IJCRR - 8(9), May, 2016
Pages: 45-47
Date of Publication: 12-May-2017
Print Article
Download XML Download PDF
MORPHOLOGICAL STUDY OF THE TIBIAL TUBEROSITY IN THE POPULATION OF SOUTH KARNATAKA, INDIA
Author: Rashmi Bhat, Ramya Rathan, Neha Samapriya, Shakuntala Pai
Category: Healthcare
Abstract:Objective: To estimate the prevalence of various morphological types of Tibial Tuberosity and to determine the side and gender differences.
Methods: 170 randomly collected tibiae of unknown sex were analysed to evaluate the shapes and the gender differences in the tibia. The prominence of the Tibial Tuberosity and the gender differences of the bone was determined
Results: Type 2 TT was the most common type seen in 34% bones followed by type 3 in 17% of the bones. Type 2 TT was the most common type seen on right side (31%) as well as on the left side (39%). Type 2 was the most common type of TT seen in both males (32%) and females (35%).
Conclusion: The present study shows variations in shape may be due to developmental reasons. There were no statistical differences in the side and gender differences. The knowledge of the present study will help further researchers in evaluating anterior knee pain syndromes.
Keywords: Tibia, Tibial Tuberosity, Shape, Gender
Full Text:
INTRODUCTION
The Tibial tuberosity(TT) is a bony landmark present at the proximal end of the tibia. It is one of the bony points to measure the Quadriceps angle (Q angle) for assessing patellofemoral mechanics. The TT is an apophysis and develops in traction.1 Development of the tubercle has been divided into four stages: cartilaginous, apophyseal, epiphyseal, and bony.2 The TT begins ossification at between seven and nine years as a distal focus. This progressively enlarges proximally and anteriorly, while the proximal tibial epiphysis concomitantly expands downward into the tuberosity.3 The TT projects only a little and is divided into distal rough and a proximal smooth region. The patellar tendon is attached to the proximal smooth area while the distal end is palpable.4 The morphology of the TT has received scant attention by researchers. Variations in the morphology of the TT could cause errors in determining its precise location. The shape and the position of the TT influences the value of the Q angle and also has impact on patellofemoral biomechanics. According to Van Eijdn et al(1987)5 ,a TT which is anteriorly placed increases the length of the contact paths on both patellar and femoral articulating surfaces, produces a lengthening of the moment arm of the patellar ligament force which may either decrease or increase the ratio between patellar ligament force and quadriceps muscle force.5 An abnormal lateral position of the TT causes distal malalignment of the extensor mechanism of the knee and can lead to lateral tracking of the patella which causes anterior knee pain or objective patellar instability and is mainly characterised by recurrent dislocation.( Koetar S et al, 2007)6. The methods used to determine the position of the TT include clinical assessment7 , conventional radiography using marking wires8 and CT scan.6,7,8,9,10 Of these methods, measurements done on CT scans appear to be the most reliable.6 However, a survey of the literature did not reveal any study that used direct bony measurements. This information is likely to be useful to the clinician in evaluating anterior knee pain syndromes. With reference to the above literature the main objective of the current study is to estimate the prevalence of various morphological types of TT and to determine the side and gender differences.
MATERIALS AND METHODS
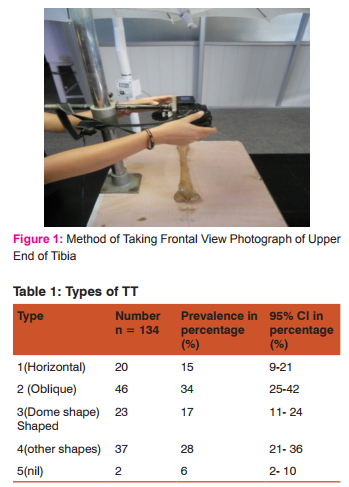
The material for the present study comprised of one hundred and seventy adult human tibia bones. The tibias were collected from the department of Anatomy from various Medical colleges in the Southern region of Karnataka. 170 tibiae were studied of which 101 belonged to right side and 69 to left side. The bones were first selected by using inclusion criteria and were numbered. The Prominence of the TT was assessed by analysing the end on frontal view photos with Adobe Photoshop version 5.0 (vide infra).
SUBJECTIVE SEXING OF THE TIBIA: was done to determine the gender differences in the above measurements. The criteria used were
• Weight and the length: measured by Electronic balance and Osteometric Board
• Mid-shaft circumference: First, the midpoint of the total length of tibia was marked. Then the midshaft circumference was measured using measuring tape.
• Width at the proximal and distal end: Were measured using digital callipers at the widest region.
• Minimum girth of the shaft: measured at the junction of middle and lower third using measuring tape.
• The bones were then classified as males or females using the demarking points given by Singh and Singh et al.11
RESULTS
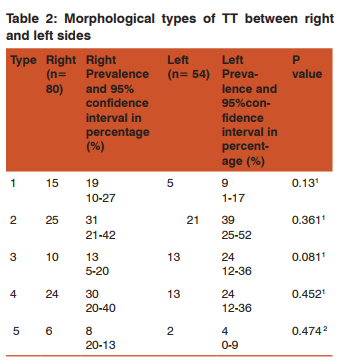
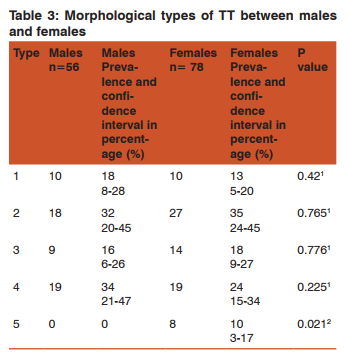
The TT was classified into 5 types based on the shape of the ridge separating the proximal and distal parts of TT. The prevalence of the 5 types of TT is shown in table 1. Type 2 TT was the most common type seen in 34% bones followed by type 3 in 17% of the bones. Type 5 TT was the least common type. Table 2 shows that Type 2 TT was the most common type seen on right side (31%) as well as on the left side (39%). Type 1 was seen to be more common on right side than on left and type 3 was more common on the left side than on the right, however both were not statistically significant. Type 5 TT was the least common type. Type 2 was the most common type of TT seen in both males (32%) and females (35%) and is present in table 3. It’s of interest to note that a ridge on TT was always present in male tibiae when compared to female tibiae which was statistically significant.
DISCUSSION
In review of literature it was noticed that there are no documented works on classification of TT based on shape of the ridge separating the proximal and distal parts of TT. Hence, comparison with other studies could not be done. This ridge across the TT marks the distal limit of the proximal tibial growth plate.3 In the present study it was noticed that the oblique shape of the ridge was most common (34%) while absence of ridge on TT was the least common (6%). This suggests that the shape of the ridge is influenced by the proximal epiphyseal pull. When analysed for side differences it was observed that that there was no significant difference between the right and left in the prevalence of morphological types of TT. If paired right and left tibia of the same cadaver were available this difference could have been analysed better. Gender difference in the morphological types of TT was further analysed. For this purpose the subjective classification of the tibia according to various parameters was done. It was noted that there was no significant difference. Of interest here to note is the constant presence of the ridge on the TT in male tibiae where as about 10% of female tibiae lacked this ridge suggesting the differential amount of force applied to this proximal epiphyseal plate in males and females. The difference was statistically significant.
CONCLUSION
The present study shows variations in shape may be due to developmental reasons. There was no statistical differences in the side and gender. The present study will help further researchers in evaluating anterior knee pain syndromes.
AKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Source of funding: NIL Conflict of Interest: NIL.
References:
1. Ogden JA, Southwick WO. Osgood–Schlatter’s disease and tibial tuberosity development. Clin Orthop Relat Res 1976; 116:180–189.
2. Ehrenborg G, Engfeldt B. The insertion of the ligamentum patellae on the tibial tuberosity. Some views in connection with the Osgood–Schlatter lesion. Acta Chir Scand 1961; 121:491–499.
3. Ogden JA. Radiology of postnatal skeletal development. X. Patella and tibial tuberosity. Skeletal Radiol 1984; 11(4): 246-57.
4. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC et al, editors. Gray’s anatomy: The Anatomical basis of clinical practice. 40th ed. UK, Elsevier Ltd; 2008. p. 1412-15.
5. Van Eijden TMGJ, Kouwenhoven E and Weijs WA. The influence of anterior displacement of the TT on patellofemoral biomechanics. International Orthopaedics.1987; 11(3): 215-221.
6. Koetar S, Diks MJ, Anderson PG, Wymenga AB. A modified tibial tubercle osteotomy for patellar maltracking: result at two years. J Bone Joint Surg Br. 2007 Feb; 89(2): 180-5.
7. Shakespeare D, Fick D. Patellar instability- canthe TT-TG distance be measured clinically? Knee. 2005 Jun; 12(3): 201-4.
8. Nagamine R, Miura H, Urabe K, Matsuda S, Chen WJ, Matsunobu T. Radiological assessment of the position of the tibial tuberosity by means of a marking in knees with patellofemoral arthritis. Skeletal radiol. 1999 Jan; 28(1): 27-32.
9. P. Schoettle, M. Zanetti, B. Seifert, C. Pfirrmann, S. Fucentese, J. Romero. The tibial tuberosity–trochlear groove distance; a comparative study between CT and MRI scanning. The Knee.2006 ;13(1): 26-31.
10. Jones RB, Barlett EC, Vainright JR, Carroll RG. CT determination of tibial tubercle lateralization in patients presenting with anterior knee pain. Skeletal Radiol. 1995 Oct; 24(7): 505-9.
11. Singh G, Singh S, Singh SP. Identification of sex from tibia. J Anat Soc India 1975;24(1).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





