IJCRR - 10(19), october, 2018
Pages: 08-13
Date of Publication: 06-Oct-2018
Print Article
Download XML Download PDF
Diabetic Patients 'Perception of Their Relationship with Family Caregiver and Health-Care Providers: A Qualitative Study in the Diabetes Centre of the National Public Health Institute of Côte d'Ivoire
Author: Marie Laurette Agbre Yace, Kadidiatou Raissa Kourouma, Yvonne Tano-Kamelan, Daouda Doukoure
Category: Healthcare
Abstract:Objective: This study aimed to investigate diabetic patients' perceptions of their relationship with healthcare providers and family caregivers.
Methods: This qualitative study using semi-structured questionnaires was performed from February to April 2018, in the Diabetes Centre of the National Public Health Institute. Data were subject to thematic analysis. Data saturation was reached after 49 interviews.
Results: the majority of the patients reported having good relationship with family caregivers and the healthcare team; actors they consider important in the management of their diabetes. The main factors that can improve the involvement of the couple patients/family caregivers were: good reception, more information and diabetes education, short waiting time.
Conclusion: family caregiver, diabetic patient and healthcare provider relationship is a necessary social dynamic for the diabetic patient: the keystone of the quality of care. It is important to make further for better decision-making in order to implement of a true winning partnership between patient, family caregiver and healthcare provider.
Keywords: Diabetes, Patient, Family caregivers, Healthcare services, Cote d’Ivoire
Full Text:
INTRODUCTION
Diabetes is a growing public health concern. Indeed, according to the World Health Organization (WHO), in 2015, an estimated 1.6 million of death were directly attributable to diabetes1. Besides this chronical disease has an impact on the society, health system and individual affected by the disease.
Diabetes treatment is also part of a triangular relationship between family caregiver/patient/healthcare providers. However, the relationship between these three actors has an impact on the quality and the continuity of care at home.
In the specialist literature different factors which influence compliance with the treatment have been identified such as socio-demographic characteristics and relationships with the disease, the therapy itself, family caregivers and healthcare providers 2, 3, 4.
The healthcare provider-patient relationship is the factor with a stronger predictive power3. Indeed, this relationship is an important concept in health care, especially in primary care. Numerous studies have found out that the relationship between healthcare provider and patient is often superficial and centered more on purely systematic and physiological aspects, without taking into account the patients’ expectations, and making unilateral decisions, depending on their experience5,6.
However, it is established that actions need to be centered on the patient instead of being centered on the disease and the interests of the health institutions, thus providing integrated care 7,8,9. The theoretical framework of the evaluation of the experience lived during the trajectory of care and services takes into account eight dimensions of the experience of care, based on the model of care centered on the patient and his family10. These eight dimensions are: respect for patients' values, preferences and needs (including involvement in decisions, listening, courtesy); access to care; coordination of care across different services; information, education and communication with professionals; physical comfort (including tranquility, cleanliness and safety, and pain relief); emotional support; the involvement of family and friends; transition and continuity of care10.
In Côte d’Ivoire where the prevalence of diabetes is around 4.94% according to the International Diabetes Federation (IFD), very little is known about the diabetic patient perception of family caregiver and healthcare providers. Thus, as part of the National Public Health Institute of Côte d’Ivoire (INSP) policy of continuous improvement in the quality of care for diabetic patients followed up at the Diabetes Center (CADA) who ongoing needs and are cared for at home by family caregivers; we performed this study with the objectives to understand in depth diabetic patients’ views and experiences of their relationship with healthcare providers and family caregivers in the care-giving process.
MATERIAL AND METHODS
The study utilized a qualitative approach centered on semi-structured interviews to assess diabetic patients’ views and experiences regarding their relationship with health-care providers and family caregivers.
This qualitative research was part of a larger study on the family caregiver/diabetic patient/ health-care provider relationship, performed at CADA. CADA’s mission is the outpatient management of diabetic patient, with an active line of more than 58,000 patients up to date. The centre receives in average 50 patients per day. The nursing staff includes twelve doctors, four nurses and one nurse aid.
The study was conducted from February to April 2018. The questions of the interview guide asked during the interviews were based on a review of the literature11 and objectives were focused on the patient’ views and experiences with their family caregivers and health-care providers. The interview guide was pre-tested on a sample of 10 patients and this helped us to improve its content.
The patients were chosen at random and the interviews were conducted face to face by 3 researchers. Each interview lasted 30-45 min and was tape-recorded. Informed consent was sought before each interview. Participants were informed about the aim of the research project and what participation in semi-structured interviews meant. They were all informed that the participation was voluntary and that confidentiality would be secured throughout the research process.
The semi-structured interviews data were analyzed following recommended guidelines for qualitative research. Data collection and data analysis were carried out simultaneously. The researchers transcribed all of the interviews immediately after completing them. The data collected from interviews were transcribed in their entirety, coded and analyzed using a content and thematic analysis of the transcripts12. Data saturation was reached after 49 interviews.
RESULTS
Of the 49 patients who consented to be interviewed, around two third were women and only 19 had the help of a family caregiver. The age range was 35–75 years: patients aged between 40 and 49 years were the most numerous. Regarding the socio-professional category, the majority of the participants exercised a liberal profession followed by the unemployed and civil servants. (Table1).
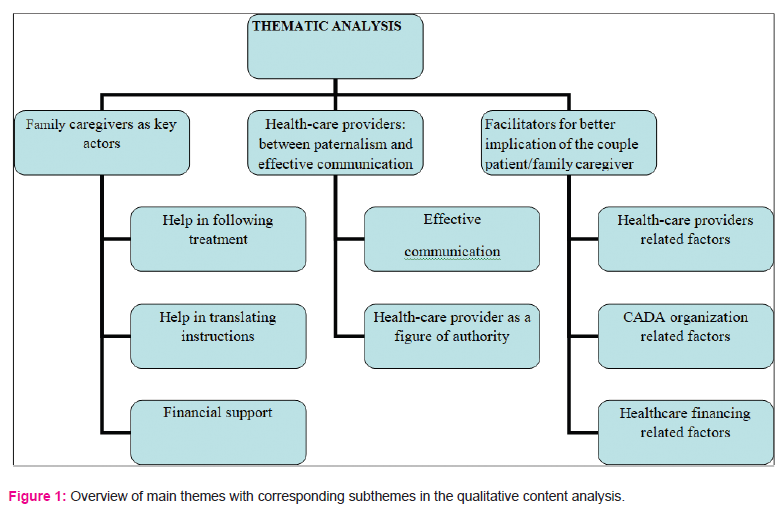
The data analysis resulted in the identification of three main themes with corresponding sub?themes related to the diabetic patients' perception of their relationship with healthcare providers and family caregivers: (1) Family caregivers as key actor for the diabetic patients; (2) Relationship with health-care providers between paternalism and effective communication, (3) Facilitators for a better involvement of the couple diabetic patient/ family caregiver in the care-giving process. Table 2 presents an overview of the main themes together with their corresponding sub?themes. Data used to illustrate the findings are verbatim quotes which have been altered as little as possible to retain authenticity, while maintaining anonymity.
Family caregiver as key factor
In general diabetic patients declared having good relationship with their family caregivers and this theme emerged from the diabetic patients' descriptions of how they perceived their relationship with their family caregivers, and is illustrated by the following subthemes: help in following treatment (medicines, diet, physical activity), help in translating the instructions given by the health-care providers, financial support.
Help in following treatment
All participants receiving help from a relative stated that they are very helpful in treatment adherence. One diabetic patient expressed it as follows: “My wife helps me a lot, she is strict with me concerning my diet, she always reminds me for my medicines and she encourages me do to some physical exercise, she even comes with me when I am walking” (diabetic patient 43).
Help in translating instructions
Moreover, family caregivers are useful for patient who does not speak French. Family caregivers can translate into dialect the instructions and information given by the healthcare staff. Many diabetic patients emphasized this essential aspect, as illustrated by one of them: “I did not go to school, so French is not easy. It is my son there who accompanies me. When the doctor talks, he explains it to me in our dialect and then I understand” (diabetic patient 31).
Financial support
Nineteen diabetic patients also mentioned the financial support of their family caregivers. Of them, one reported a situation where his daughter had an unpleasant behavior towards him because of the financial support she provides: "It is my daughter who accompanies me to my appointments, when we are sick we see everything. Some day we came for my appointment and the doctor said that I had to amputate my toe, when we finished my daughter got upset saying she was tired of spending money for my treatment. That day, I really hurt" (diabetic patient13).
Relationship with health-care provider: between paternalism and effective communication
This theme emerged from the diabetic patients' descriptions of how they perceived their relationship with the heath-care providers. The corresponding subthemes were: effective communication, health provider as a figure of authority.
All the participants highlighted the importance of the health-care providers and the key role they play in the evolution of their health. It was a statement that we found frequently during the analysis of the interviews. However the quality of relationship depends on the health-care providers approach.
Effective communication
Forty one participants stated that their health-care provider has established a good relationship with them. One of them reported it as follows: "My doctor is very kind with me, he knows how to talk to me, so that I do not stress too much about my illness. When I come to consultations, he takes his time to listen to me, I feel very important and cared. He even has my daughter’s phone number and he often calls her to check on me." (diabetic patient 02).
Health-care providers as figure of authority
Nine diabetic patients described the relationship the health-care provider has established with them as paternalist and still perceived health-care providers as a figure of authority as stated by one of them:" when I come to the consultation, our discussions are limited to instructions for treatment. Doctors know the right medicines to treat us. We do not know anything about diabetes we should follow their instructions. They know their job and we do not have to quarrel or argue with them "(diabetic patient 07).
Facilitators for a better involvement of the couple diabetic patient/ family caregiver
This theme reflects on the facilitating factors that can reinforce their implication in care-giving process and their collaboration with the healthcare staff. This is described by the following three subthemes: healthcare provider’s related factors; CADA organization related factors; healthcare financing related factors.
Healthcare provider’s related factors
All the participants emphasized the importance of a good reception by healthcare provider as illustrated by a patient: “when we come to the hospital and we are warmly welcomed, respected and doctors listen to us, there is no reason not to get involved” (diabetic patient 01)
The vast majority of the patient also deplored the lack of information on diabetes, as stated by one patient: “As far I am concerned, it will be easier for my family caregivers and me to get involved if we know everything about the disease. We must be at the same level of information. Doctors should give us more information on diabetes” (diabetic patient 44).
CADA organization related factors
For many diabetic patients the organizational practices of CADA should be improved regarding appointments management. One diabetic patient described a situation where he argued with the healthcare provider:"Some day, I came for my appointment but the doctor came late, I got upset because it's not normal. We are sick and we are the ones to come early. Doctors must come early to take us quickly (diabetic patient 20). "
Another factor was the waiting time which is too longue according to the diabetic patient interviewed as stated by this patient:" When we come here, we can wait one hour or more before being received by the healthcare provider, it is very difficult for us. Sometimes we need to eat, but we cannot go outside to look for food by for fear of missing the appointment (diabetic patient 15). "
Healthcare financing related factors
Ten of the diabetic patients declared that the reduction of the treatment cost can improve their implication in the care process. One of them expressed it as follows:" We have so many medicines and medical examination that sometimes it is not possible for me to respect my appointment. The treatment is too expensive, if the government finds a solution to reduce the cost, my wife and me will get more involved in the care process (diabetic patient 22).
Moreover, three diabetic patients also cited the availability of medicine such insulin as a facilitating factor as mentioned by one of them:" How do you want my family caregiver and me to be involved when diabetic medicine are not available (diabetic patient 19). "
DISCUSSION
Strengths and limitations of the study
The limitation of our study is linked to the interviews’ setting. Indeed, the interviews took place in CADA which may have induced a refusal to answer or generated social desirability response bias that is difficult to interpret.
The strength of our study consists in its originality and the context. CADA medical team is desirous to establish a strong family caregiver/diabetic patient/ health-care provider partnership. To succeed in this partnership, it is important to know in depth the patients view and expectations about the relationship they establish with healthcare providers and family caregivers. To this end, it is essential to develop study in proximology within CADA. The originality of this new area of research is to consider the role of healthcare provider and family caregiver as determining factors in the patient’s environment, and therefore the effectiveness of the disease management and care13.
Comparison with existing literature
Our findings showed that diabetic patients interviewed have in general a good relationship with their family caregivers and the health-care providers working at CADA.
Family caregivers are the backbone of healthcare system, and they are more and more involved in the care-giving process. In our study, the patients declared that family caregivers play an important role notably in helping them to follow the treatment, to translate instructions given by the health-care providers from French to dialect. They also give a financial support which is essential for the adherence to treatment. The importance of family caregivers, especially during consultations, was also highlighted by Fanzang in French oncology patients14. However the presence of the family caregivers can be constraining of stressful15. In our study only one diabetic patient related a situation where his daughter who accompanied him misbehaved towards him. The nature of the relationship patient/family caregiver can have an impact on the quality and the continuity of care at home, it is important for the healthcare providers to be attentive, listen in both patient and family caregiver.
As regard diabetic patient/health-care provider relationship, the majority of diabetic patient declared to have a good relationship with them and effective communication. Health-care providers should have effective communication with their patients in order to improve patient health outcomes16. However we noticed some health-care providers still establish paternalist relationship with patients.
In our study we did not explore the perception of the patient concerning the impact of poor relationship patient-physicians on the care-giving process. However in the study we conducted among health professionals in CADA, these declared that a poor relationship with diabetic patient could lead to the abandonment of the health structure and care17.
Moreover, a study carried out in China which investigated how aspects of the patient-physician relationship are associated with diabetes-related distress, insulin adherence, and glycemic control, showed that: patient dissatisfied with aspects of their interactions with physicians, exhibited poor insulin adherence18.
On the other hand, the qualitative study performed by Beverly and colleagues highlights the fact that both physicians and patients often assumed responsibilities for poor clinical outcomes in the treatment of type 2 diabetes. Patients felt defeated, depressed and expressed lack of self-efficacy, while physicians pointed to health system constraints and high expectations19.
Numerous studies have shown that patients prioritize the relational qualities of their caregivers19,20. In our study, relational qualities (listening, respect, kindness, hospitality) were cited by patients as one of the factors that facilitate their implication as well as that of their family caregiver in the care-giving process. In addition to this facilitator, the information and education of patients and family caregiver, the reduction of waiting time were also cited. For best patient outcomes, it is essential that patients have a more active role in their care20. When patients work in partnership with healthcare providers: complications decrease and care is better. Additionally, physicians’ perceived responsibility and patients’ self-blame for difficulty achieving treatment goals may serve as barriers to an effective relationship. Physicians and patients may benefit from a greater understanding of each other’s frustrations and challenges in diabetes management19.
Implications for future research and healthcare providers practices
The establishment of a positive and trusting therapeutic relationship with patients and family caregivers is recognized as an essential component of healthcare providers practice and is important for effective care. It is crucial for healthcare providers of CADA to use a framework to develop therapeutic relationships with the couple patient/family caregiver. It also important in clinical practice, to explore and understand the challenges in developing effective therapeutic relationships with patient at the healthcare system level, and considers how these challenges can be addressed through the implementation of proximology study13.
CONCLUSION
In healthcare system, the key to any successful patient health outcomes is the recognition of the inseparable partnership between the couple patient/family and health professional. There is a need for decision makers to recognize the importance and the impact of this partnership on the quality of care. It is also crucial for health professionals to ensure that they work together with the couple patient/family caregiver, to establish effective communication and to pay attention to their needs in order to improve the quality of care.
AUTHOR CONTRIBUTIONS
M.L.A.Y and K.R.K had the initial idea for this study and wrote the research proposal. K.R.K, D.D and Y.T.K conducted interviews: read, coded, and thematically analyzed the transcripts; and wrote the manuscript. M.L.A.Y and K.R.K reviewed and edited the manuscript. All contributors had access to the data and can take responsibility for the integrity of the data and the accuracy of the data analysis.
CONFLITS OF INTERESTS:
Authors declare no conflict of interest
ACKNOWLEDGEMENTS
The authors would like to thank CRESAR-CI (Cellule de Recherche en Santé de la Reproduction de Côte d’Ivoire) for its technical and financial support during the study implementation. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Organisation Mondiale de la Santé, http://www.who.int/mediacentre/factsheets/fs312/fr/ consulté le 23 mars 2018.
2. Heredia Galán MV. ¿Qué influye en la adherencia al tratamiento de la diabetes? Rol de Enfermería 2004, 27:57-60.
3. Carratalá Munuera C, Orozco Beltrán D, Gil Guillén V, Merino Sánchez J. Factores en el cumplimiento terapéutico y diabetes. In: Gil Guillén V, Merino Sánchez J, Palop Larrea V, editors. El cumplimiento factor clave en el control de las enfermedades. Valencia: SVMFIC Societat Valenciana de Medicina Familiar i Comunitaria 2003, p. 133-42.
4. Emanuel EJ, Fairclough DL, Slutsman J, Alpert H, Baldwin D, Emanuel LL. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Eng J Med 1999, 341:956-63.
5. Fernández Fernández I. Atención sanitaria centrada en el paciente con diabetes: necesitamos incorporar las perspectivas/expectativas de los pacientes. Aten Primaria 2002, 32:195-202.
6. Isla P, López C, Valls R. Diabetes mellitus. Expectativas de futuro en la educación sanitaria. Rol de Enfermería 1997, 224:51-3.
7. Peralta G, Figuerola D. Aspectos psicosociales de la diabetes. Endocrinol Nutr 2003, 50:280-5.
8. Szabó-Kallai K, Gyimesi A, Iványi J. Role of emotional factors in diabetes. Acta Diabetol. 1990, 27:23-9.
9. Hiscock J, Legard R, Snape D. Listening to diabetes service users: qualitative findings for the Diabetes National Service Framework, UK; 2001.
10. Gerteis, M., Edgman-Levitan, S., Daley, J., & Delbanco, T. Through the patient' eyes: Understanding and promoting patient-centered care. San Francisco: Jossey-Bass Publishers; 1993.
11. Ridd M, Shaw A, Lewis G, Salisbury C. The patient–doctor relationship: a synthesis of the qualitative literature on patients' perspectives Br J Gen Pract 2009 Apr 1; 59(561): e116–e133.
12. Guest GS, MacQueen KM, Namey EE. Applied thematic analysis. Thousand Oaks: Sage; 2012.
13. Proximology, Perspectives on the entourage of sick, dependent or disabled people, coord. and preface by Hugues Joublin, p. XI.
14. Fainzang S, La relation médecins-malades : information et mensonge, Paris, Presses Universitaires de France ; 2006.
15. Schnitzler M. Le rôle de l'entourage au sein de l'hôpital africain: une thématique négligée? Sciences sociales et santé 2014, 32(1): 39-64.
16. Klein E. R. Effective communication with patients. The Pennsylvania Nurse 2005, 60(4): 14-15.
17. Kourouma KR, Agbre Yace ML, Doukoure D, Tano Kamelan Y, N’Dia Anon F, Acka KF, Aka J, Aké O, Aké M and Kouassi D Health Professionals’ perceptions and Experiences of Family Caregivers: A Pilot Qualitative Study Carried Out at the Diabetes Centre of the National Public Health Institute of Cote d’Ivoire. Nurs Health Care Int J 2018, 2(5): 000157.
18. Linetzky B, Jiang D , Funnell MM, Curtis BH, Polonsky WH. Exploring the role of the patient-physician relationship on insulin adherence and clinical outcomes in type 2 diabetes: Insights from the MOSAIc study. J Diabetes 2017 Jun, 9(6):596-605. doi: 10.1111/1753 0407.12443.
19. Elizabeth A. Beverly, Marilyn D. Ritholz, Kelly M. Brooks , Brittney A. Hultgren, Yishan Lee, Martin J. Abrahamson, and Katie Weinger. A Qualitative Study of Perceived Responsibility and Self-Blame in Type 2 Diabetes: Reflections of Physicians and Patients J Gen Intern Med 2012 Sep, 27(9): 1180–1187; doi: 10.1007/s11606-012-2070-0.
20. Marie Lorraine FRIDERICH La relation soignant-soigné au Burkina Faso en 2008. Comment les professionnels et les patients la perçoivent-ils? Available on http://docnum.univlorraine.fr/public/SCDMED_T_2009_FRIDERICH_MARIE_LORRAINE.pdf
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





