IJCRR - 10(18), September, 2018
Pages: 18-24
Date of Publication: 28-Sep-2018
Print Article
Download XML Download PDF
Cataract Burden in a Peri-Urban Local Government in a Low Income Country: The Need for Government Intervention
Author: Onabolu Oluwatoni, Fakolujo Victoria, Ajibode Haroun, Bodunde Olubunmi, Otulana Olusola
Category: Healthcare
Abstract:Objective: To determine the prevalence of cataract in Sagamu Local Government Area (SLGA), in Ogun State of Nigeria and suggest strategies for government intervention. Methods: The study was conducted among adult population who were 30 years and above and regular residents of SLGA, Ogun state, Nigeria. After ocular examination of the respondents their pupils were fully dilated with tropicamide 1% and crystalline lens focused with the plus +9diopters on the direct ophthalmoscope. Lens opacity was graded into no opacity, few dot opacities, observed opacity less than clear area, observed opacity more than clear area, opacity obscuring total field, aphakia or displaced lens, pseudophakia, and unable to assess due to corneal opacities. Lens opacities more than clear area and total lens opacities were designated as \"cataracts\". Results: Six hundred and eight participants were included in this study consisting of 369 females (60.7%) and 239 males (39.3%) with M:F of 1:1.6 Age range was 30-80 years. Prevalence of \"cataracts\" affecting vision in the right eye was 9.04%. Twenty participants (3.28%) had uniocular blindness (vision< 3/60). Cataract was significantly higher in those above 50 years and in non-professionals. There were no eye care workers in neither primary nor secondary health facilities in SLGA. Conclusion: The prevalence of cataract blindness in Sagamu Local Government Area was 9.04% and is a cause for concern. Both State and Local Government should be ready to take responsibility for increase uptake in cataract surgery.
Keywords: Cataract prevalence, Cataract surgical uptake, Government intervention
Full Text:
Introduction
Cataract is the most common cause of blindness worldwide with its high prevalence responsible for unfavourable social burdens as well as functional disabilities.[1] Age related cataract is the most common type and elderly people in rural areas of the world are most affected.[1] The vision loss expert group in 2015 estimated that about 36 million people are blind in the world and that cataract remains the leading cause of blindness contributing to 26% of visual impairment out of which 12.6 % are blind.[2] Cataract blindness is more prevalent in poorer regions of the world especially in low and middle income countries.[3] The Nigerian National Survey of blindness found that about 43% of blindness is due to cataracts.[4]
World Health Organization (WHO) and International Agency for the Prevention of Blindness (IAPB) launched VISION 2020 in 1999 to reduce causes of avoidable blindness world- wide. Cataract was one of the diseases targeted.[5] The only treatment for cataract is surgery. Modern surgery of cataract is visually rewarding, cost effective and has been found to improve the quality of lives of individuals.[6] Researchers have found that there are barriers in accessing cataract surgery especially in low income countries in Africa.[3] Cost of cataract surgery is an important barrier because often times people pay out of pocket and the elderly cannot afford high cost of surgery.[7] Lack of awareness of surgical intervention, fear of surgery, distance to the hospital and having an escort are notable barriers. [8,9] There is also gender preference for males to be treated first and socio cultural practices delaying access to surgery in females.[10] .Poor outcome of surgery is a barrier that is often not considered especially when offering free surgery.[11,12] In order to reduce the barrier of cost in cataract surgery some countries have implemented free surgery especially to the poor.[13]
. Although South West of Nigeria had the lowest prevalence of blindness of 2.8%, cataract is still the most common cause of blindness.[14] The cataract surgical rate in Nigeria is low at 300 per million. [5] More than 10 years after the Nigerian National survey of blindness there is a need to determine the magnitude of cataract blindness in Nigeria especially in rural areas. Sagamu Local government area is largely peri-urban having a tertiary health center with comprehensive eye care service in Sagamu town. Research has shown that it is possible to find a high prevalence of cataracts even where surgical services are readily available.[16] The aim of this study is to determine the prevalence of vision disabling cataract in Sagamu Local Government Area and suggest strategies for government intervention to reduce cataract blindness.
Materials and Methods
Sagamu Local Government Area(SLGA) is one of the 20 Local Government areas in Ogun state of Nigeria. Ogun state is in the South West of the country..[17] The people are mainly Yorubas and the occupation of the rural areas is subsistence farming. The urban underserved is populated by factory workers and petty traders who are indigenes and migrant workers from other states.
The population is about 255,885 comprising 126,855 males (49.6%) and 129,030 females (50.4%).[19] Population estimates for those 30 years and older was 74,974. There is one teaching hospital where four ophthalmologists, six residents and seven ophthalmic nurses render comprehensive eye care services. There are ophthalmologists in private settings who operate on cataracts but they do not render comprehensive services. Local government clinics (28) do not have eye care workers nor render eye care services.
Study design: This was a population based; descriptive, cross-sectional study conducted using a multi-stage stratified, cluster random sampling technique with probability proportional to size. It was part of a study on “Presbyopia: Prevalence and impact on quality of life in adults of SLGA of Ogun State”.[17]It took place between 17th of September and 25th of November 2012. The setting was among adult population 30 years and above who were regular residents of the SLGA. The minimum sample size was calculated using the Leslie-Kish formula.[18] The minimum sample size was 441, but was adjusted to 662 by 1.5 for design effects. Each cluster had 50 participants. The sampling unit was the household which was taken to consist of all individuals who live under the same roof.
Each eligible individual was given an identification slip to bring to the examination centre where interviews were conducted. The socio-demographic details of the respondents were obtained in addition to visual acuity, ocular examination with a pen torch, refraction and fundoscopy. .[17] After the preliminary tests, participants were seated in a darkened area of the room where the pupils were dilated with1% Tropicamide. The crystalline lens was examined with a brightly lit direct ophthalmoscope held with its dial on +9 diopters at about 20cm from the eye. This was conducted by two independent ophthalmologists (OO and VO). There was good Inter rater agreement of ≥0.6
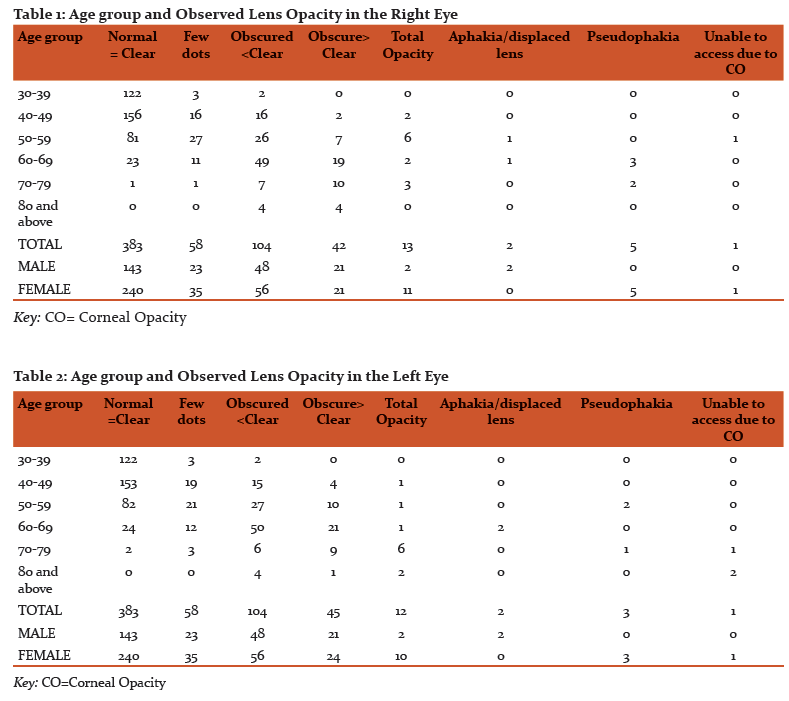
The lens opacity was classified thus: (1) Normal-no lens opacities, (2) few dot opacities, (3) observed opacity less than clear area, (4) observed opacity more than clear area, (5) opacity obscuring total field, (6) Aphakia or displaced lens, (7) Pseudophakia, (8) Unable to assess due to corneal opacities.[19] Lens opacities more than clear area and total lens opacities were designated as “cataracts”. Operable cataracts in this study were those whose vision were ≤ 6/60, had total lens opacities and lens opacities more than clear areas with best corrected vision and no other pathology.
The results were grossly similar in both eyes therefore the Right eye was used for analysis. The only government hospital where cataract surgery was done was assessed for regular provision of cataract surgical services.
Ethical approval for this study was obtained from the ethical committee of OlabisiOnabanjo University Teaching Hospital Sagamu. Permission to carry out the study was obtained from the health department of Sagamu Local Council. Oral /written consent was obtained from each participant prior to interview and examination.
The data was entered into a computer spreadsheet of Statistical package for Social Sciences IBM Version 20 and comparison analysis done. Discrete variables were compared using chi square and odds ratio with a significant difference determined at p value < 0.05. Continuous variables were compared using arithmetic proportions.
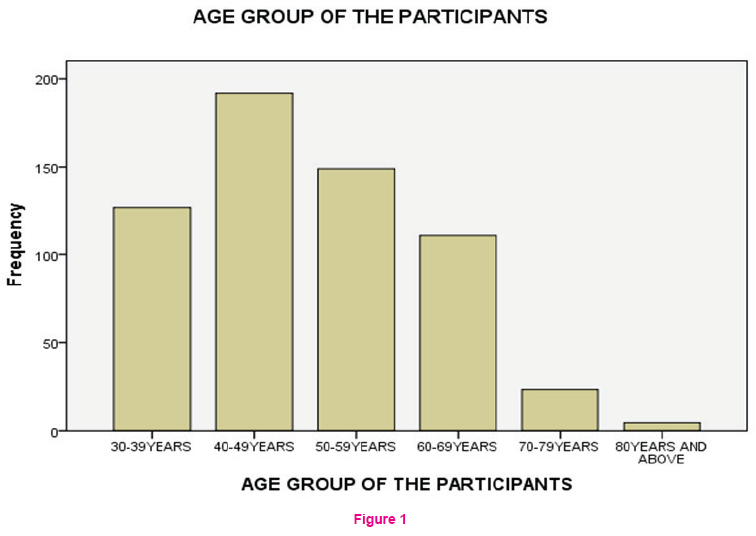
Results: Out of the 662 participants enumerated, six hundred and eight completed the interview and examination giving a response rate of 91.7% There were 369 females (60.7%) and 239 males with M:Fof 1:1.6 Age range was 30-86 years with a mean of 49.74 ±Standard Deviation 11.0 years Fig 1.
Two hundred and seventeen participants had lens opacities in the Right eye (35.69%). Fifty five (9.04%) had “cataracts “ ( visually disabling lens opacities). Tables 1 and 2 showed an overview of all participants with lens opacities in both eyes. This implied that while some might require surgery as soon as possible others will require surgery later. The result of the Right eye was similar to the Left therefore the Right eye was used for analysis.
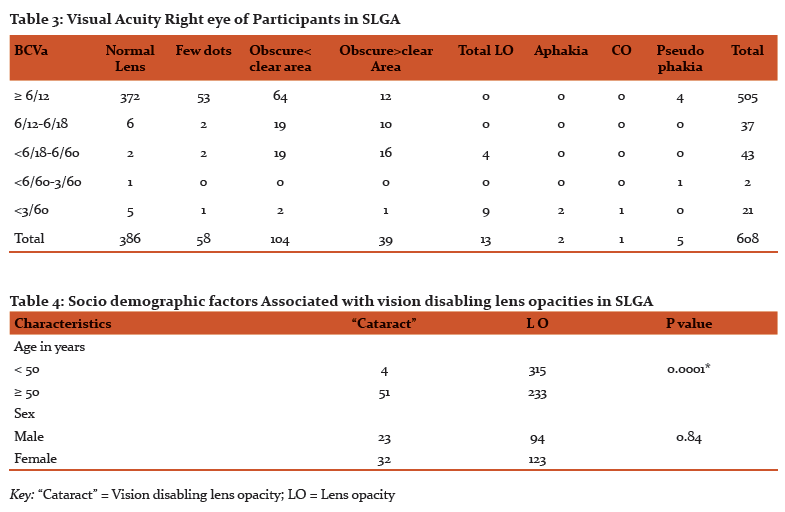
Five hundred and forty two participants out of 608 (89.14%) had no visual impairment i.e. vision ≥6/18 in their Right eyes. Sixty six (10.85%) had visual impairment (vision≤ 6/18) Table 3. Best corrected visual acuity showed that 10 participants were blind (visual acuity<3/60) in each eye from “cataracts”(3.28%). Five participants were pseudophakic in the Right eye out of which four (80%) had no visual impairment. Two participants were aphakicin the Right eye with severe visual impairment while one had corneal scar obscuring view of the lens. No lens was couched in either eye.
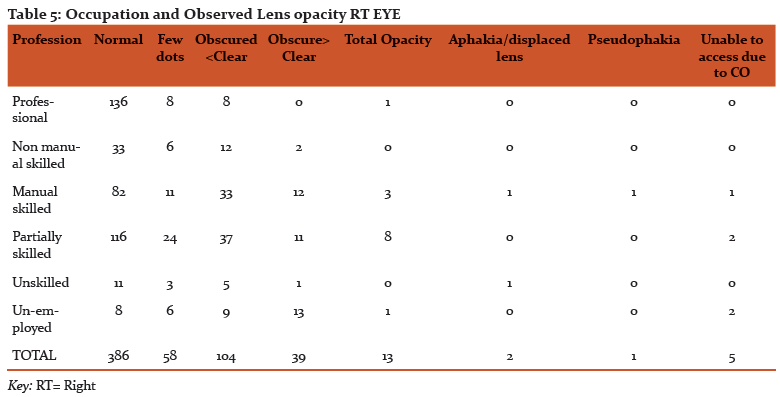
Fifty-one out of the 55 with cataracts were aged 50 and above (92.72%). This was statistically significant Fishers exact= 0.0001 Table 4. Also “cataracts” were found in non- professionals 51 out of 55 (92.72%) participants, which was also significant- Fishers exact =0.0001 Table5. “Cataracts” were more common in females than males 32 out of 55(63.63%). However this was not statistically significant p value= 0.84. Participants whose maximum education was primary school 19% (43 out of 226) were more likely to have “cataracts” than those with higher education 3% (9 out of 279) and this was statistically significant chi-square p<.0001 95% confidence interval 3.3797-14.9213.
The teaching hospital of Olabisi Onabanjo University at Sagamu was the only government facility for cataract surgery. There are four consultant ophthalmologists who provided cataract surgery which is presently Small Incision Cataract Surgery with intra ocular lens implant. Cost of surgery gradually rose from USS 50$ to USS 150$ in the last 20 years. Cataract surgery was not regular during the study period. Cataract surgery was supplemented by voluntary organizations working in Abeokuta about 50 km away. Although services were free to the people transportation cost and in availability of escort prevented many patients from assessing this offer. .
Discussion.
The prevalence of cataract amongst participants older than 30 years in SLGA was found to be
9.04% which is similar to the study done by Kolawole et al, but lower than that of Adegbeingbe et al in similar geographical area.[1,14]However in Adegbeingbe’s study all those with lens opacities were designated as having cataracts. “Cataracts” were more common in older participants above the age of 50 years similar to previous studiesand confirming that old age is a risk factor for cataracts.[4]Lens opacities was more common in females than males as in other studies.[1,14] Also cataracts as defined in this study was more common in females.
“Cataracts” causing visual impairment, 55 of 608 (9.04%) were more common amongst the unemployed and elderly in the society. The participants that had operable cataracts, those that had uni-ocular blindness and visual impairment were indicative of the cataract burden in SLGA. Several researchers had found that in low income countries, the low standard of living, and the cultural predisposition of the people to matters pertaining to health do not allow for early medical consultation. [9] These attributes also hindered cataract surgical uptake. [19,7] In order to access health care in these countries patients often pay out of pocket to the service provider. The expenses were not subsidized or reimbursed by the state or insurance scheme.[20] Although most of our patients had access to a tertiary center where they could seek eye care there was financial barrier which was made worse by the high unemployment rate of their wards.[21] The economic recession in the country and by extension Sagamu local government had indirectly caused visual impairment in the elderly not to be a priority problem in the family. The benefit of cataract surgery for the elderly should be promoted to involve the whole family not just the patient. These benefits included improvement in their quality of life which was beneficial to the whole family.[10,6] It was noteworthy that no lens was couched in SLGA unlike the findings of The Nigerian blindness survey, Odugbo et al in the middle belt of Nigeria and Kolawole et al in the rural towns of South West Nigeria.[4,22,1] This might be due to the peri- urban status of SLGA and nearness to Lagos – Nigeria’s commercial center with both status creating awareness of attendance in hospital for ailments. Itinerant “couchers” were more in villages where access to eye care workers was poor.
Education also affected the number of those that had cataracts. The less educated were more likely to wait longer for surgery because of ignorance, less demand on higher visual acuity and a belief that elderly people were not meant to see clearly. Also illiterates were more likely to have financial challenges reducing access to surgery.
The only facility for cataract surgery was the teaching hospital. The barrier to regular surgery in this tertiary center is from un-sustained infrastructural development due to limited resources and cost of surgery.[20] There are economic and political challenges which are beyond the capability of the hospital such that maintenance of instruments and replacement of faulty instruments are difficult. It is suggested that health policies of the State and Local Government should also focus on non- communicable diseases especially cataract blindness. Hitherto efforts to improve on surgical care are being driven by academics and institutions without the people themselves demanding for it.[20] Free cataract surgery for the elderly should be seen as a cost effective venture.[11] Both State Government (Ogun state) and Local Government have different roles to play. The state government can provide infrastructure and employment of ophthalmologists while the local government through the staff provide health education and screening for cataract surgery. Cost of surgery- part payment or total payment can be taken up by the Local government as part of health service to the elderly. Lin and co- workers found a high acceptance of free surgery amongst the elderly in urban China in a setting similar to SLGA.[13]
In SLGA there is a need to include cataract screening services in the health centres. It is therefore necessary to provide training for doctors, nurses and community extension workers in the health centers to recognize cataracts in children and adults and refer appropriately.[23] One of the centrally placed Local government health centers can be equipped with a theatre to bring services closer to the people and user fees reduced to a minimum. The teaching hospital can provide resource persons for the training. Collaboration between the teaching hospital and SLGA health centres is essential for increase in cataract surgical uptake.
Outreach services in which patients are screened outside the hospital premises and brought in for operation had been found to increase cataract surgical uptake.[24] This is more evident when payments for surgery are removed or reduced. However it was noted that such practices cannot be sustained unless government is involved.[25] The experience in this study is that government pay for accommodation and feeding of voluntary organizations that came to operate without providing essential equipment for ophthalmologist in the locality so that when the voluntary organizations leave surgery was suspended until the next visit.
Conclusion
In conclusion the prevalence of cataract blindness in Sagamu Local Government Area was high and is a cause for concern. Participants with only primary school education and non-professionals were more likely to have un-operated cataracts. Participants did not present early for surgery. Both state and Local Government should be ready to take responsibility for increase uptake in cataract surgery.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles were cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles journals and books from where the literature for this article has been reviewed and discussed.
The authors acknowledge the video clip designed by Dr Peter Abikoye.
DECLARATION. The authors declare no conflict of interest in this article
References:
1. Kolawole O, Mahmoud A, Adeoti C, Ashaye A. Cataract blindness in Osun state, Nigeria: Results of a survey. Middle East Afr J Ophthalmol. 2012;19(4):364-71
2. Ackland P, Resnikoff S, Bourne R. World blindness and visual impairment: despite many successes, the problem is growing. Community Eye Health J. International Centre for Eye Health; 2017 ;30(100):71–3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29483748[acessed 2018 May 28, 2pm]
3. Aboobaker S, Courtright P. Barriers to cataract surgery in Africa: A systematic review. Middle East African Journal of Ophthalmology. 2016;23(1):145-149
4. Rabiu MM, Kyari F, Ezelum C, Elhassan E, Sanda S, Gudlavalleti V. S, Sivasubramaniam MS et al. Review of the publications of the Nigeria national blindness survey: Methodology, prevalence, causes of blindness and visual impairment and outcome of cataract surgery. Ann Afr Med. 2012;11(3):125–30.
5. WHO | Blindness: Vision 2020 - The Global Initiative for the Elimination of Avoidable Blindness. WHO [Internet]. World Health Organization; 2010 [cited 2018 May 31]; Available from: http://www.who.int/mediacentre/factsheets/fs213/en/
6. Groessl EJ, Liu L, Sklar M, Tally SR, Kaplan RM, Ganiats TG. Measuring the impact of cataract surgery on generic and vision-specific quality of life. Quality of Life Research. 2013;22:1405–14.
7. Okoye O, Eze BI, Chuka-okosa CM. Eliminating the barriers to uptake of cataract surgery in a resource ? poor setting?: A focus on direct surgical cost. Niger J Clin Pract. 2015;18(3):10–3.
8. Gyasi M, Amoaku W, Asamany D. Barriers to Cataract Surgical Uptake in. Ghana Med J. 2015;41(4):167–70.
9. Khan MNA, Ansari MA, Ahmad A, Maroof M. a Study To Assess the barriers for cataract surgery uptake among elderly population of Aligarh. Int J community Med public Heal. 2017;4(11):4219–23.
10. Geneau R, Lewallen S, Bronsard A, Paul I, Courtright P. The social and family dynamics behind the uptake of cataract surgery: Findings from Kilimanjaro region, Tanzania. Br J Ophthalmol. 2005;89(11):1399–402.
11. Mitsuhiro MH, Berezovsky A, Belfort R, Ellwein LB, Salomao SR. Uptake, Barriers and Outcomes in the Follow-up of Patients Referred for Free-of-Cost Cataract Surgery in the Sao Paulo Eye Study. Ophthalmic Epidemiol. 2015;22(4):253–9.
12. Rabiu MM, Jenf M, Fituri S, Choudhury A, Agbabiaka I, Mousa A. Prevalence and causes of visual impairment and blindness, cataract surgical coverage and outcomes of cataract surgery in Libya. Ophthalmic Epidemiol. 2013;8:27-32
13. Lin H, Lin D, Long E, Jiang H, Qu B, Tang J, et al. Patient participation in free cataract surgery: A cross-sectional study of the low-income elderly in urban China. BMJ Open. 2016;6(4):1–8.
14. Adegbehingbe BO, Majengbasan TO. Ocular health status of rural dwellers in south-western Nigeria. Aust J Rural Health. 2007;15(4):269–72.
15. Babalola OE. The peculiar challenges of blindness prevention in Nigeria: a review article. Afr J Med Med Sci. 2011;40(4):309–19.
16. Adio A. The Rivers State, Nigeria Eye Care Program--the first few steps towards achieving V2020. Nigerian journal of medicine. 2011. p. 250–5. Available from: http://www.scopus.com/inward/record.url?eid=2-s2.0-82255179725&partnerID=tZOtx3y1 cited on april 20 2018
17. Ajibode, HA, Fakolujo V, Onabolu O, Jagun O, Ogunlesi T, Abiodun O. a Community-Based Prevalence of Presbyopia and Spectacle Coverage in Southwest Nigeria Une Predominence De Presbyopie a Base Communautaire Et Le Taux De Lunettes Au Sud-Ouest Du Nigeria. J.WACS.2016;6(4):66–82.
18. Araoye M .O. Research Methodology with statistics for health and social sciences. Nathadex Publishers. 2004: pg 119
19. Kessy JP, Lewallen S. Poverty as a barrier to accessing cataract surgery: A study from Tanzania. Br J Ophthalmol. 2007;91(8):1114–6.
20. Ologunde R, Maruthappu M, Shanmugarajah K, Shalhoub J. Surgical care in low and middle-income countries: Burden and barriers. Int J Surg. 2014;12(8):858–63. Available from: http://dx.doi.org/10.1016/j.ijsu.2014.07.009
21. Salami CGE. Youth unemployment in Nigeria?: A time for creative intervention. Int J Bus Mark Manag www.resjournals.org/IJBMM. 2013;1(2):18–26.
22. Odugbo O, Aboje A, Chiroma M, Mpyet C. Cataract blindness, surgical coverage, outcome, and barriers to uptake of cataract services in Plateau State, Nigeria. Middle East Afr J Ophthalmol. 2012;19(3):282-8.
23. Zhang XJ, Liang YB, Liu YP, Jhanji V, Musch DC, Peng Y, et al. Implementation of a free cataract surgery program in rural China: A community-based randomized interventional study. Ophthalmology. 2013;120(2):260–5.
24. Finger RP, Kupitz DG, Holz FG, Chandrasekhar S, Balasubramaniam B, Ramani R V., et al. Regular provision of outreach increases acceptance of cataract surgery in South India. Trop Med Int Heal. 2011;16(10):1268–75.
25. Lewallen S, Roberts H, Hall A, Onyange R, Temba M, Banzi J, et al. Increasing cataract surgery to meet Vision 2020 targets; experience from two rural programmes in East Africa. Br J Ophthalmol. 2005;89:1237–40.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





