IJCRR - 11(3), February, 2019
Pages: 09-13
Date of Publication: 07-Feb-2019
Print Article
Download XML Download PDF
Dental findings in Fanconi Bickel Syndrome: Case Report
Author: Jomaa Nermine, Ben Brahim Meriam, Bourguiba Emna, Jemmali Badiaa
Category: Healthcare
Abstract:Introduction: Fanconi-Bickel syndrome is an extremely rare disorder characterized by glycogen accumulation and generalized dysfunction of renal proximal tubules. It was first described by Fanconi and Bickel in 1949. This disease is caused by a defective monosaccharide transporter Glut2. Polyuria, metabolic acidosis, recurrent episodes of severe hypoglycemia, growth retardation, hepatomegaly, and rickets or osteomalacy are clinical consequences of this disease. However, a little information describing the dental and the orofacial signs and symptoms of this abnormality are available. Thus, the aim of this paper was to present the orofacial manifestations and dental management in a girl with Fanconi's syndrome.
Case Report: In this paper, we report a dental findings in a case of 8-year-old girl with the Fanconi-Bickel syndrome who was referred to the Oral Medicine Department of La Rabta hospital (Tunisia). She suffered from many oral manifestations includes delayed development of dentition, opaque areas (hypocalcification), rapidly progressive periodontal disease and premature loss of temporary teeth, as well as general abnormalities.
Conclusion: Through this observation, we conclude that the knowledge of craniofacial features and various dental abnormalities helps dentist to discover underlying systemic disease or syndrome. Thus reducing the morbidity of disease and improving the quality of life. Also, this case makes us thinking that an oral evaluation should be performed in all patients with Fanconi Bickel Syndrome.
Keywords: Fanconi-Bickel syndrome, Hypophosphatemic rickets, Delayed eruption, Taurodontism, Premature loss
Full Text:
Introduction
Fanconi-Bickel syndrome is an extremely rare disorder characterized by the accumulation of a substance called glycogen in different parts of the body.[1] It was first described by Fanconi and Bickel in 1949.[2]Until now, the prevalence is unknown but less than 200 cases have been described in the literature.[1]The mutations in Glut2 is incriminated in the development of this syndrome.[3] The gene for the glucose transporter protein 2 is expressed in liver, pancreas, intestine and kidney.[3] While, The Fanconi-Bickel syndrome can be referred as idiopathic, sporadic, or primary when no identifiable secondary cause is recognized.[4] As regards the mode of transmission, autosomal dominant, recessive, or X-linked trait were reported. [4,5]
This disorder is characterized by hepatorenal glycogen accumulation and general dysfunction of renal proximal tubules.[3] Different to other types of glycogen storage disease caused by enzymatic defects of glycogenolysis, Fanconi-Bickel syndrome caused by a defective monosaccharide transporter, Glut2, in cell membranes of different tissues.[6] The proximal renal tubular dysfunction provoke glycosuria with normal serum glucose levels and urinary loss of bicarbonate, phosphate, potassium, amino acids, and low molecular weight proteins. [7]
Polyuria, metabolic acidosis, recurrent episodes of severe hypoglycemia, growth retardation, hepatomegaly, and rickets or osteomalacy are clinical consequences of the disease.[7] A brain damage and convulsions which are the result of hypoglycemia are also a consequences of this disease.[8] Besides, a facial and truncal adiposity, hyperlipidemia and bleeding tendency, which is related to impaired platelet function, can be present on the patients. [8]
However, a little information describing the dental and the orofacial signs and symptoms of this abnormality are available.[9] In fact, dental findings of Fanconi’s syndrome have been described as a similar to these in hypophosphatemic vitamin D-resistant rickets.[9]
Thus, the aim of this paper was to present the orofacial manifestations and dental management in a girl with Fanconi’s syndrome.
Case report
Medical history
A 8-year-old girl with Fanconi-Bickel syndrome whose condition was first diagnosed when she was 20 months of age. She was referred to the Department of Oral Medicine, LA RABTA hospital (Tunisia) for the evaluation of her dental growth and development.
The patient was the third child of a healthy parent, without the notion of consanguineous marriage. The other children are healthy also.
Physical examination revealed a short stature with a height of 122 cm and weighed about 20 kg, bone deformities, protuberant abdomen and growth retardation.
Laboratory revealed hypocalcemia (65 mg/L), hypophosphatemia(14 mg/L), and Hyperlipidemia ( Triglycerides 2.02 g/L).
The proximal renal tubular dysfunction is expressed by glucosuria, generalized aminoaciduria, bicarbonate wasting, and hypophosphatemia.
Then, laboratory investigations confirmed severe hypophosphatemic rickets.
Dental findings
The patient was submitted to clinical evaluation and radiographic examination.
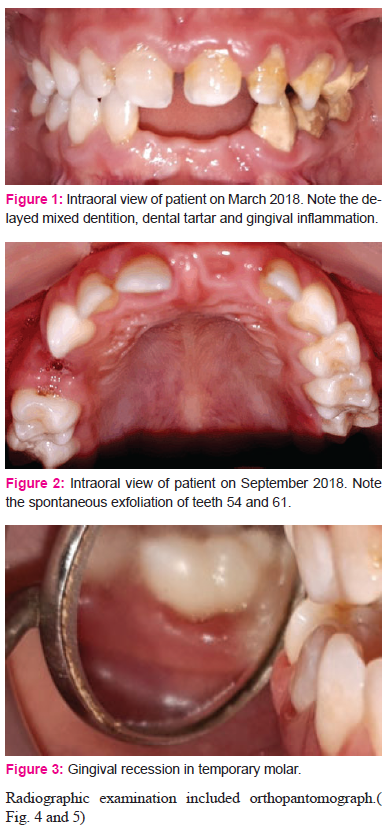
The intraoral examination revealed a delayed tooth eruption in permanent dentition. The gingiva presented signs of inflammation. Also, the patient presented dental tartar on the left side.( Fig. 1)
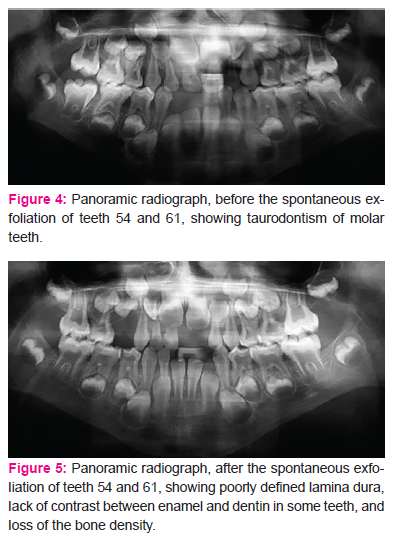
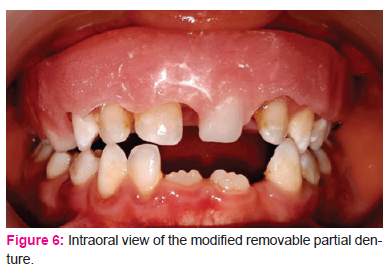
Teeth 61, 82 and 54 were exfoliated spontaneously without history of tooth decay or trauma (Fig. 2). Moreover, All erupted teeth showed a normal size and shape. But all temporary teeth are mobile and opaque areas (hypocalcification) showed especially in the 51, 62, 63 and 64. Gingival recession was described in temporary molar.(Fig. 3)
The most significant radiographic finding was the taurodontism of both primary and permanent molars. In addition, the developing of dental germs were normal in number and shape, but this development was delayed.
Also, we found poorly defined lamina dura, lack of contrast between enamel and dentin in some teeth, and loss of the bone density in maxilla and mandible.
Treatment
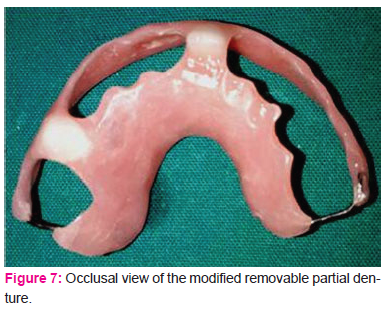
Our patient was counseled and educated on the maintenance of good oral hygiene. The patient underwent descaling. Then, fissure sealants were applied to all permanent first molars. A modified removable partial denture was indicated to replace teeth 61 and 54. The removable partial denture did not contain clasp, because this dispositive could damage loose teeth with an increased risk of falling (Fig 6 and 7). However, the maxillary base plate was expanded to vestibular gum in order to make the appliance more stable and retentive.
Discussion
Oral manifestations:
Fanconi Bickel Syndrome is accompanied by severe growth deficiency and hypophosphatemic rickets, including craniofacial manifestations. Those manifestations were previously reported by Morisaki in 1989, which described a case affected by Fanconi's syndrome with growth deficiency of craniofacial bones and dental alterations. Family history of this case revealed healthy parents without consanguineous marriage.[10]
Oral manifestations of this disease, as seen in the present case, includes delayed development of dentition, opaque areas (hypocalcification), rapidly progressive periodontal disease and premature loss of temporary teeth.
Also, the pulp/crown ratio of all molar teeth showed taurodontism, as mentioned by Jorgenson et al. [11]
In fact, this dental findings of Fanconi Bickel Syndrome have been described as similar with variable degrees to those in hypophosphatemic vitamin D-resistant rickets, Renal tubular acidosis, and hepatomegaly resulting from glycogen storage disease type XI.[9,12]
The renal tubular defect decreases the renal threshold for phosphate. This results in loss of phosphates, sugars and amino acids which leads to a failure of calcium. Thus, hypophosphatemic rickets can be developed. Also, this disorder can be caused by a failure of production of 1,25-dihydroxy vitamin D from its precursor 25-hydroxy vitamin D. This altered vitamin D absorption and metabolism affects the growth and development of calcified tissue in the body, including the dental hard tissue. This syndrome results in hypoplasia and deficient calcification of mineralized structures such as bones and teeth. Mainly, dental enamel is the most mineralized tissue in human body, white opaque areas (hypocalcification) or enamel hypoplasia, has been reported in a child with Fanconi Bickel Syndrome.[10,13,14] Clinical and histologic abnormalities may be seen in the dental hard tissue, essentially when systemic symptoms appear during a period of odontogenesis. [15]
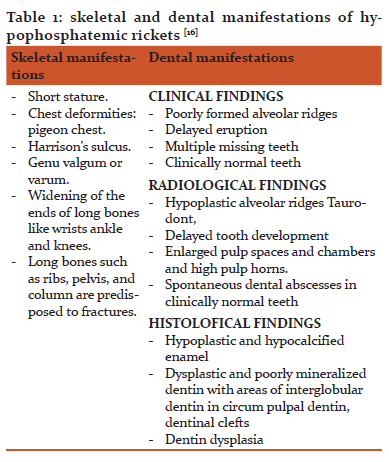
Hypophosphatemic rickets are characterized by different skeletal and dental manifestations. Those characteristics are collected in Table 1. [16]
As regards delayed eruption, it is considered one of the symptoms of Fanconi’s syndrome.[9] In fact, delayed dental development, like growth deficiency, is a secondary to disturbed biochemical findings that results from deficient hepatic and renal glucose-6-phosphatase activity.[15] Besides, A chronic metabolic acidosis can be a factor in the formation of the dental disease.[17]
Dental considerations:
Firstly, preventive dental care must be included into the treatment plan. All patients affected by Fanconi's syndrome need counseling and educating on the importance of maintenance of good oral hygiene. Periodic dental examinations each 3 mouth is obligatory. Also, pit and fissure sealants are indicated when the permanent teeth are erupting.
In any case, these patients had a high carious risk, because of the hypocalcification on the one hand and his treatment which based on the providing exogenous glucose on the other hand. In fact, this treatment includes frequent carbohydrate feedings during the day and continuous overnight intragastric infusions of glucose polymers.[18,19]
This glucose polymers cause a decrease in plaque pH below the critical pH of 5·5. [20] In addition, in children over 2-years-old the daytime glucose polymer is replaced with uncooked cornstarch that acts as a slow release source of glucose.[20] The caries potential of uncooked cornstarch is less than that of glucose, but, cornstarch has a tendency to adhere to the enamel surface if it is not carefully removed each day. [20]
Another point is that premature loss of temporary teeth can be managed by oral
rehabilitation in order to facilitate speech, mastication, and esthetics. But, it is very important to be careful about the periodontal state of the teeth and we must not damage them more.
Conclusion
In conclusion, we reported, in this paper, a dental findings in patient with Fanconi Bickel Syndrome. Multiple missing teeth, mobility opaque areas and delayed eruption are described in this case. They make us thinking that an oral evaluation should be performed in all patients with Fanconi Bickel Syndrome.
Moreover, the pediatrician and the dentist have to collaborate during the early ages of the affected individuals. Besides, early diagnosis is essential, since morbidity can be minimized if children are treated before the age of eight months. [21]
Finally, the knowledge of craniofacial features and various dental abnormalities helps dentist to identify the underlying systemic disease and cure them well.
Acknowledgements
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
-
Glycogen storage disease due to GLUT2 deficiency Available from https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Expert=2088&lng=EN:/
-
Fanconi G, Bickel H. Die chronische Aminoacidurie (Aminosaeurediabetes oder nephrotischglukosurischer Zwergwuchs) bei der Glykogenoseund der Cystinkrankheit. Helv Pediat Acta. 1949;4:359-396.
-
Santer R, Schneppenheim R, Suter D, Schaub J, Steinmann B, Fanconi-Bickel syndrome – the original patient and his natural history, historical steps leading to the primary defect, and a review of the literature. Eur J Pediatr. 1998; 157(10):783-797.
-
Klootwijk E, Reichold M, Helip-Wooley A et al. Mistargeting of peroxisomal EHHADH and inherited renal Fanconi’s syndrome. N Engl J Med. 2014; 370(2):129-138.
-
Pereira PCB, Miranda DM, Oliveira EA et al. Molecular pathophysiology of renal tubular acidosis. Curr Genomics. 2009; 10(1):51-59.
-
Santer R, Schneppenheim R, Dombrowski A, Gotze H, Steinmann B, Schaub J, Mutations in GLUT2, the gene for the liver-type glucose transporter, in patients with Fanconi Bickel syndrome. Nature Genet. 1997; 17(3):324-326.
-
Drube J, Schiffer E, Mischak H et al. Urinary proteome pattern in children with renal Fanconi syndrome. Nephrol Dial Transplant. 2009; 24(7):2161-2169.
-
Karande S, Kumbhare N, Kulkarni M, Fanconi-Bickel Syndrome. Indian Pediatrics. 2007; 44(3):223-225
-
Ichijiro M, Keiko A, Shizuo S, Orofacial manifestations in a child with Fanconi’s syndrome. ORAL SURG ORAL MED ORAL PATHOL. 1989; 68(2):171-174.
-
SHIRLENE B, and al, Dental findings in Brazilian patients with Fanconi syndrome. International Journal of Paediatric Dentistry. 2016; 26(1): 77-80.
-
Jorgenson RJ, Salinas CF, Shapiro SD, The prevalence of taurodontism in a select population. J Craniofac Genet Dev Biol. 1982;2(2):125-136.
-
Jagtap s v. and al. review: Hypophosphatemic rickets. Indian journal of endocrinology and metabolism. 2012; 16 (2):177-182.
-
Bata P, Tejani Z, Mars M, X-Linked hypophosphatemia: Dental and histologic findings. J Can Dent Assoc. 2006; 72 (1): 69-72.
-
Tümen and al. Types of Rickets, Dental and Histologic Findings: Review of the Literature. Pesq Bras Odontoped Clin Integr. 2009; 9(2):241-246.
-
Loevy HT, Matalon R, Rosenthal IM, Delayed dental age in hepatorenal glycogen storage disease. JADA. 1983; 107(6):944-946.
-
Veena R, Babitha K, Anuradha P Orofacial and Skeletal Manifestations of Hypophosphatemic Rickets in Fanconi Bickel Syndrome. American Journal of Clinical Medicine Research. 2014; 2(4): 68-71
-
Katz J, Shenkman Z, Sela M, Rakotz M, Garty BZ, Oral manifestations and anesthesia considerations in a child with glycogen storage disease type Ib: Case report. Pediatr Dent. 1997;19(2):123–126.
-
Savelli PD, and al, Fanconi syndrome. Metabolic studies on treatment. The Journal of bone and joint surgery. 1955; 2 (4):529-539.
-
Scriver CR and al, The Metabolic and Molecular Bases of Inherited Disease 8th Edition 2001. Journal of Inherited Metabolic Disease.2001; 24(4):519-520.
-
Kidd SA, Rademeyer C, Roberts GJ, Lee PJ, Lucas VS, Dental disease indices and caries-related microflora in children with glycogen storage disease. International Journal of Paediatric Dentistry .2002; 12(1): 8-13.
-
Types of Rickets, Dental and Histologic Findings: Review of the Literature Available from http://www.redalyc.org/articulo.oa?id=63712851017
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





