel of tertiary care hospitals. The present study also aims to study the actions taken by the HCWs following an accidental NSI exposure.
MATERIAL AND METHODS:
This cross-sectional study was carried out from April 2014 to October 2014 for a period of six months at Sher-i-Kashmir Institute of Medical Sciences, Soura. All categories of the workforce, which included doctors, nursing-staff, lab-staff, sanitation-staff, administration, laundry and linen, participated in the study. The participants were further broadly classified into high risk and low risk groups depending on the risk of exposure to infectious material. High-risk group include doctors, nursing staff, paramedic/ lab-staff, sanitation, laundry and linen. Low risk group included staff of the hospital administration who was not directly involved with the infectious agent. Needlestick injuries in this study included injuries caused by sharps used during medical intervention such as needles, cannulas and intravenous sets. All the participants were explained the objective of the study and written informed consent was taken from each of them. The data was collected using a pretested, semi structured questionnaire. The questionnaire consisted of information related to socio demographic details, history related to their occupational exposure to needlestick injury in their work tenure.
DATA ANALYSIS:
Data was analyzed by using SPSS software version 20. Results are represented in the form of tables and figures. Chi square test was used for univariate analysis and p value of less than 0.05 was considered as statistically significant.
RESULTS:
Among 2763 employees who participated in the study, 71.4% were males and 28.6% were females. Mean age of employees was 40.46 ± 10.1 years. 57.9% of employees were between 31-50 years of age while only 17.1% were above 50 years of age (Table 1).
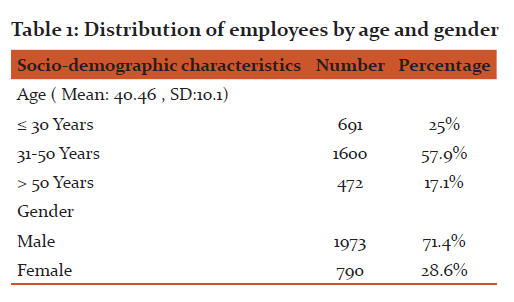
Table 2 depicts that out of total 2763 employees, 27.90% belonged to nursing staff, 24.50% were doctors, and 27.36% belonged to administration and rest of employees 11.11%, 7.35%, 1.77% belonged to lab staff, sanitation, laundry and linen respectively. 72.64% of employees belonged to high risk group and 27.36% to low risk group. High- risk groups included doctors, nursing staff, para- medic/ lab-staff, sanitation, laundry and linen. Low risk group included staff of the hospital administration who were not directly involved with the infectious agents.
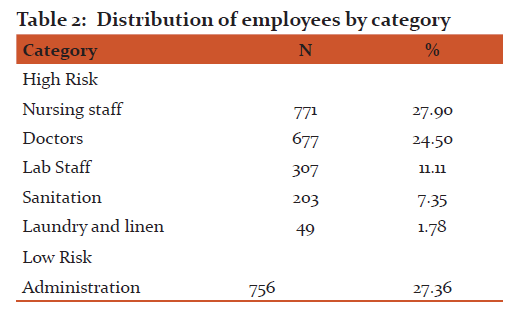
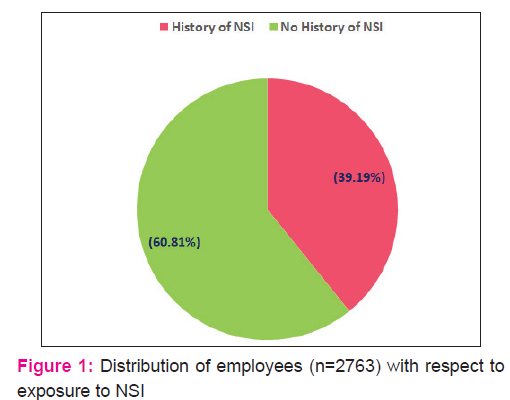
Table 3 depicts that 64.16%% of employees gave history of some kind of occupational exposure. Among those employees who gave history of occupational exposure 43.20% gave history of needle stick injury, 38.91% had blood and body splash and 17.87% gave history of both kinds of exposure (Table 3 ). Among the total employees who participated in the study, 1083 (39.19%) had history of needle stick injury (Fig. 1).

Among the HCWs with NSIs, doctors had the highest percentage (38.6%) followed by nurses (37.9%). laboratory staff (12.3%) and sanitation staff (7.1%). These differences with respect to designation and occurrence of NSIs were found statistically significant. Almost all NSI’s (96.7%) were found in the high risk group employees.(Table 4)
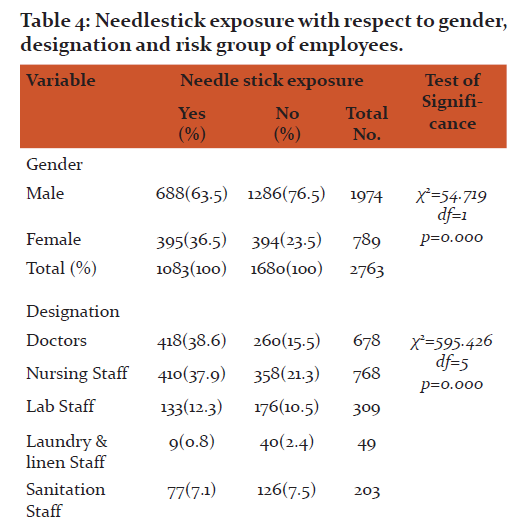
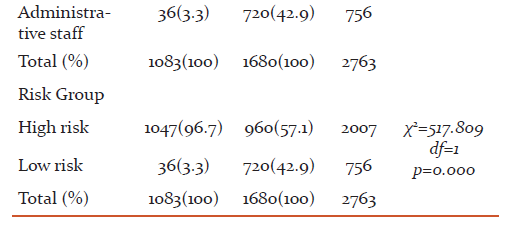

Table 5 depicts that 44.1% of the needlestick injuries was as a consequence of giving injections, 23.5% while drawing blood, 19.8% during suturing and 7.6% as a consequence of recapping of needles. In 79.605 cases a hollow bore needle was responsible for the injury. Only 27.23% of the employees who sustained needlestick injuries were wearing gloves.
With regards to the action taken following accidental exposure only 5% among high risk group took post-exposure prophylaxis (PEP), reported to authorities and washed the exposed part while other 0.5% of employees among this group took only PEP. Majority of employees (92.6%) immediately washed the exposed part following an accidental NSI (Fig.2).

DISCUSSION:
The mean age of our study participants was 40.46±10.01years which was almost in accordance with that observed by Maryam Amini et al[14] (37±9years). Holla et al[15] in their study also reported majority of study participants belonging to age group between 25 and 45 years with mean age as 35.53±9.45years. Majority of our study participants were males (71.4%). This was contrary to that reported by Maryam Amini et al[14] in their study where 58.8% were females. Holla et al [15] also reported almost equal distribution of males and females. The most common occupational category in our study were nurses (27.90%) followed by doctors (24.50%) and administrative staff (27.36%). Maryam Amini et al[14] also reported nurses as the predominant category among their study participants. Contrary to this Devendra Jaybhaye et al[16] and Holla et al [15] reported that doctors were the most common among their study participants. In our study out of a total of 2763 study participants 1083 gave history of needlestick injury thus giving an overall prevalence of NSI as 39.19%. This is much lower than that reported by Chen et al[17] (71.3%), Holla R et al[15] (71.9%) and Maryam Amini et al [14] (67.8%). Different prevalence rates have been reported from other countries including 55.5% from Thailand[17], 57 % in England [18] and 72.4% from Canada [19]. The present study revealed that doctors suffered the highest number of NSIs followed by nurses. Similar observations were reported by Salelkar et al [20] and Rahul Sharma et al. However, Muralidhar et al[22] and Devendra Jaybhaye et al[16] reported that NSIs were more common in nurses followed by doctors. Evans et al[23] in their study in UK also reported that nurses were the commonest victims of NSIs. Needle stick injuries were more common among male employees of our study population. Salelkar et al[20] in their study reported almost equal prevalence of NSIs in males and females. Contrarily, Maryam Amini et al[14] reported that female employees had NSIs more than males. The most common procedure responsible for NSI in our study was injection administration (44.1%) followed by blood drawing in 23.5% cases, suturing in 19.8% cases and recapping of needle in just 7.6% 0f incidents. Salelkar S et al[20] reported maximum NSIs following sharps disposal (31.7%), 21.6% during operative procedures, 13.8% during withdrawal of samples, 13.2% during injections and 6.3% while recapping of needles. However Rahul Sharma et al[21] and Muralidhar et al[22] reported recapping as the most common procedure responsible for NSIs with 34% and 39% NSIs respectively associated with recapping. Devendra Jaybhaye et al[16] reported that in 52% of NSIs recapping of needle was responsible. Muralidhar et al [22] in their study however, reported withdrawal of blood as the commonest clinical activity to cause NSI. In 79.6% of our NSI incidents hollow bore needles were involved. Similar observations were reported by Salelkar et al [20] who reported that in 77.5% incidents of NSIs hollow bore needles were responsible. Rahul Sharma et al[21], Devendra Jaybhaye et al[16] and Muralidhar et al[22] also reported hollow bore needles being responsible for majority of the NSIs. As far as personal protection is concerned, only 27.3% of our employees were wearing gloves at the time of NSI. Contrary to this Maryam Amini et al[14] reported that only 1.8% used protective barriers. Muralidhar et al [22] in their study reported that majority of health care workers (74%) were wearing gloves at the time of NSI. In another study by Salelkar et al[20] 58% of the health care workers were wearing gloves at the time of injury. Following the NSI, majority (92.6%) of employees immediately washed the exposed part, 5% of the employees washed exposed part, reported to the authorities and took PEP while as a small percentage 0.5% took only PEP. Muralidhar et al[22] in their study reported that 74% of those suffering a NSI took action in the form of washing the site, applying antiseptic, reporting to seniors and seeking advice on PEP. Salelkar S et al[20] in their study reported that 3% of HCWs with NSI had taken PEP for HIV and 32% of HCWs reported the injury to concerned superiors. In a study by Rahul Sharma et al [21] it was reported that 27.5% HCWs reported a NSI to their senior and 20.7% got their blood tested immediately after injury.
CONCLUSION: NSIs are a common public health problem in this tertiary care institute hence guidelines regarding disposal of biomedical waste must be strictly followed. Proper and continuous awareness among staff with regard to adoption of standard precautions coupled with immunization against hepatitis B, proper working conditions and cooperative atmosphere in the hospital will help in ensuring control of potential blood borne infections due to occupational exposure in this tertiary care institute.
ACKNOWLEDGEMENT: We are thankful to all those staff members of the institute who participated in the study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Ethical Clearance: Not required
Informed Consent: Taken individually
Financial support: Nil
Conflict of interest: Nil
References:
- Elizabeth A, Bolyard R, Ofelia CT, Walter WW, Pearson ML, Craig N, et al. Guideline for infection control in health care personnel, 1998. Am J Infect Control. 1998;26(3):289–327.
- Hughes S. Annual Number of Occupational Percutaneous Injuries and Mucocutaneous Exposures to Blood or Potentially Infective Biological Substances. International Healthcare Worker Safety Center, University of Virginia. 1998 [cited 2013 Sep 7]. Available from: http://www.healthsystem.virginia.edu/pub/epinet/estimates.html
- Saleem T, Khalid U, Ishaque S, Zafar A. Knowledge, attitudes and practices of medical students regarding needle stick injuries. J Pak Med Assoc 2010;60:151?6.
- World Health Organization ICN on Preventing Needlestick Injuries. Facts and Issues. 2000.
- Wicker S, Jung J, Allwinn R, Gottschalk R, Rabenau HF. Prevalence and prevention of needlestick injuries among health care workers in a German University Hospital. Int Arch Occup Environ Health 2008;81:347?54
- Hanafi MI, Mohamed AM, Kassem MS, Shawki M. Needlestick injuries among health care workers of University of Alexandria Hospitals. East Mediterr Health J 2011;17:26?35.
- Mokuolu OA. Needlestick Injuries in Nigerian Health Workers. Available from: http://www.thefreelibrary.com/Needle+stick+injuries+in+Nigeria+Health+Care+Worker. [Last accessed on 2015 Dec 27].
- Adams D, Elliot TS. A comparative user evaluation of three needle protective devices. Br J Nurs 2003;12:470-4.
- Jayanth ST, Kirupakaran H, Brahmadatan KN, Gnanaraj L, Kang G. Needle stick injuries in a tertiary care hospital. Indian J Med Microbiol 2009; 27 : 44-7.
- Rele M, Mathur M, Turbadkar D. Risk of needle stick injuries in health care workers – a report. Indian J Med Microbiol 2002; 20: 206-7.
- Jahan S. Epidemiology of needlestick injuries among health care workers ina secondary care hospital in Saudi Arabia. Ann Saudi Med 2005;25:233-8.
- European Centre for Disease Prevention and Control. Rapid risk assessment of Ebola in West Africa. Stockholm. 2014. Available from: http: //www.ecdc.europa [Last accessed on 2014 Sep 15].
- Asuzu MC, Adebiyi AO. Prevention of nosocomial outbreaks of Lassafever. Arch Ib Med 2007;9:42?5.
- Amini M, Behzadnia MJ, Saboori F, Bahadori MK, Ravangard R. Needle stick injuries among health care works in a Teaching Hospital. Trauma Monthly. 2015 Nov;20(4).
- Holla R, Unikrishnan B, Ram P, Thapar R, Mithra P, Kumar N et al. Occupational exposure to needle stick injuries among health care personnel in a tertiary care hospital: A cross sectional study. J. Community Med Health Education S2:004.doi:10.4172/2161-0711,S2-004.
- Jaybhaye D, Dahire P, Nagoankar A, Vedpathak V, Deo D, Kawalkar U. Needle stick injuries among health care workers in a tertiary care hospital in rural India. Int.journal of medical Science and Public Health.2014; 3 (1):49-52.
- Chen L, Zhang M, YanY, MiaoJ, Lin H, ZhangY, et al. Sharp object injuries among health care workers in a Chinese Province. AAOHN J.2009;57(1):13-16.
- Honda M, Chompikul J, Rattanapan C, Wood G, Klungboonkrong S. Sharps injuries among nurses in a Thai regional hospital: Prevalence and risk factors. Int J Occup. Environ Med. 2011;2(4):215-23.
- Cleveland JL, Barker LK, Cuney EJ, Panlilio AL. National Surveillance System for health Care Workers. Preventing percutaneous injuries among dental health care personnel. J Am Dent Assoc.2007;138(2):169-78.
- Salelkar S, Motghare DD, Kulkarni MS, Vaz FS. Study of needle stick injuries among health care workers at a tertiary care hospital. Indian Journal of Public Health.2010;54(1):18-20.
- Sharma R, Rasania SK, Verma A and Singh S. Study of prevalence and response to needlestick injuries among health care workers in a tertiary care hospital in Delhi, India. Indian J Community Med 2010;35(1):74-77.
- Muralidhar S, Singh PK, Jain RK, Malhotra M and Bala M. Needle stick injuries among health care workers in a tertiary care hospital of India. Indian J Med Res 131, March 2010:405-410.
- Evans B, Duggan W, Baker J, Ramsay M, Abiteboul D. Exposure of health care workers in England Wales and the Northern Ireland to blood borne viruses between July 1997 and June 2000: Analysis of surveillance data. BMJ 2001;322:397-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





