IJCRR - 11(8), April, 2019
Pages: 01-07
Date of Publication: 30-Apr-2019
Print Article
Download XML Download PDF
The Malignant Round Cell Tumors: Histopathological Study and Immunohistochemistry
Author: Meghavi R. Joshi, Dhaval Jetly, Mital Kundariya
Category: Healthcare
Abstract:Malignant round cell tumors include a diverse group of cancers that appear morphologically as round cells. More commonly malignant round cell tumors include cancers consisting of small to intermediate cells having a dark, hyper chromatic nuclei and scant or indistinct cytoplasm. These malignant blue cell tumors include: Primitive neuroectodermal tumor (PNET)/Ewing's sarcoma family, Neuroblastoma, Non-Hodgkin's lymphoma, Rhabdomayosarcoma, Wilms tumor, Retinoblastoma, Small cell osteosarcoma, Medulloblastoma, Desmoplastic round cell tumor, Mesenchymal chondrosarcoma and Merkel cell carcinoma.
Aims & Objectives:
1. To study Histopathology of Malignant small round cell Tumors.
2. To correlate Histopathological findings with Clinical features, physical findings and imaging studies.
3. To study importance of Immunohistochemistry profiles in Malignant small round cell tumors.
Materials & Methods: This is the prospective study and 100 consecutive cases of Malignant round cell tumor received from data of department of pathology during period from 2014 to 2017 were studied. Histological parameters were studied on biopsy fixed in 10% neutral formalin, embedded in paraffin wax and stained with hematoxyline &eosin. IHC stains were performed on each cases.
Results: Out of 100 cases, there were 36 cases of Ewing sarcoma/PNET with highest incidence (36%) 21 Cases of Neuroblastoma(21%),15 cases of Non-Hodgkin's lymphoma (15%). According to age distribution, the highest incidence was observed in 0-14 years of age group. According to sex distribution, highest incidence observed in males. IHC study in Ewing sarcoma /PNET and Neuroblastoma shows positive reaction with CD 99, vimentin and NSE, NB, S100, synaptophysin, chromogranin respectively. IHC study of NHL showing majority are T cell lymphoblastic lymphoma. IHC study of Rhabdomyosarcoma shows positive reaction with desmin, myoD1, Myoglobin, vimentin.
Conclusion: Most frequent round cell tumors are Ewing sarcoma /PNET , Neuroblastoma, Non-Hodgkin's lymphoma, Rhabdomyosarcoma, Wilms tumor, Retinoblastoma. Malignant round cell tumors have male predominance and presented in early childhood. This study highlights the importance of histological examination of resected specimen or biopsied tumors. IHC represents a tool that can provide a clear distinction among the various tumor types.
Keywords: Small blue round cell tumors, Ewing sarcoma/PNET, Primitive tumors, Childhood undifferentiated tumor
Full Text:
INTRODUCTION
Malignant round cell tumors include a diverse group of cancers that appear morphologically as round cells. These may be large undifferentiated malignant neoplasms. More commonly malignant round cell tumors include cancers consisting of small to intermediate cells having a dark, hyper chromatic nuclei and scant or indistinct cytoplasm.
These malignant blue cell tumors include: Primitive neuroectodermal tumor (PNET)/Ewing’s sarcoma family, Neuroblastoma, Non-Hodgkin’s lymphoma, Rhabdomayosarcoma , Wilms tumor, Retinoblastoma, Small cell osteosarcoma, Medulloblastoma, Desmoplastic round cell tumor, Hepatoblastoma –[anaplastic form only], Mesenchymal chondrosarcoma, Merkel cell carcinoma. 1
In Malignant round cell tumors, this task is difficult because of similar morphological appearances in histopathology. Through the identification of specific cellular components, using specific monoclonal or polyclonal antibodies, Immunohistochemistry (IHC) has emerged as the most practical adjunct tool to the histopathology making accurate diagnosis possible.9
AIMS & OBJECTIVES
-
To study Histopathology of Malignant small round cell Tumors.
-
To correlate Histopathological findings with Clinical features, physical findings and imaging studies.
-
To study importance of Immunohistochemistry profiles in malignant small round cell tumors.
MATERIALS & METHODS
Patients diagnosed in our institute as Malignant round cell tumor were selected. This is the prospective study and 100 consecutive cases of Malignant round cell tumor received from data of department of pathology during period from 2014 to 2017 were studied. Clinical finding of patient was obtained by patient’s medical records, relevant clinical history, laboratory investigation and Radiological finding.
Histological parameters were studied on biopsy fixed in 10% neutral formalin, embedded in paraffin wax and stained with hematoxyline &eosin .Examine for Architecture and pattern of tumor cells, morphology of cells with nuclear and cytoplasmic characteristics, Presence of mitosis, Hemorrhage, Necrosis or Calcification, any extracellular materials in Stroma, Presence or Absence of Rosettes or Pseudo rosettes. After microscopic examination of routinely stained section followed by special stain [PAS], diagnosis is formulated.
IHC stains were performed on biopsy section and IHC was performed on tissue block from each cases using ABC technique with antigen epitope enhancement by heat, the diaminobenzidine reaction was used as final detection step. The slides were counter stained with Mayer’s hematoxylin. The method for epitope retrieval was overnight incubation at 60 degree Celsius. After antigenic epitope enhancement the staining was performed by fully automated machine VENTANA BENCHMARK XT. Appropriate positive and negative controls were included in all stains to ensure quality and consistency of staining results.
RESULTS AND OBSERVATION
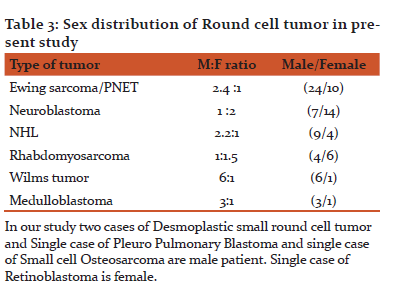
The Malignant small round cell tumors are a heterogeneous group of malignant neoplasms. Most higher incidence noted in our study is Ewing sarcoma /PNET (36%) followed by Neuroblastoma(21%), Non-Hodgkin’s lymphoma (15%) and other small round cell tumor as shows in table no1. These tumors occurs mainly in children up to 14 years of age. Most of the Neuroblastomas &Nephroblastomas (Wilms tumor) appeared in the age group of less than 5 years whereas majority of other Small Round Cell Tumors appeared after the age of 5 years (table 2). Male predominance seen in these tumors. (Table 3).
Histopathological features:
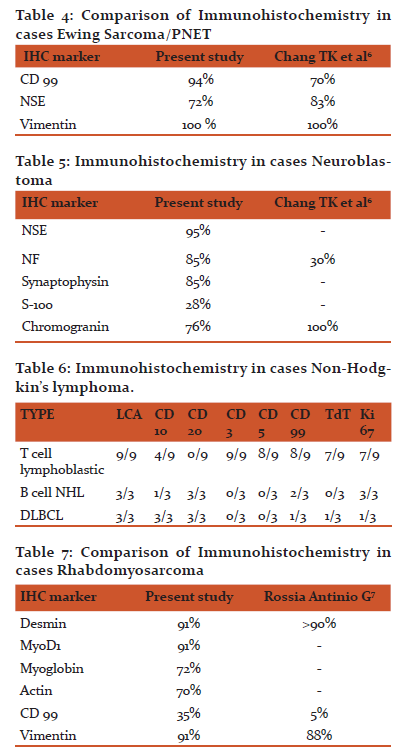
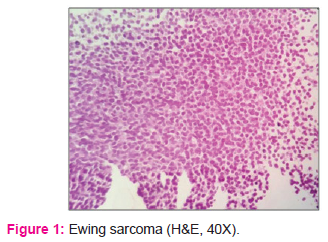
36 cases of Ewing sarcoma / PNET showing Diffuse sheet or lobular pattern of cells, these cells are small, round to oval with fine to vesicular chromatin with occasional nucleoli with scanty cytoplasm or some having vacuolated due to glycogen deposition ,with variability in mitosis, necrosis. IHC shows positive reaction as in Table 4.
21 cases of Neuroblastoma showing diffusely arranged small round to oval cell with salt and pepper chromatin with occasional nucleoli, scanty cytoplasm with variable necrosis and rosettes formation and three cases having ganglionic differentiation. IHC shows positive reaction as in Table 5.
9 out of 15 cases of Non-Hodgkin’s lymphoma showing T cell lymphoblastic lymphoma, 3 cases of B cell lymphoblastic lymphoma and 3 cases evaluated as DLBCL by IHC. Table 6.
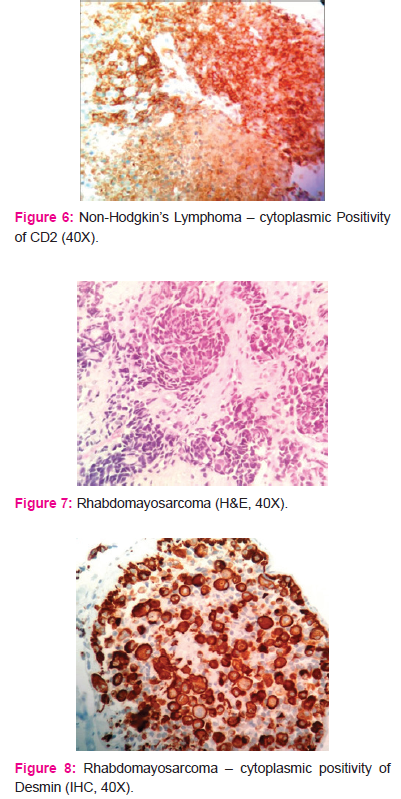
Out of 11 cases of Rhabdomyosarcoma 8 cases shows histological features of Embronal type and 3 cases shows alveolar type Rhabdomyosarcoma. IHC shows positive reaction as in Table 7.
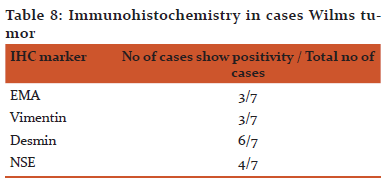
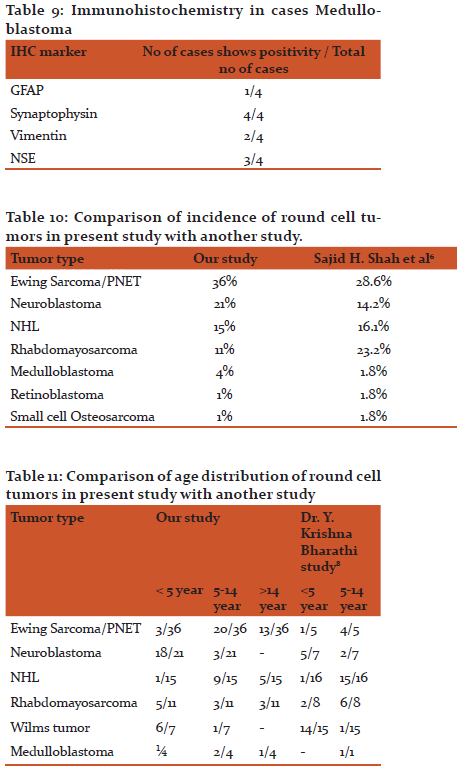
7 Cases of wilms showing microscopically blastemal cells are arranged in nests diffuse sheets, tubules surrounded by mesenchymal cells. These cells are small round with hyper chromatic nuclei, inconspicuous nucleoli with scanty cytoplasm, with variable mitosis and necrosis.IHC shows positive reaction as in Table 8.
All cases of Medulloblastoma showing sheets of small round cells with scanty cytoplasm, hyper chromatic nuclei often elongated or carrot shaped. Mitosis seen. IHC shows positive reaction as in Table 9.
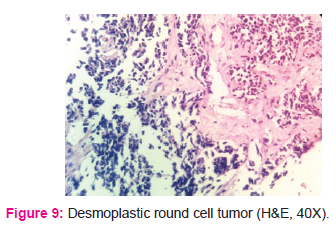
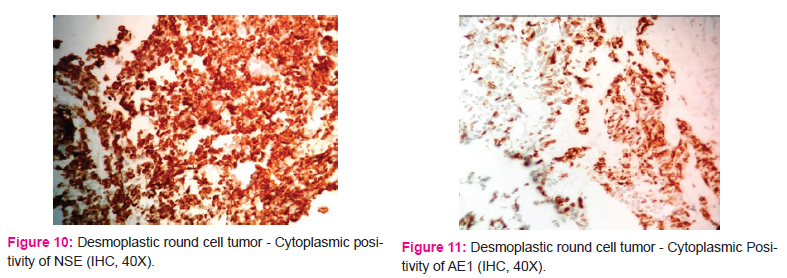
There are 2 cases of desmoplastic small round cell tumor shows solid nests of round to oval cells surrounded by cellular desmoplastic stroma. Necrosis is seen. Both cases of DSRCT showing immunoreactivity with AE1, Desmin, vimentin, and NSE. [Figure10, 11]
One case of Retinoblastoma showing microscopically sheets and nests of small round cells with scanty cytoplasm, hyper chromatic nuclei. Flexner winter steiner rosettes seen.IHC shows positivity with NSE, Synaptophysin, and S100.
One case of pleuropulmonary blastoma microscopically showing cyst wall lining and tumor cells are beneath to lining epithelium. Tumor cells are round to spindled hyper chromatic nuclei. Focal area of necrosis is seen. IHC shows positivity with Vimentin, Desmin, CD117, Ki-67 (high 85%), CD99 (weak)
One case of Small cell OS showing diffusely arranged small round to spindly cells, focal area of malignant osteoid seen. IHC shows positivity with Vimentin and S100. Negative for CD99, EMA, LCA, Desmin, Synaptophysin.
Discussion
Malignant Small round cell tumors comprise a significant fraction of pediatric tumors. Malignant Small Round Cell Tumors is the name given to a group of malignant neoplasms that occur mostly in the pediatric age group (up to 14 Yrs.) These tumors show characteristic appearance under the microscope, consist of Small Round Cells that Stain Blue on routine Haematoxylin and Eosin stain. 1
Incidence of SBRCT is on rise all over the world 2 Over 60% of all childhood MRCT are now curable.3 In present study out of 100 cases 76 cases are in pediatric age group below 14 years.
Distribution of types of tumor in our study compared with other study. Result shows some variation as in Sajid H. Shah5 study 12.5% cases have inconclusive results so not categorized to specific type, however in our study one cases is inconclusive and we also encounter one case of Pleuropulmonary blastoma and two cases of DSRCT .(Table 10)
In our study Most of the Neuroblastomas and Wilms Tumor appeared in the age group of less than 5 years whereas majority of other malignant round cell tumor appeared after the age of 5 years, similar to Dr. Y. Krishna Bharathi study of 56 cases round cell tumors in pediatric age group 8.(table 11)
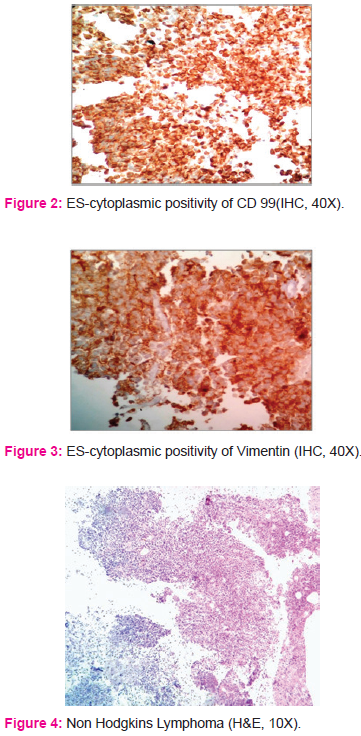
As shown in our results, ES/PNET is the most common MSRCT. The tumor cells show cytoplasmic immunoreactivity to vimentin and membranous immunoreactivity to CD99. CD45 was negative which ruled out lymphoma. Immunohistochemically, strong membrane staining for CD99 is consistently seen in almost all cases of EWS/PNET, although it is not very specific because it is shown in several other soft tissue sarcomas and lymphoblastic lymphomas.
Twenty one case of Neuroblastoma which showed cytoplasmic positivity for Synaptophysin and Chromogranin and NSE. Absence of positive staining for CD99 and CD45 was helpful in differentiating it from EWS/PNET and lymphoma. The markers synaptophysin, and chromogranin and CD56 are restricted to neuroendocrine neoplasms; nevertheless, it should be reemphasized that they are seen in only 30-50% of cases. Neuroblastoma shows immunoreactivity with, Synaptophysin, chromogranin, NSE and CD56.Tumor cells usually do not react with vimentin, CD99, actin or desmin.
In present study T-LBL is more compared to those with B-LBL. T-LBL constituting 60% of all lymphoma cases. These cases show younger age, a higher rate of mediastinal mass.
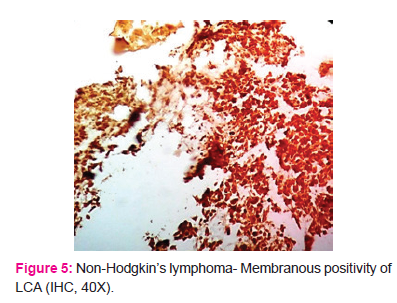
IHC was performed in all cases of suspected NHL. The tumor cells show cytoplasmic and membranous immunoreactivity to CD45. Cytokeratin (CK) was negative which excluded poorly differentiated and undifferentiated carcinomas. CD45 is a surface antigen expressed by virtually all hematolymphoid proliferations, and monoclonal antibodies for this marker are reliably specific.
We found three cases of Rhabdomyosarcoma which showed cytoplasmic immunoreactivity for vimentin, desmin and CD99, hence subcategorized as alveolar rhabdomyosarcoma. Rhabdomyosarcoma express skeletal muscle markers, like desmin, myoD1, myogenin and CD99 (the alveolar type).
Single cases of Retinoblastoma of eye, presented as a big mass involving the eye and extending to the periorbital region. On H&E examination it presented as malignant round cell tumor with rosette formation but for definite diagnosis IHC needed.
Four cases of Medulloblastoma were diagnosed in the cerebellum in which tumor cells were so undifferentiated in morphology that making the differentiation from Glioblastoma multiforme (GM), PNET, and metastatic carcinoma very difficult. IHC solved the problem and diagnosis was given in these cases.
Two Abdominal DSRCT cases, One case of Pleuropulmonary blastoma and One case of Small cell Osteosarcoma the diagnosis was given by extensive panel of antibody given on IHC. In only single case IHC is inconclusive even by extensive panel of antibody so given as Undifferentiated Malignant Round Cell Tumor. Immunohistochemistry is playing an increasing role in modern surgical Histopathology.3 The use of extensive panels of antibodies in all Malignant Round Cell Tumors allows accurate histological diagnosis in more than 95% cases.
Conclusion
The MRCTs are a heterogeneous group of malignant neoplasms. It occurs mainly in children up to 14 years of age. Most of the Neuroblastomas &Nephroblastomas (Wilms tumor) appeared in the age group of less than 5 years whereas majority of other Small Round Cell Tumors appeared after the age of 5 years. Male predominance seen in these tumors.
Histopathological examination forms the basis for diagnosis of MRCT in the form of features like Small Blue Round Cells with scanty cytoplasm along with specific characteristics like Rosettes, Pseudo rosettes and Neurophils that helps to differentiate the entities of MRCTs. Special stain like PAS is also helpful for diagnosis of ES/PNET family of tumors by positive staining for glycogen.
After the Histopathological diagnosis of typing of MRCTs, IHC has to be done in each and every case. IHC represents a tool that can provide a clear distinction among the various tumor types to ensure appropriate and specific treatment. This study highlights the importance of histological examination of resected specimen or biopsied tumors. However, IHC confirms the final diagnosis and also helpful to know the Prognosis of tumor. In Recent years, role of molecular genetic studies has proved its role as a valuable tool for definitive diagnosis in questionable cases.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature of article has been reviewed and discussed.

References:
-
Gregario A, Corrias et.al (July,2008)”Small blue round cell tumors”: Diagnostic& prognostic usefulness of surface molecule”. Histopathology 53 (1):73-80. doi:10.111/j.1365-2559. 2008.
-
Arya L.S. Childhood cancer-challenges and opportunities. Indian j.of paediatrics.2003;70:159-62.
-
Wick MR. Immunohistochemical approaches to the diagnosis of undifferentiated malignant tumors. Ann Diagn Pathol 2008;12:72-84.
-
Chan JK. Advances in immunohistochemistry: Impact on surgical pathology practice. Semin Diagn Pathol 2000;17:170–7.
-
Sajid hussain shah et al.Frequency of malignant solid tumors in children, JPMA March 2000.
-
Chang TK,LI CY ,Smithson WA. Immunohistochemical study of small round cell tumors in routinely processed specimen.Archpathol lab med 1989;113(12):1343-8.
-
Rossia Antinio G, Nascimentob,Fabio Canala, Angelo Paolo Dei Tosa. Review :Small Round Cell Neoplasm of Soft Tissues: An Integrated diagnostic approach. Current Diagnostic pathology:2007,13150-163
-
Dr. Y. Krishna Bharathi, Study of pediatric small blue round cell tumors with immunohistochemical correlation IOSR Journal of Dental and Medical Sciences 2279-0853,Volume 15,Issue 6 ,June 2006.
-
Kurtin PJ, Pinkus GS. Leukocyte common antigen-a diagnostic discriminant between hematopoietic and nonhematopoietic neoplasms in paraffin sections using monoclonal antibodies: Correlation with immunologic studies and ultrastructural localization. Hum Pathol 1985;16:353-65.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





