IJCRR - 8(9), May, 2016
Pages: 64-67
Date of Publication: 12-May-2016
Print Article
Download XML Download PDF
SQUAMOUS CELL CARCINOMA OF TONGUE - A CASE REPORT AND REVIEW OF LITERATURE
Author: L. Kayal, S. Jayachandran, Y. Hemavathy Bhaskar
Category: Healthcare
Abstract:Oral Squamous cell carcinoma is the most common cancer of the Oral Cavity and it is usually seen in patients above the age of 50 years. It rarely occurs in patients who are less than 30 years old (0.4-5.5%). Diagnosis in advanced stage, misdiagnosis usually lead to inappropriate treatment and delayed definitive treatment. Studies show that nearly 30-40 % of all cancer-related mortality are due to human behaviors such as smoking, consumption of alcohol, poor diet quality and physical inactivity. The morbidity of this malignant neoplasm is low in young patientsonly about 2 % of patients was diagnosed with tongue cancer in patients under the age of 35 years. This case report describes a squamous cell carcinoma, involving anterolateral border of tongue in young adult.
Keywords: Malignant, Neoplasm, Morbidity, Squamous cell carcinoma
Full Text:
INTRODUCTION
Squamous cell carcinoma (SCC) constitute more than 90% of all head and neck cancers. It typically occurs in the elderly men during the fifth-eighth decade of life and rarely occurs in the young patients under the age of 401 . The recent literature has given increasing attention to SCC of tongue in young adults2 . Only approximately 2% of patients are diagnosed before the age of 35 and another 7% before the age of 45, despite the fact that there is an increasing prevalence of tongue SCC3 . Literary reports regarding the etiology, history, and management is limited due to the rarity of this tumor in young patients. Even though tobacco and alcohol abuse is said to be the main etiological factor, it was reported only for a small percentage of patients in some series.
The lack of significant habits in young patients have prompted many to postulate other factors like immune deficiency, genetic factors, and dietary factors in the etiology of cancer. Viruses like herpes simplex virus and human papilloma virus have also been reported as contributing factors.4 Patients in the younger age group were claimed to have a more aggressive disease with a higher incidence of local recurrence or regional lymph node involvement after treatment and a higher mortality rate compared with older patients5 In this paper a young adult male with a chronic non-healing ulcer which turned out to be a SCC is discussed. He had the habit of pan chewing and smoking and sharp teeth in relation to the affected site of the tongue. Case scenario A 29 year male patient reported to the department of oral medicine and radiology with the chief complaint of an ulcer in his tongue for past 6 months.
History revealed he was chronic smoker and pan chewer for past 10 years. Patient was well nourished with BMI 29.5 Kg/m2 .So patient was referred to tobacco cessation center for counselling regarding his habits . During our routine investigation he had a high blood pressure (160/100 mm Hg) and blood sugar level – FBS 111mg/dl, PBS- 181mg/dl. Patient then started taking medication tab, metformin 500mg 1-0-1 for diabetes and tab. Envas 2.5mg 1-0-1 for hypertension.
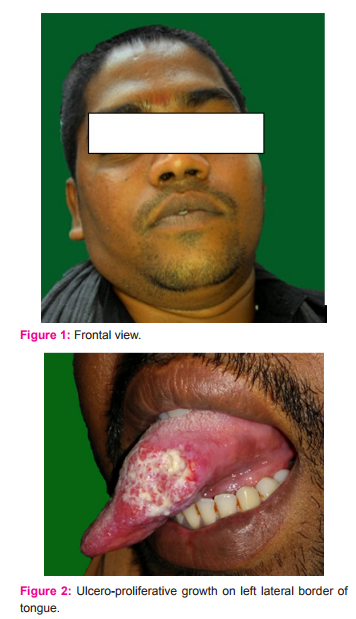
On extra-oral examination, no facial asymmetry was observed and level 2 lymph nodes palpable on left side. On intra-oral examination, an ulcero-proliferative growth was seen in left side of anterior two-third involving lateral border of tongue extending into ventral surface , which measures about 4.5 × 2cm, mixed white and red in colour, surface was granular, and margins were everted. On palpation, the growth bleeds on touch and soft in consistency, base is not indurated.
The presence of sharp cuspal edges in lingual cusp of 35,36 and buccal cusp of 24,25 was also noted in the region of the ulcer causing obvious trauma in the area. Provisional diagnosis of malignant ulcer with clinical staging of the tumour T3N1M0 was given and chair side investigation was carried away by applying toluidine blue stain which stained malignant cells and also helped in selecting biopsy site , laterincisional biopsy was performed under Local anaesthesia.
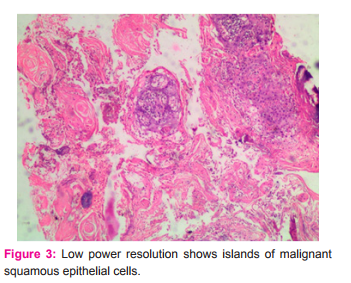

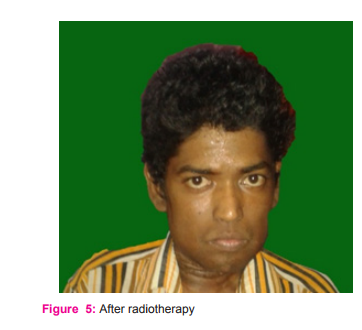
Histopathology revealed islands of malignant squamous epithelial cells with keratin differentiation in connective tissue stroma and result was well differentiated squamous cell carcinoma. CT scan revealed evidence of subtle soft tissue thickening of size 20.6 cm and minimal contrast enhancement on left lateral border of tongue and evidence of no lymph node enlargement Patient was then referred to department of surgical oncology, Royapettah govt. hospital for treatment, which consisted of modified unilateral radical neck dissection and wide local excision. After surgery, radiotherapy of 2Gy for 5 days/week for 5 weeks period. After RT patient has lost weight and his BMI is 20 kg/m2 . Despite radical neck dissection followed by radiotherapy , patient was comfortable for one month and again there was relapse, for which chemotherapy was advised. Patient had tab. Cisplastin 100mg once in 3week for 3 cycles of chemotherapy. Patient became thin and very ill, unable to walk. From the reports of the relatives of the patient we came to know that the patient died after 5months.
DISCUSSION SCC in young adults arerare. Tongue cancer has a male predominance and occurs in 6-8th decade of life after long term exposure to cigarette smoke and alcohol abuse. Tobacco use and alcohol consumption are not only risk factors for oral cancinoma but there also strong effects on patient morbidity, recurrence and second primary tumour and mortality6 . Chronic mechanical trauma due to sharp teeth, under fillings, badly fitting dentures in the etiology of oral squamous cell carcinoma has been reported in literature In the present case, patient was chronic smoker and pan chewer which has a significant adverse effect on survival7 Though environmental exposure to tobacco and other carcinogens are important factors for cancer, it is now well documented that other factors such as diet have play an important role in the carcinogenesis process. Several dietary factors act as risk modifiers. In general, dietary deficiencies have not been shown to initiate events, but epidemiological and experimental studies provided strong evidence for dietary substance, in promotion, progression and inhibition of cancer8 .In the present report also due to dietary deficiencies patient become immaciated which might be a factors for his death.
Dental health care workers are a largely untapped resource for providing advice, educate and brief counseling to tobacco-using patients, and there are good reasons to believe that they can be effective in this role. Here in this case report , our patient underwent tobacco cessation counselling9 . Friedlander et al , in a study of younger and older (6oyrs) patients with tongue cancer matched for alcohol and tobacco usage and other factors, found no difference in survival, although younger group of patients had a higher incidence of local regional recurrence1 . Kuriakose et al found that in young patients the cancer was more aggressive with an invasive pattern and prognosis was poor in early stage of disease compared to older patients10. In diabetic patients, alterations occur in the oxidative equilibrium of free radicals.
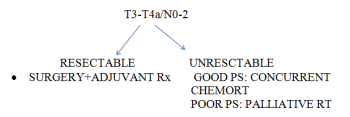
Increased consumption of saturated fats increases the risk of diabetes mellitus, but recently it has been suggested that it also increases the risk of oral cancer11 Treatment of squamous cell carcinoma of tongue remains mainly surgery, with adjuvant radiotherapy added for advanced stage disease or in patients at risk of local regional failure. The achievement of clear resection margin is important because survival is closely related to resection regardless of any subsequent therapy the patients may receive12. In the present case, tumour removed with 1cm clearance followed by adjuvant radiotherapy.
Metastatic spread of squamous cell carcinoma of tongue is facilitated by the tongue’s rich lymphatic network, which tends to increase with the size of the primary tumour. Approximately 50% of tongue cancers present with lymph node involvement. Lymph node metastasis is a well known negative prognostic factor for squamous cell carcinoma of tongue, and it decreases the survival rate by 50%12. Studies have shown that survival rates in men are lower than women with tongue cancer13.It is well documented that the incidence of local recurrence is higher with positive histological resection margin compared with negative histological resection margin in head and neck cancer14.The reported incidence of local recurrence rates in the margin ranged from 29% - 70% and were 4%-38% for negative resection margins15.
CONCLUSION Oral cancer occurring in young adult is uncommon but nevertheless should always considered such patients present with sharp tooth will produce ulceration particularly in the high-risk sites of the tongue. Several studies suggested that oral cancer in younger patients is inherently more aggressive with a worse prognosis than the disease in older individual. By prompt diagnosis and treatment stratergies the life span of these patients may be prolonged further.
References:
1. Friedlander PL, Schantz SP, Shaha AR, Yu G, Shah JP : Squamous cell carcinoma of the tongue in young patients: A matchedpair analysis. Head Neck 1998;20:363-368.
2. Myers JN, Elkins T, Roberts D, Byers RM. Squamous cell carcinoma of the tongue in young adults: Increasing incidence and factors that predict treatment outcomes :Head Neck Surg 2000; 122: 44-51.
3. Aleksandra Crede, Michael Locher and Marius Bredell : Tongue cancer in young patients: case report of a 26-year-old patient. Head and Neck Oncology 2012, 4:20.
4. Elizabeth Mathew Iype, Manoj Pandey, AleyammaMathewy, Gigi Thomasz, Paul Sebastian and Madhavan Krishnan Nair : Squamous Cell Carcinoma of the Tongue Among Young Indian Adults: Neoplasia . Vol. 3, No. 4, 2001, pp. 273–277
5. Sarkaria J N, Harari P M. Oral tongue cancer in young adults less than 40 years of age: rationale for aggressive therapy. Head And Neck 1994; 16: 107-111.
6. G. Bachar, R. Hod, D.P. Goldstein, J.C. Irish, P.J. Gullane, D. Brown, R.W.Gilbert, T.Hadar, R. Feinmesser, T. Shpitzer: outcome of oral tongue squamous cell carcinoma in patients with and without known risk factors. Oral oncology 47(2011) 45-50.
7. Orbak R, Bayraktar C, Kavrut F, Gundogdu C. Poor oral hygiene and dental trauma as the precipitating factors of squamous cell carcinoma. Oral Oncol 2005;41:109–13.
8. MPR. Prasad, TP Krishna, S Pasricha, MA Quereshi, K Krishnaswamy:Diet and oral cancer - a case control study:Asia pacific j clinnutr(1995) 4: 259-264.
9. PavanUdayPatil , S Vivek , Thatimatla Chandrasekhar, NaliniParimi , B H Praveen , Sunil Lingaraj: Patient Receptivity to Tobacco Cessation Counseling and Services in a Dental Teaching Institute: A Patient Review: Journal of International Oral Health 2015; 7(1):1-4).
10. Kuriakose M, Sankara Narayanan M, Nair MK et al.: comparison of oral squamous cell carcinoma in younger and older patients in India. Eur J cancer B Oral Oncol 1992: 288: 113-20.:
11. AjitAuluck : Diabetes Mellitus: An Emerging Risk Factor for Oral Cancer?: JCDA: July/August 2007, Vol. 73, No. 6.
12. Mildasuslu MD, Ali sefikHosal MD, TugbaAslan MD, BulentSozeri MD, and Anil Dolgunphd : carcinoma of the oral tongue : a case series analysis of prognostic factors and surgical outcomes: J Oral maxillofacsurg 71: 1283-1290, 2013.
13. BerrinoF ,Gatta G: variation in survival of patients with head and neck cancer in Europe by the site of origin of tumours. Eurocare Working Group. Eur J cancer 34:2154, 1998.
14. Po Wing Yuen, FRCS, FACS, King Yin Lam, FRCPA, Alexander Chak Lam Chan, FRCPA, William Ignace Wei, FRCS, FACS, Lai Kun Lam, FRCS, Hong Kong: Clinicopathological Analysis of Local Spread of Carcinoma of the Tongue: Am J Surg. 1998;175:242–244. © 1998.
15. Zieske LA, Johnson JT, Myers EN, Theale PB. Squamous cell carcinoma with positive margins. Arch Otolaryngol Head Neck Surg. 1986;112:863–866.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





