IJCRR - 11(2), January, 2019
Pages: 01-06
Date of Publication: 22-Jan-2019
Print Article
Download XML Download PDF
Comparison of Effects of Continuous and Interval Training on Aerobic Capacity in Healthy, Non Exercising Young Individuals
Author: Saba Khan, Razia Nagarwala, Ashok Shyam, Parag Sancheti
Category: Healthcare
Abstract:Objective: Participation in aerobic exercise generates increased cardiorespiratory fitness, which results in a protective factor for cardiovascular disease and all-cause mortality. Interval training might cause higher increases in cardiorespiratory fitness in comparison with continuous training; nevertheless, current evidence is not conclusive. This study tests the effect of interval training with moderate intensity continuous training on aerobic capacity (V02 max).
Method: 40 young healthy subjects were recruited according to inclusion and exclusion criteria and were randomly allocated into a supervised 6 week endurance training program of 3 weekly sessions of either Interval training ( 5 minutes' bout at 75%-80% HRMax with 2 minutes of active recovery at 40% -50% HRMax) and continuous training (40%- 60% HR Max) of walking on a treadmill for 30 minutes per session. Primary outcome measure was V02max; secondary outcome measure was resting heart rate, resting respiratory rate, blood pressure and Rating of Perceived Exertion.
Results: Vo2max (ml/kg/min) improved significantly in both the groups.(P=0.000). There was reduction in resting heart rate, resting respiratory rate and resting blood pressure in both the groups post 6 weeks of training intervention. Rate of perceived exertion was unchanged in both the groups post training intervention.
Conclusion: It was observed that both the groups showed significant improvements in aerobic capacity (Vo2max). There was reduction in resting heart rate, resting respiratory rate and resting blood pressure in both the groups post 6 weeks of training intervention.
Keywords: Interval training, Continuous training, VO2max
Full Text:
INTRODUCTION
Exercise, in general, is one of the best preventive actions to fight illness and maintain health. There is an increasing evidence of cardiovascular problems in present era, due to which importance of exercise for development of fitness is on rise. There is a slow decline in cardiovascular function with advancing age that is significantly accentuated by a sedentary lifestyle. ACSM has released a physical activity guideline to improve physical fitness. Hence it was recommended that “there should be accumulation of at least 30 minutes of moderate activity on most preferably all days of week.” [1]
Participation in aerobic exercise develops increased cardiorespiratory fitness, which protects from cardiovascular morbidity and mortality. Maximal oxygen consumption (VO2max) provides a measure of the maximal volume of oxygen that the body consumes via the respiratory system and is transported through the bloodstream to be used to release energy in the cell.
VO2max is currently the best indicator to assess Cardiorespiratory fitness and it is directly related to cardiovascular health, and its improvement has been linked to decreases in risk of death from cardiovascular disease. Laukkanen et al. studied the association between low levels of VO2max (<27.6 ml/(kg min)) and premature death and found that unfit men had more than twice the risk of overall death and over three times the risk of cardiovascular-disease-related death in comparison with fit men (VO2max >37.1 ml/kg/min)[2]
In a study conducted by Richard suminski etal, found that 28.1% of Asian college going students aged 18 to 25 years are physically inactive.[3]
Low fitness levels are responsible for the highest proportion of deaths, followed by smoking had amongst the four cardiovascular lifestyle factors. Hence interventions to decrease the prevalence of low fitness and smoking can promote reduced mortality rates.[4]
Intensity seems to be an important predictor of the effectiveness of fitness training programmes. Moderate-intensity continuous training methods and high-intensity interval training are typically prescribed to increase Cardiorespiratory fitness. Continuous or long, slow distance training involves steady paced prolonged exercise at either moderate or high aerobic intensity, usually 60-80%Vo2max. Continuous exercise may increase Vo2max, capillary density, oxidative enzyme activity and plasma volume in untrained individuals. [5]
Interval training consists of periods of high-intensity exercise alternated by periods of relative rest that makes it possible for patients to complete short work periods at higher intensities. Aerobic interval training is one of the most common training methods to improve athletes’ endurance and training performance. Continuous (CT) and interval training (IT) are both established exercise modalities used in the rehabilitation of patients with chronic diseases as well as to improve aerobic and anaerobic capacity of elite athletes. [6]
The sedentary non exercising age group is most susceptible to develop cardiovascular problems hence this study aims to find out the effects of continuous and interval training modes on Vo2max so as to predict which is more better for improving cardiovascular fitness so that we can make recommendations on how to improve fitness level in young population in the rehabilitation setting so as to maximize training effects and provide a shortened fitness program to promote a better, holistic feeling of health in young individuals.
MATERIALS AND METHODS:
Subjects
40 Sedentary (≤150 min of aerobic exercise a week) young individuals between 18-28 years of age were recruited to participate in this study. Prior to starting the program, all participants had to accept their voluntary participation by signing an informed consent form. The participants were made to answer PAR-Q (physical activity readiness Questionnaire) questionnaire and those who met the inclusion and exclusion criteria were included in the study.
The inclusion criteria were Males and females in 18-28 years age group Healthy, non exercising, recreationally active adults without any co morbid illness.
The exclusion criteria were subjects with Body mass index BMI>40, any neuro-musculoskeletal problems, cardiovascular and respiratory problems, Smokers and any other systemic illness. The subjects were randomly assigned into two groups, continuous training and interval training group.
Study design
Subjects were ascribed randomly using computer generated randomized table into two experimental groups: Continuous training (CT) or Interval training (IT) .20 subjects in each group.
Prior to training the subjects were made to walk on treadmill (Trackmaster® model TMX 425C) and predicted Vo2max (Max aerobic capacity) was calculated according to modified Bruce protocol.
The equation for calculation of Vo2Max using modified Bruce protocol is: VO2max = 3.5+ [0.1*speed] + [1.8*speed*grade][1]
Training program:
Subjects performed 3 training sessions per week in the laboratory over a 6 weeks period (18 sessions).
CONTINUOUS TRAINING PROTOCOL consisted of 5min of warm up –stretching, spot jogging , 30 minutes of walking on treadmill (Trackmaster® model TMX 425C) at40%- 60% HR Max followed by 5 minutes of cool down which included stretching, spot jogging, breathing exercises.
INTERVAL TRAINING PROTOCOL consisted of 5 minutes of warm up-stretching, spot jogging, 30 mins training including-5 minutes’ bout of treadmill exercise at 75%-80% HRMax with 2 minutes of active recovery, i.e. treadmill walking at 40% -50% HRMax followed by 5 minutes of cool down which included stretching, spot jogging, breathing exercise. The intensity of each interval training session was reached and adjusted manually throughout the session by a trained investigator manipulating the speed and incline of the treadmill to reach the target heart rate.
Pre training and Immediate post training Heart rate (HR), Respiratory rate (RR), Blood pressure (BP) and Rating of perceived exertion (RPE) using Borg’s scale was obtained. (6-20 Borg’s scale)
All the subjects underwent supervised training for 6 weeks, 3 times per week on alternate days.
Post 6 weeks of training Vo2max (aerobic capacity) was again calculated using modified Bruce protocol on treadmill (Trackmaster® model TMX 425C).
OUTCOME MEASURES
The primary outcome measure was Pre training and post training Vo2max using Modified Bruce protocol on treadmill. The secondary outcome measures were pre training and post training vitals HR, RR, BP and Rate of perceived Exertion (RPE).
STATISTICAL ANALYSIS:
The statistical analysis was done by using SPSS software 16. P value was set at 0.05. The intra group pre and post test aerobic capacity (Vo2max), BP, HR, RR were analysed using paired t test. The inter group post test scores of aerobic capacity(Vo2max) , BP, HR, RR were analysed using unpaired t test.
RESULTS:
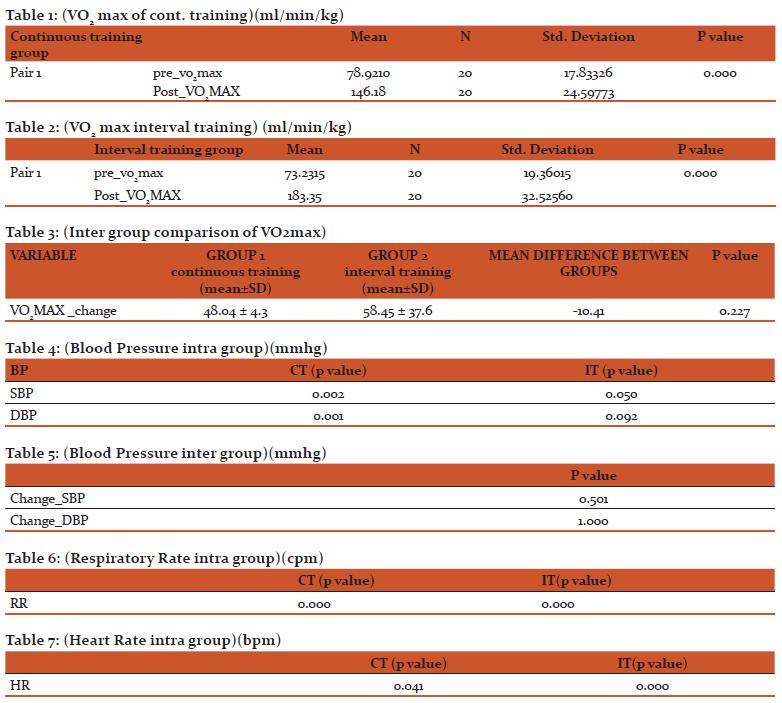
40 patients (20 in each group) were enrolled and all completed the study, without any dropouts. As shown from table 1 and table 2, Vo2max improved significantly in continuous training and interval training groups respectively.
TABLE 1 (VO2 max of cont. training)
t(df)=- 12.50(19); p value=0.000. The p value was set at 0.05.
The p value is less than 0.05 for intra group analysis for continuous training. Hence it is statistically significant
TABLE 2 (VO2max of interval training group)
t(df)= - 17.52(19); p value=0.000; p<0.05 . Hence it is statistically significant.
The above table shows that p value of within group for interval training group is less than 0.05, hence it is statistically significant.
TABLE 3: (inter group comparison of VO2max)
There was no significant difference in Vo2Max between both the groups as per table 3. p value =0.227 for change in Vo2Max between both the groups.
TABLE 4; (Blood Pressure intra group)
There was significant reduction in resting systolic BP in both the training groups post intervention
TABLE 5: (Blood Pressure inter group)
P is not <0.05 for change in BP hence, insignificant
TABLE 6: (Respiratory Rate intra group)
There was significant in reduction in resting RR in both the groups post training .p<0.05.The p value for change_RR between both the training groups was 0.210. p value not less than 0.05, hence it is not statistically significant
TABLE 7: (Heart Rate intra group)
There was a statistically significant reduction in HR in both the groups. The p value for change in HR in between both the groups was 0.000, p value<0.05, hence it was statistically significant.
DISCUSSION
The purpose of this study was to compare the effects of six weeks of continuous training and interval training on aerobic capacity (Vo2Max) and cardiorespiratory parameters i.e. heart rate, blood pressure, respiratory rate and RPE Borgs scale in young healthy individuals. The primary findings of this study is that young, previously sedentary, recreationally active individuals randomly assigned to six weeks of continuous training and interval training on treadmill showed similar improvements in aerobic capacity (Vo2Max). The subjects also showed statistically significant improvements in cardiovascular parameters i.e. blood pressure, heart rate and respiratory rate in both the groups.
There was no change in RPE Borg’s scale in both the groups post training
Aerobic capacity (Vo2Max):
Vo2Max improved significantly in both the groups individually.Vo2Max improved with 58±14.92 ml/kg/min in interval training group and with 48.04±4.71 ml/kg/min in continuous training group. These increases are of clinical relevance, as shown in a large observational study, where each 3.5 ml/kg/min increment in peak VO2 resulted in a 12% improvement in survival [7]
Vo2Max improved in interval training group with 58±14.92 ml/kg/min after 6 weeks. In a study conducted by Khadijeh Pour-Abdi et al 2013, Interval running done in 4 replicates of 4 minutes and 30 seconds with an intensity of 75% of HRR and three minutes active rest including jogging and light running with an intensity of 60% of HRR for 6 weeks, 3 times a week on alternate days caused a significant increase in maximal oxygen consumption.[8]
HIIT requires a higher oxygen delivery which leads to greater adaptations of the oxygen delivery system (e.g. through increased stroke volume and cardiac output) which leads to an increase in VO2Max. HIIT allows the participants to stay longer at VO2Max during active rest, and does not allow the decline of lactate which helps the improvement of VO2Max. Active recovery has shown to result in a faster clearance rate of lactic acid, making it the preferred form of recovery when compared to a passive form of recovery.[9] This improvement in interval training group might be due to the increases in oxygen delivery as well as improved oxygen utilization by active muscles through greater capillarization and mitochondrial density.[10] Due to frequent breaks between activities, in interval training more oxygen is made available to muscles ,which improves the interactions and energy saving. Thus Interval exercise scan causes significant changes in muscle metabolism through the expansion of the capillary network and increasing the content of mitochondrial enzymes. These changes further cause increased oxidation of fats, reduced adipose tissue, remaining glycogen storage, lower lactic acid production, and less feeling of fatigue.[11]
Vo2Max improved significantly in continuous training group by 48.04±4.71 ml/kg/min in a study conducted by Gordon Fisher et al 2015 on sedentary overweight or obese men assigned to HIIT and moderate intensity continuous exercise (MIT), for 6 weeks showed that a greater improvement in VO2peak occurred in MIT (11.1%) compared to HIIT (2.83%).[12] Continuous endurance training causes improvement in Vo2Max via metabolic adaptations. During sub-maximal exercise, muscle O2 delivery is closely matched to mitochondrial O2 demand, increasing the potential for oxidative production of ATP. Local hypoxia is a major signal for muscular adjustments to endurance exercise, as there occurs a dramatic drop in muscle oxygen tension with the onset of exercise. The intensity of Continuous Training (above 60% of Vo2Max) induces a significant fall of cellular PO2 and therefore triggers the signaling pathways causing greater improvement of capillary density and vascular conductance with moderate intensity continuous training by improving muscle perfusion and thus O2 supply.[6]
In this study Vo2Max improved equally in both the groups of continuous training and interval training. In a study conducted by Brandon J. Sawyer et al both HIIT and MICT groups had similar increases in VO2Max after 8 wk of training [13] Studies done by Burgomaster KA et al 2008, [14] Whyte LJ et al 2010, [15] Wallman K et al 2009 ,[16]. showed similar increases in Vo2max in both the groups. The reason for non significant difference between the groups can be due to shorter duration of training i.e 6 weeks, lack of use of larger work rest ratios in case of interval training. In a study conducted by Luc E. gosselin, et al 2012, found that greater the work-to-rest ratio, the greater the VO2Max.[17] At the beginning of exercise, the contribution of different pathways [immediate breakdown of high energy phosphate stores (e.g., adenosine triphosphate, creatine phosphate), glycolysis, and aerobic metabolism] depends on a number of variables. The aerobic metabolism is determined by oxygen consumption during work, and the extent of rise depends upon the duration of exercise, the level of fitness of an individual [18] but also on the work intensity.
Whipp and Wasserman [19] demonstrated that at low workloads, steady state _VO2 is reached within 3 minutes from the start of exercise. With high work intensities, the _VO2 kinetics show an initial rapid phase followed by a slower secondary phase such that steady-state _VO2 was not achieved even in the sixth minute of exercise. Our subjects exercised at a workload corresponding to 70% of HRmax for 5 minutes and 2 minutes rest period at 40% HRmax, it can be that the work-to-rest dynamics of the exercise protocol did not allow our subjects sufficient time to achieve the expected VO2.
Resting heart rate:
In this study it was found that there was significant reduction in resting heart rate values pre and post training in both the groups.
Interval training=7.7±0.0 bpm; Continuous training=1.65±0.32.bpm
In a study conducted by Nummela A et al 2016, it was found that the nocturnal HR is decreased and nocturnal Heart rate variability indices are increased during high-intensity but not during constant load aerobic training program in sedentary participants.[20]
A lower resting-HR can be due to central and peripheral factors derived from a training program. Central factors like increase of venous return and systolic volume, and improved myocardial contractility; and peripheral factors like improved oxygen extraction (oxygen arteriovenous difference) or enhanced O2 use to generate more work (mechanical efficiency), cause HR to reduce to those (submaximal) required levels. [21]
Resting Blood Pressure:
Both the groups show a significant decrease in resting systolic blood pressure (SBP) (p<0.05) and resting diastolic blood pressure.(DBP) Resting systolic blood pressure reduced from baseline by 2.6±4.3 mmHg in interval training group and 4.30± 3.6 mmHg in continuous training group.
There is no significant difference in improvement in Blood pressure between both the groups. In a meta analysis conducted by Ve´ronique A. Cornelissen et al ,2005 where it was stated that the BP decrease was more in the hypertensive study groups (6.9/ 4.9 mm Hg), but that significant BP reductions were also seen in normotensive (2.4/1.6 mm Hg) in response to endurance training.[22] The reduction in blood pressure is due to reduced sympathetic nervous system activity with training , normalisation of arteriolar morphology and decrease peripheral resistance to blood flow.[23] 4 weeks of moderate-intensity Aerobic exercise training decreases central arterial stiffness by 9.5% and peripheral stiffness by 8.5%. [24] there occurs an increase in concentration of vasodilator substance, plasma nitric oxide (NO), and reduction in concentration of vasoconstrictor substance , plasma endothelin-1 (ET1) by aerobic exercise training in older women [24,25] causing increase in systemic arterial compliance and reducing blood pressure.
Resting respiratory rate:
Resting respiratory rate reduced after 6 weeks of training in both the groups. This can occur due to increase in kinetics of gaseous exchange. Exercise training causes improvement in the under-perfusion of respiratory muscles [26] and reverses the metabolic and histological abnormalities in respiratory muscles [27] and improved oxidative capacity of these muscles is similar to that in the peripheral skeletal muscles [28,29]
Endurance training causes an increase in aerobic enzyme levels and oxidative capacity of respiratory muscles thus increasing ventilatory muscle function. Inspiratory muscle capacity is increased to generate more force and reduce work of breathing and hence reduce the respiratory rate at rest.[30]
CONCLUSION
In this study it was found that both interval training and continuous training are equally effective in improving aerobic capacity in young healthy, non exercising individuals. Both the training modes are equally effective in reducing resting systolic and resting diastolic blood pressure, resting respiratory rate. Interval training was found to be more effective in reducing resting heart rate than continuous training.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors also acknowledge the esteemed principal of Healthcare academy for allowing us to conduct the study and providing treadmill machine for conducting training of the subjects.
CONFLICT OF INTEREST:
There was no conflict of interest between the authors regarding the study.
References:
1. ACSM guidelines for exercise testing and prescription. 9th Edition.
2. Laukkanen JA, et al. Cardiovascular fitness as a predictor of mortality in men. Arch Intern Med. 2001;161(6):825–31.
3. Richard R. Suminski PhD, Rick Petosa PhD, Alan C. Utter PhD & James J. Zhang PhD. Physical Activity Among Ethnically Diverse College Students. Journal of American College Health Vol. 51, Iss. 2, 2002
4. Xuemei Sui,1 Hongjuan Li etal. Percentage of Deaths Attributable to Poor Cardiovascular Health Lifestyle Factors: Findings from the Aerobics Center Longitudinal Study. Epidemiology Research International, Volume 2013 (2013), Article ID 437465.
5. Mazoochi M, Fateminezhad SE, Mazoochi T. Effects of Continuous and Interval Training on Different Fitness Parameters in Athletes. World applied sciences journal. 2013; 28(3):312-5.
6. Daussin FN, Zoll J, Dufour SP, Ponsot E, et al Effect of interval versus Continuous training on cardiorespiratory and mitochondrial functions: relationship to aerobic performance improvements in sedentary subjects. American journal of physiology-regulatory, integrative and comparative Physiology. 2008 Jul 1; 295(1):R264-72
7. J. Myers, M. Prakash, V. Froelicher, D. Do, S. Partington, J.E. Atwood, Exercise capacity and mortality among men referred for exercise testing, N. Engl. J. Med. 346 (11)(2002) 793–801.
8. Pour-Abdi, Kh. et al. (2013). Effects of Short-Term Interval Training Courses on Fitness and Weight Loss of Untrained GirlsAnn Appl Sport Sci, 1(2): 1-9.
9. Esfarjani F1, Laursen PB. Manipulating high-intensity interval training: effects on VO2max, the lactate threshold and 3000 m running performance in moderately trained males. J Sci Med Sport. 2007 Feb;10(1):27-35. Epub 2006 Jul 28
10. Hottenrott K, Ludyga S, Schulze S. Effects of high intensity training and Continuous endurance training on aerobic capacity and body composition in recreationally active runners. Journal of sports science & medicine. 2012 Sep;11(3):483
11. Fox EL, Mathews DK. The Physiological Basis of Physical Education and Athletics. 3rd ed: Saunders College Publishing; 1981. 677 p.
12. Fisher G, Brown AW, Bohan Brown MM, Alcorn A, Noles C, Winwood L, et al. (2015) High Intensity Interval- vs Moderate Intensity- Training for Improving Cardiometabolic Health in Overweight or Obese Males: A Randomized Controlled Trial. PLoS ONE 10(10): e0138853. Journal. Pone.0138853
13. Brandon Swayer, Welsey J Tucker et al Effects of high-intensity interval training and moderate-intensity continuous training on endothelial function and cardiometabolic risk markers in obese adults. J Applied Physiol, 2016.115 2/japplphysiol.00024.2016.
14. Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, Macdonald MJ, McGee SL, et al. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol. 2008; 586(1):151–60.
15. Whyte LJ, Gill JM, Cathcart AJ. Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metabolism. 2010; 59(10):1421–8. J. Metabol. 2010. 01.002 PMID: 20153487.
16. Wallman K, Plant LA, Rakimov B, Maiorana AJ. The effects of two modes of exercise on aerobic fitness and fat mass in an overweight population. Res Sports Med. 2009; 17(3):156–70.
17.Gosselin LE, Kozlowski KF, DeVinney-Boymel L, Hambridge C. Metabolic response of different high-intensity aerobic interval exercise protocols. The Journal of Strength & Conditioning Research. 2012 Oct 1; 26(10):2866-71.
18. Hagberg, JM, Hickson, RC, Ehsani, AA, and Holloszy, JO. Faster adjustment to and recovery from submaximal exercise in the trained state. J Appl Physiol 48: 218– 224, 1980.
19. Whipp, BJ and Wasserman, K. Oxygen uptake kinetics for various intensities of constant-load work. J Appl Physiol 33:351–356, 1972.
20. Kenny W. L. et al (1985) parasympathetic control of resting heart rate, relationship to aerobic power. Med. Sci. Sports Exer, 17:451
21. Marcos B. Almeida and Claudio Gil S. Araújo, Effects of aerobic training on heart rate, Rev Bras Med Esporte. Vol. 9, No. 2 – Mar/Abr, 2003.
22. Ve´ronique A. Cornelissen, Robert H. Fagard. Effects of Endurance Training on Blood Pressure, Blood Pressure–Regulating Mechanisms, and Cardiovascular Risk Factors, Hypertension. 2005;46:667-675.
23. William McArdle et al 2010,7th edition,Exercise Physiology.886-888.
24. Maeda S, Tanabe T, Otsuki T, et al: Moderate regular exercise increases basal production of nitric oxide in elderly women. Hypertens Res 2004; 27: 947–953.
25. Maeda S, Tanabe T, Miyauchi T, et al: Aerobic exercise training reduces plasma endothelin-1 concentration in older women. J Appl Physiol 2003; 95: 336–341.
26. Mancini D, Ferraro N, Nazzaro D, Chance B, Wilson J. Respiratory muscle deoxygenation during exercise in patients with heart failure demonstrated with near infrared spectroscopy. J Am Coll Cardiol 1991;18:492 –8
27. Lindsay DC, Lovegrove CA, Dunn MJ, et al. Hstological abnormalities of muscle from limb, thorax and diaphragm in chronic heart failure. Eur Heart J 1996;17:1239 –50
28. Adamopoulos S, Coats AJS, Brunotte F, et al. Physical training improves skeletal muscle metabolism in patients with chronic heart failure. J Am Coll Cardiol 1993;21:1101–6.
29. Stratton JR, Dunn JF, Adamopoulos S, Kemp GJ, Coats AJ, Rajagopalan B. Training partially reverses skeletal muscle metabolic abnormalities during exercise in heart failure. J Appl Physiol 1994;76:1575 –82.
30. William McArdle et al 2010, 7th edition, Exercise Physiology.467-468.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





