IJCRR - 9(7), April, 2017
Pages: 19-22
Date of Publication: 11-Apr-2017
Print Article
Download XML Download PDF
A Comparative Study of Carrying Angle with Respect to Sex and Dominant Arm in Eastern Population of Nepal
Author: Rakesh Kumar Adhikari, Subodh Kumar Yadav, Abhishek Karn
Category: Healthcare
Abstract:Objective: To find the gender and dominant handedness difference in the carrying angle of adolescent males and females of eastern population of Nepal.
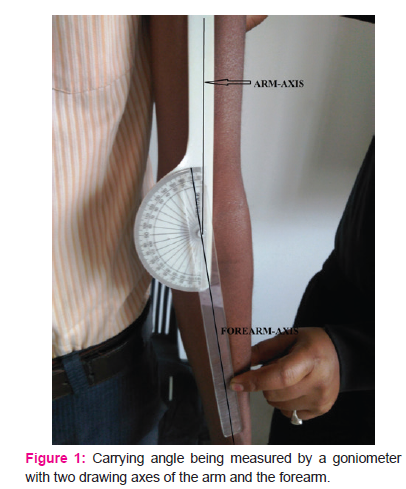
Methods: The carrying angle was measured by a goniometer in 100 healthy subjects without any anomaly, pathology or asymmetry in shoulder, elbow or wrist (50 males and 50 females) by extending, supinating and fixing each forearm and placing the fixed arm of the goniometer on the central longitudinal axis of the upper arm and the adjustable arm of the goniometer on the central longitudinal axis of the lower arm. The means were evaluated using the Student t-test where p < 0.05 was considered to be statistically significant.
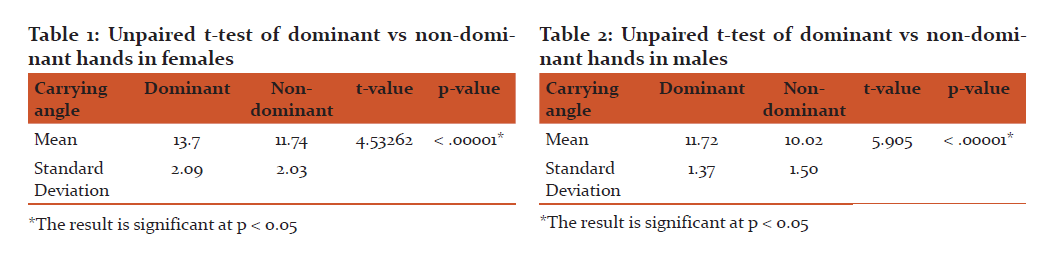
Results: The mean carrying angle of males on the dominant upper limb was 11.72\?1.37 and the non-dominant upper limb was 10.02\?1.5 and the mean carrying angle of females on the dominant upper limb was 13.7\?2.09 and the non-dominant upper limb was 11.74\?2.03. The carrying angle was significant greater in females (p < 0.00001) and in the dominant arm in both sexes (p < 0.00001).
Conclusions: Our observation of carrying angle can be used to assess traumatic elbow injuries and as an adjunct to identification of skeletal remains in forensic practice in this population.
Keywords: Carrying angle, Gender, Dominant arm, Adolescents
Full Text:
Introduction
The arm and the forearm are not aligned in humans, which is most obvious when the elbow is straight and the forearm fully supinated. An acute angle at the elbow medially made by the long axis of the humerus and the long axis of the ulna in the anatomic position is recognized as the carrying angle.1 A little degree of cubitus valgus is fashioned by the axis of a radially swerved forearm and the axis of the humerus which assists the arms whilst walking to move to and fro without thumping the hips.2 The normal carrying angle in males is 5°-10° and slightly greater in females being 10°-15°. 3 If this angle is > 15°, it is called cubitus valgus whearas if it is < 5° it is called cubitus varus.3 The angulation is as a consequence of the configuration of the articulating surfaces of the humeral condyles that articulate with the radius and ulna. This angulation vanishes when the forearm is pronated and the elbow is in full extension and when the supinated forearm is flexed alongside the humerus in full elbow flexion.4
The angle differs noticeably between individuals and it is greater in females as compared to males and greater in adults as compared to children. Females have narrower shoulders and wider hips than males which may be a suitable cause for having a more acute carrying angle and is therefore deemed as one of the secondary sexual characters.5-9
Nevertheless, there is a wide overlap in this angle between males and females, and a gender difference has not been steadily scrutinized in scientific studies.2, 10 Therefore, this present study was carried out to estimate the gender dominant handedness difference in the carrying angle of pubescent males and females of eastern population of Nepal. Furthermore, our study might be helpful in monitoring of traumatic elbow injuries which frequently necessitate appraisal of the carrying angle. Additionally, the forensic experts may employ our study to determine the gender of an individual of this area from skeletal remains.
Materials and Methods:
A total of 200 elbows of 100 healthy young males and females belonging to the age group of 16 to 24 years with normal bony configuration in equal sex ratio were examined at the Department of Human Anatomy of Nobel Medical College Teaching Hospital, which is situated in eastern Nepal. Individuals with shoulder, elbow or wrist pathologies, asymmetry, congenital malformations, history of elbow surgery, and fracture of limbs were excluded from the study. They were placed in anatomical position and the bony landmarks (olecranon process of the ulna, head of the radius, medial and lateral epicondyles of humerus and head of ulna) were acknowledged by means of palpation. Then the carrying angle was measured by a goniometer by extending, supinating and fixing each forearm. The fixed arm of the goniometer was placed on the central longitudinal axis of the upper arm and the adjustable arm of the goniometer was placed on the central longitudinal axis of the lower arm.11
Figure 1
The angle thus measured was noted by two observers to evade interobserver disparity. The carrying angle of dominant and non-dominant hands was recorded separately.
Statistical Method:
The obtained data were statistically analyzed using the SPSS® for Windows, Version 17.0. Continuous variables means were evaluated using the Student t-test where p < 0.05 was considered to be significant.
Results
The mean carrying angle of males on the dominant upper limb was 11.72±1.37 and the non-dominant upper limb was 10.02±1.5 and the mean carrying angle of females on the dominant upper limb was 13.7±2.09 and the non-dominant upper limb was 11.74±2.03.
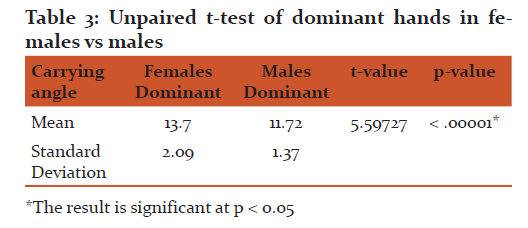
In this study we observed that there was a significant difference (p< .00001) between the carrying angles of dominant and non-dominant hands in the same gender as well as in the carrying angles of dominant hands in between males and females as shown in the tables below.
Table 1
Table 2
Table 3
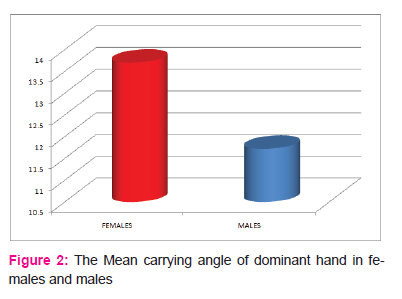
Figure 2
Discussion
In this present study, the mean carrying angle of males on the dominant upper limb was 11.72±1.37 and the mean carrying angle of females on the dominant upper limb was 13.7±2.09. The mean carrying angle of dominant hand in females was more compared to that of males which was found to be statistically significant. The first researcher to carry out a study on variation of carrying angle in between males and females was Potter H.P who observed the carrying angle to be greater in females as compared to males.5 Except few researchers who found no significant difference between the carrying angles of males and females 10-14 most of the study shows that the carrying angle of females was greater than males 2, 5- 9, 16-24 also observed by our study which shows that the carrying angle of dominant hand of females and males differ statistically.
We also observed that the mean carrying angle of the dominant hand was more as compared to the non-dominant hand in either sexes (males:11.72±1.32 vs 10.02±1.50; females: 13.7±2.09 vs 11.74±2.03) and this too was statistically significant finding also observed in other studies.21,22,24 This significant difference between the carrying angles of the dominant and non-dominant sides may imply more laxity of the ligament at the medial elbow or bony remodeling to adapt more stress in the dominant hand.
However, we did not analyze the influence of variables like height, age and race of the individual, length of the arm, length of the forearm, and width of the hip to the carrying angle.
Conclusion
Our subjects were adolescents and the carrying angle was significantly more in females as compare to males which may be due to laxity of articular ligaments and a wider pelvis, the outcome of which is a greater tangential divergence of the forearm on the arm. The carrying angle of dominant arm was observed to be greater than the non-dominant arm in both males and females which was statistically significant. This may be because of bony remodeling to adapt more and repeated stress in the dominant arm due to its more frequent use as compared to the non-dominant arm.
Our observed values will be important in the management of traumatic elbow injuries and in the diagnosis of diseases of the lateral and medial epicondyles which frequently necessitate appraisal of the carrying angle. Our finding can also be used as an indicator of gender in this population and thus an adjuvant forensic parameter to aid in identification of human remains which is an important part of medicolegal practice.
Acknowledgement
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Ethical Clearance
Ethical clearance was obtained from the Institutional Review Committee of Nobel Medical College and Teaching Hospital, Biratnagar-5, Morang.
Source of Funding
None declared.
Conflict of interest
None declared.
References:
- Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Ferguson MW, Greys Anatomy, 38th Ed, Churchill Livingston, London, 1995. pp.642-643.
- Van RP, Baeyens JP, Fauvart D, Lanssiers R, Clarijs JP. Arthro-kinematics of the elbow: study of the carrying angle. Ergonomics 2005;48:1645–56.
- David J. Magee, Orthopedic Physical assessment, 6th edition (2014),: 392-393.
- Norkin, C.C,P.K. Levangie, The elbow complex. In Joint Structure and Function, 4th Ed, F.A. Davis, Philadelphia, 2005. pp.284
- Potter HP. The obliquity of the arm of the females in extension. J Anat Physiol 1895;29:488-492.
- Atkinson WD. Elftman H. The carrying angle of the human arm as a, secondary sex character. Anat Record 1945;91:49-53.
- Aebi H, Ellbogenwinkel DER, Geschlecht SB, Hüftbreite KU. Acta Anat 1947;3:228-264.
- Keats TE, Teeslink R, Diamong AE, Williams JH. Normal axial relationship of the major joints. Radiol 1966;87:904-908.
- Baugman FA, Higgins JV, Wads¬worth TG, Demaray MJ. The carrying angle in sex chromosome anomalies. JAMA 1974;230:718-720.
- Zampagni M, Casino D, Zaffagnini S, Visani AA, Marcacci M. Estimating the elbow carrying angle with an electrogoniometer: acquisition of data and reliability of measurements. Orthopedics 2008;31:370.
- Bari W, Alam M, Omar S. Goniometry of elbow carrying angle: a comparative clinical study on sexual dimorphism in young males and females Int J Res Med Sci. 2015;3(12):3482-3484.
- Steel FLD, Tomalinson JDW. The carrying angle in man. J Anat. 1958;92:315-317.
- Smith L. Deformity following supracondylar fractures of the humerus. J Bone joint surg. 1960;42-A:235-238.
- Maria LZ, Daniela C, Sandra M, Andrea V, Maurilio M. Estimating the elbow carrying angle with an electrogoniometer. J Shoulder elbow surg 2008;17(1):106-112.
- Zampagni ML, Casino D, Zaffagnini S, Visani AA, Marcacci M. Estimating the elbow carrying angle with an electrogoniometer: acquisition of data and reliability of measurements. Orthopedics. 2008;31(4):370.
- Purkait R. An Anthropometric investigation to the probable cause of formation carrying angle. A Sex indicator. JIAFM 2004;26:14?20.
- Balasubramanian P, Madhuri V, Muliyil J. Carrying angle in children: a normative study. J Pediatr Orthop B. 2006;15:37-40.
- Golden DW, Jhee JT, Gilpin SP, Sawyer JR. Elbow range of motion and clinical carrying angle in a healthy pediatric population. J Pediatr Orthop B. 2007;16:144-149.
- Tükenmez M, Demirel H, Perçin S, Tezeren G. [Measurement of the carrying angle of the elbow in 2,000 children at ages six and fourteen years]. Acta Orthop Traumatol Turc. 2004;38:274-276.
- Sharma K, Mansur DI, Khanal K, Haque MK. Variation of carrying angle with age, sex, height and special reference to side. Kathmandu Univ Med J (KUMJ). 2013;11(44):315-8.
- Paraskevas G, Papadopoulos A, Papaziogas B, Spanidou S, Argiriadou H, Gigis J. Study of the carrying angle of the human elbow joint in full extension: a morphometric analysis. Surg Radiol Anat. 2004;26:19–23.
- Yilmaz E, Karakurt L, Belhan O, Bulut M, Serin E, Avci M. Variation of carrying angle with age, sex, and special reference to side. Orthopedics. 2005;28(11):1360-1363.
- Chein-Wei Chang, Yi-Chian Wang, Chang-Hung Chu. Increased Carrying Angle is a Risk Factor for Nontraumatic Ulnar Neuropathy at the Elbow. Clin Orthop Relat Res. 2008; 466(9):2190–2195.
- Allouh MZ, Abu Ghaida JH, Jarrar AA, Khasawneh RR, Mustafa AG, Bashaireh KM. The carrying angle: racial differences and relevance to inter-epicondylar distance of the humerus. Folia Morphol (Warsz). 2016;75(3):388-392.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





