IJCRR - 12(14), July, 2020
Pages: 117-122
Date of Publication: 22-Jul-2020
Print Article
Download XML Download PDF
Transition to Competency-Based Medical Education: A Proposed Rollout Model
Author: Tripti K Srivastava, Lalitbhushan S Waghmare, Alka T Rawekar
Category: Healthcare
Abstract:The Undergraduate Medical education curriculum in India is revised to competency-based Competency-Based Medical Education (CBME)) as per Graduate Medical Education (amendment 2019) from 2019 \? 20 onwards. This manuscript suggest a Competency-Based Medical Education (CBME) Roll out model that can aid Medical Institutes across India to plan and implement this revised curriculum. The Model suggests formulation of various relevant committees, their terms of reference, Phases of roll out (Planning, implementation, Monitoring, Evaluation and Amendment) and GANTT chart. Implementation of reforms in a phasic manner with capacity building at relevant intervals, as suggested in the model, will provide a steady foundation to the revised curriculum and will ease the process of change.
Keywords: Competency-Based Medical Education, Indian Medical Graduate, Ethics and Communication.
Full Text:
Introduction:
The Undergraduate Medical education curriculumin India is revised to competency–based as per Graduate Medical Education (amendment 2019) from 2019 to 20 onwards.1 The emphasis is to enable Indian Medical Graduate (IMG) to recognize "Health for all" as a National goal and fulfill his/her societal obligations.1 The revised curriculum is better aligned with Health professional attributes that are locally relevant and globally adaptive. The goal is that the IMG must be able to function in the roles of Clinician, Leader and Member of health care team, Communicator and Life long learner and Professional appropriately and effectively. Competency based learning includes designing and implementing medical education curriculum that focuses on the desired and observable ability in real life situations. Competency, per se, is defined as the habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values, and reflection in daily practice for the benefit of the individual and community being served.2
The regulatory body of Medical education suggests the broad framework of Competency-Based Medical Education (CBME).1,3 This manuscript suggests a comprehensive roll out plan by Jawaharlal Nehru Medical College, a constituent unit DMIMS, a deemed to be University, with flexibility of appropriate incorporations at local level to suit the need and context, keeping the broad framework intact. The various reforms that are contemplated with regards to Competency-Based Medical Education (CBME) are as stated under;
-
Aligned and integrated curriculum
-
Foundation course
-
Early clinical exposure
-
Electives
-
Student - Doctor Method of Clinical Training
-
Certification of essential skills
-
Attitude, Ethics and Communication (AETCOM) skill module
-
Self directed learning
-
Co-curricular activities
-
Reforms in Formative, Internal and Summative Assessments
The rollout plan incorporates formulation of specific committees, terms of reference, phases of rollout, and Gantt chart.
-
Composition of various committees :
New COMPETENCY-BASED MEDICAL EDUCATION (CBME) curriculum must be phased out through the co-ordination of three significant committees viz.1. Departmental Curriculum Committee (DCC), 2. College Curriculum Committee (CCC) and 3. Expert Group (EG).
The Composition of the three committees is proposed as under;
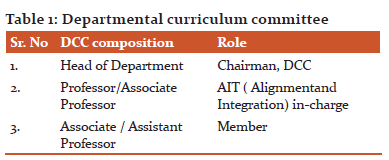
a. Departmental Curriculum committee (DCC) : The DCC committee must consist of three members who have undergone training in MCI recognized Basic course workshop and Curriculum Implementation and Support program (CISP).
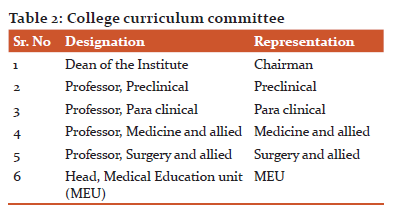
b. College Curriculum Committee(CCC) : The College Curriculum Committee must consist of six members, in accordance with BOGs, MCI guidelines as stated below;
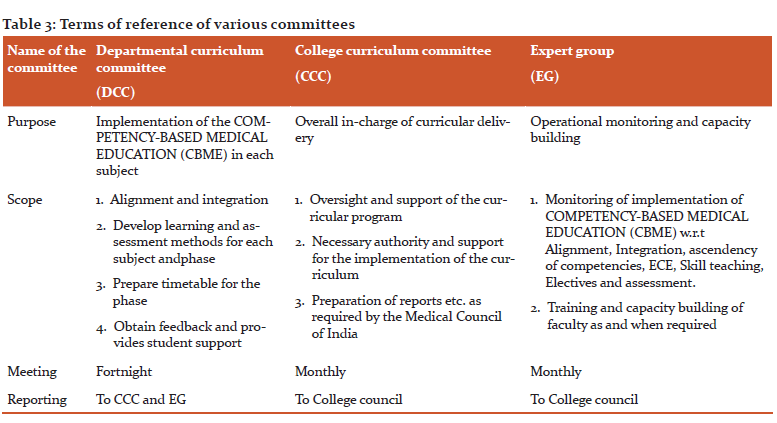
c. Expert group (EG): Four expert groups viz 1.Alignment Integration and ECE , 2. Assessment 3. Skills and 4.Electivesmust be formed. Each expert groups can consist of five members, each of whom have undergone training in MCI recognized Basic/revised basic course in Medical Education, Curriculum Implementation and Support Program and Advance course in ME/MPhil HPE. Each group must have a Co-convener and a member of CCC. The overall in-charge of the expert groups must be MEU co-coordinator. Each expert group will be responsible for operational monitoring and need based capacity building with regards to COMPETENCY-BASED MEDICAL EDUCATION (CBME). The terms of reference of various committees are identified in table no 3.
-
Phases of Roll-out :
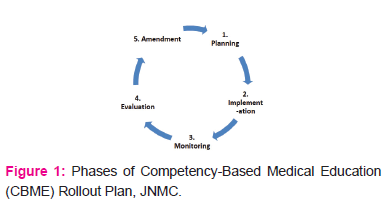
As mentioned in earlier paragraphs, the various reforms must be rolled out in five phases, as stated below;
1 : Planning phase
The first step to sustainable curricular reform is proper planning. The entire rollout plan must be planned with respect to desired tasks at hand, timeline and responsibility. Planning phase begins from the year of launch of first professional year with new curriculum and must continue prospectively for forthcoming professional years viz Professional year II, III and VI.
The planning phase comprises of two parallel levels of operation as depicted below;
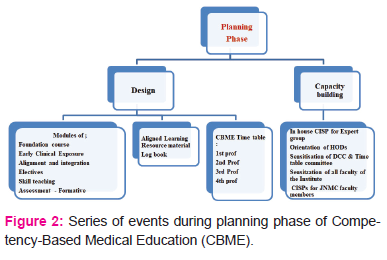
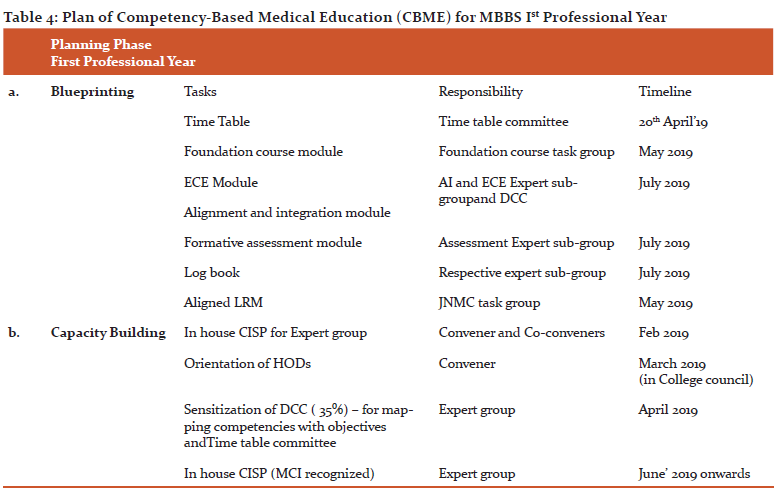
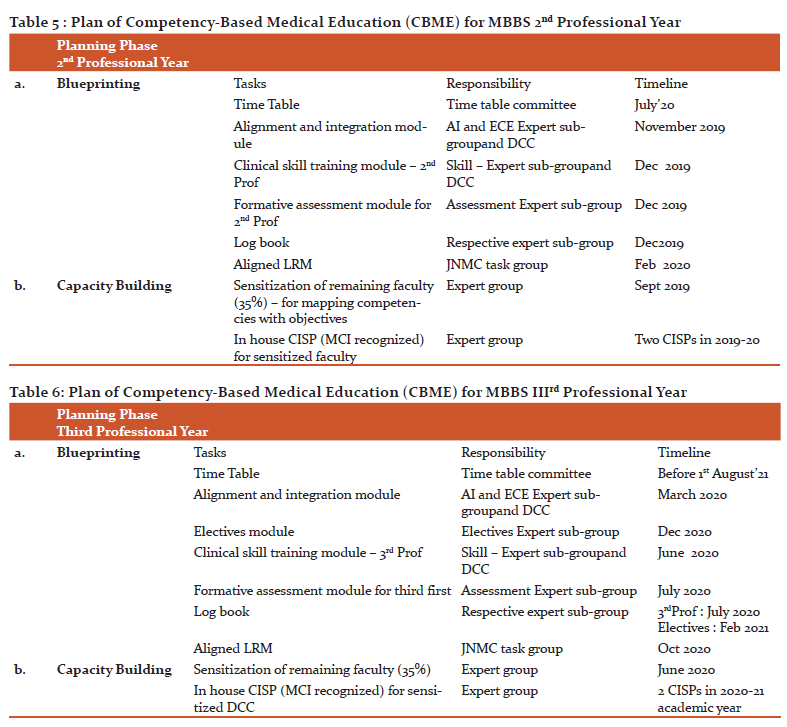
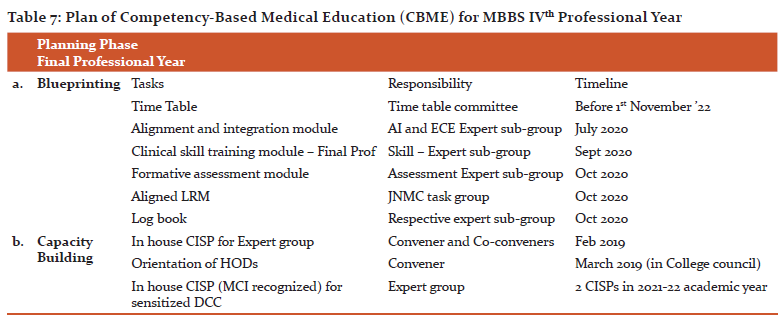
The tables 1-4 gives operational details during planning phase for Ist – IVth professional year, for the new curriculum launched in 2019academic year, under the sections of Blueprinting and Capacity building.
2. Implementation phase: Implementation of Competency-Based Medical Education (CBME) must be done prospectively and routed through Dean of the Institute and departmental curriculum committee headed by Head of Department. Need based capacity building must be taken up by Expert group as and when required.
Report: DCC must submit the report of Competency-Based Medical Education (CBME) implementation to CCC on quarterly basis. The compiled quarterly reports must be submitted to Medical Education Unit on annual basis which should be later submitted to Regulatory body for compliance.
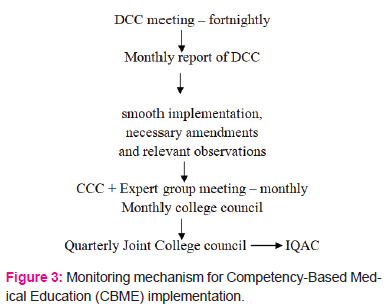
3.Monitoring Phase:
The monitoring will be done at two levels, as stated below;
1. Mechanical monitoring: DCC
2. Operational monitoring: Expert group
It is proposed that DCC must meet fortnightly to discuss implementation of Competency-Based Medical Education (CBME) at the departmental level. The monthly report from DCC must be submitted to CCC. The CCC and expert group meetings should be held monthly to review the reports of DCC to ensure smooth implementation, necessary amendments, and relevant observations. The minutes of this monthly meeting must be itemized in the monthly college council meetings. This will enable formative evaluation of COMPETENCY-BASED MEDICAL EDUCATION (CBME) and allow intermediate corrections during the course. The same will be reviewed in quarterly joint college council meetings.
4. Evaluation Phase: The entire roll out plan must be evaluated (formatively and summatively) by Internal Quality Assurance Cell (IQAC), as per the indicators identified in the planning and implementation phase.
5. Amendment Phase: The observations and suggestions of IQAC must be incorporated and aligned planning should be done before implementation.
-
COMPETENCY-BASED MEDICAL EDUCATION (CBME)Roll-out Time line: The entire roll out plan must have well defined deliverables with dedicated timeline as depicted in the GANNT chart for the COMPETENCY-BASED MEDICAL EDUCATION (CBME) launch in 2019 academic year.
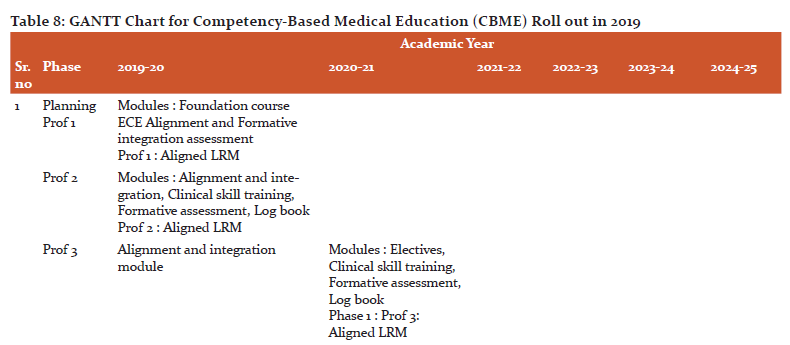
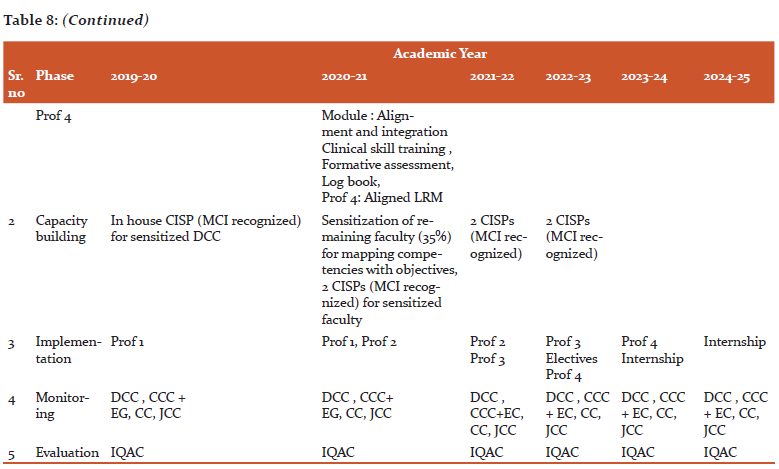
Implication :Implementation of reforms in a phasic manner with capacity building at relevant intervals, as suggested in the model, will provide a steady foundation to the revised curriculum and will ease the process of change.
Conclusion : Any change should be weighed from multiple perspectives.The magnitude of change also defines the amount of input, resources and time. Bigger the change , more will be the time required for planning and leadership support. 4One key aspect involves involving various stakeholders as change agents and appraising them about the benefits of the Change. Competency Based Medical Education is one such change that requires careful planning, diligent implementation and robust monitoring. The proposed rollout plan, with its five distinct phases, can serve as a useful guide for educational leaders at various Medical schools to bring about this change with capacity building at one hand and administrative support at the other. The Interoperable systems that support information flow in number of directions is a hallmark of the proposed plan.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of Interest: Nil
Source of Funding: Nil
References:
-
https://www.mciindia.org/CMS/e-gazette (last accessed on 25th April 2020)
-
Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002;287(2):226-235.
-
Curriculum Implementation Support Program of the Competency Based Undergraduate Medical Education Curriculum, Medical Council of India, 2019
-
Bland CJ, Starnaman S, Wersal L, Moorhead-Rosenberg L, Zonia S, Henry R. Curricular change in medical schools: how to succeed. Acad Med 2000; 75:575-94
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





