IJCRR - 10(11), June, 2018
Pages: 11-19
Date of Publication: 11-Jun-2018
Print Article
Download XML Download PDF
Antioxidant Efficacy of Black Tea and Green Tea Equally Modulates Vasculogenic Factors in Preeclamptic Placental Trophoblast: A Comparative Study
Author: Padmini Ekambaram, Christina Joseph Mary Susai
Category: Healthcare
Abstract:Aim: Preeclampsia is hypertensive disorder of human pregnancy. Trophoblast, a prime cell of the placenta, is affected during preeclampsia due to the imbalance between oxidant and antioxidants resulting in aberrant cellular vascularization. Vasculogenesis is regulated by the endothelial nitric oxide synthase (eNOS), a potent vasodilator, regulating the expression of growth factors. Vascular endothelial growth factor (VEGF) is a prime regulator of vasculogenesis. Placental growth factor (PLGF) plays a crucial role in placental development during pregnancy. Synthetic drugs can hardly be used under complicated pregnancy. The requirement for herbal remedies renders essential regulatory mechanism to ensure adequate protection from preeclampsia.
Methodology: In the current study, black tea and green tea were used to assess the stress markers (LPO and TAC) and vasculogenic factors (ADMA, eNOS, VEGF-C, and PLGF) in normotensive and preeclamptic placental trophoblast.
Results: The increased expression of LPO, ADMA and decreased TAC, eNOS, VEGF-C, PLGF were observed in preeclamptic placental trophoblast. On tea incubation, vasculogenic proteins were significantly altered in preeclamptic placental trophoblast when compared with their respective subjects.
Discussion: Our present study results reveal that protective effect of black tea is equal to the green tea. This may be due to the tea polyphenols produces a beneficiary effect in the case of the preeclamptic placenta.
Conclusion: The present study concludes that tea with or without fermentation process has a significant impact on crucial vasculogenic factors. This effect can be suitably exploited to avoid further complications in preeclamptic pregnancy.
Keywords: Hypoxia, Preeclampsia, Tea, Trophoblast and Vasculogenic factors
Full Text:
INTRODUCTION
Preeclampsia is a pregnancy-specific disorder characterized by the development of hypertension and proteinuria; it is a leading cause of materno-fetal morbidity and mortality.(1) The etiology of preeclampsia has not been defined. However, Julian and his colleagues(2) reported that hypoxia might serve as an essential factor in the pathophysiology of preeclampsia. In the present study, placental trophoblast was analyzed as they are the structural unit of the placenta and it plays a crucial role in placental development, mediated by the invasion of extravillous trophoblast into the endometrium.(3) This, in turn, regulates the blood perfusion in the fetus during normal pregnancy. Improper trophoblast invasion plays a critical role in propagating endothelial dysfunction associated with preeclampsia resulting in the poorly perfused placenta with vascular dysfunction. Asymmetric dimethylarginine serves as the prime factor for mediating the endothelial dysfunction via endothelial nitric oxide synthase inhibition under hypoxic conditions.(4)
Nitric oxide is synthesized through constitutive calcium sensitive isoforms; nitric oxide synthase, i.e., endothelial nitric oxide synthase and neuronal nitric oxide synthase, or by inducible isoform (inducible nitric oxide synthase) which is calcium?independent.(5) Nitric oxide is a pleiotropic molecule, regulates diverse biochemical and physiological function including regulation of vascular tone, vascular remodeling, and protection against stress-induced cell damage.(6) The formation of nitric oxide by placental nitric oxide synthase and its following release in the intervillous space prevents platelet adhesion and aggregation; thereby it increases the blood flow to the placental villi leading to vasorelaxation.(7) Establishment of the proper cellular vascular system is essential during pregnancy and is mainly regulated by endothelial nitric oxide synthase through its impact on the expression of growth factors.(8)
Vascular endothelial growth factor plays a potential role in fetoplacental vessel formation by the processes of vasculogenesis and angiogenesis leading to the placental development.(9) Vascular endothelial growth factor is a 45 kDa disulphide linked homodimeric glycoprotein. The vascular endothelial growth factor family contains seven homologies such as vascular endothelial growth factor A, B, C, D, E, F, and placental growth factor, which all have a common vascular endothelial growth factor homology domain.(10) In the present study, placental trophoblasts determine the vascular endothelial growth factor-C expression for adult tissues prominently expressed vascular endothelial growth factor-C in heart, placenta, ovary, small intestine, and the thyroid gland. The actions of vascular endothelial growth factor are mediated through kinase domain receptor and soluble form of fms-like tyrosine kinase receptors. (11) Expression of vascular endothelial growth factor-C in the placenta can increase vascular permeability, stimulate the migration and proliferation of endothelial cells, through its binding to vascular endothelial growth factor receptor 2 and 3/sFLT-4 receptor.(12) Adequate and organized interaction of vascular growth factors and their receptors are required for proper placental vascular development.(9)
Placental growth factor is a homodimeric glycoprotein, 46-50 kDa in size, belongs to the vascular endothelial growth factor sub-family.(13) During pregnancy, expression of placental growth factor in villous trophoblast is essential for trophoblast invasion to the maternal decidua resulting in proper placentation and angiogenesis.(14) Placental growth factor regulates endothelial cell survival and proliferation by activating extracellular signal-regulated kinase 1 and 2 activity. Hence, the limited expression of placental growth factor in placental tissue is used as a predictive marker for preeclampsia.
Management of preeclampsia with natural remedy having vasodilating property is essential to improve placental blood flow and preclude hypertension. Various medications including antihypertensive, anticonvulsants and corticosteroids are available for managing preeclamptic complications. However, they are found to cause extreme side effects to both mother and fetus. Hence natural remedy is recommended to manage complications. Previously, our laboratory established the beneficiary effect of black tea on placental cells.(15) The present study riveted on evaluating the effect of black tea on vasculogenic factors in preeclamptic placental trophoblast in comparison with green tea. Both black tea and green tea are derived from the same plant Camellia sinensis, unique in its diverse medicinal properties.(16) Tea is the second most-consumed beverage in the world. Tea is also recommended as complementary and alternative medicines due to its anti-stress, anti-inflammatory and vasodilatory properties.(17) These properties may be attributed to the bioavailability of its key components present in green tea and black tea such as catechins and theaflavins which directly acts against or neutralizes the free radicals at the cellular level.(18) So far, the beneficiary effect of black tea and green tea on vasculogenic factors during preeclampsia is not explored in preeclamptic placental trophoblast. Therefore, our study aims to inquire the efficacy of black tea and green tea by analyzing the expression of vasculogenic factors in before and after tea incubation.
MATERIALS AND METHODS
Selection of subjects
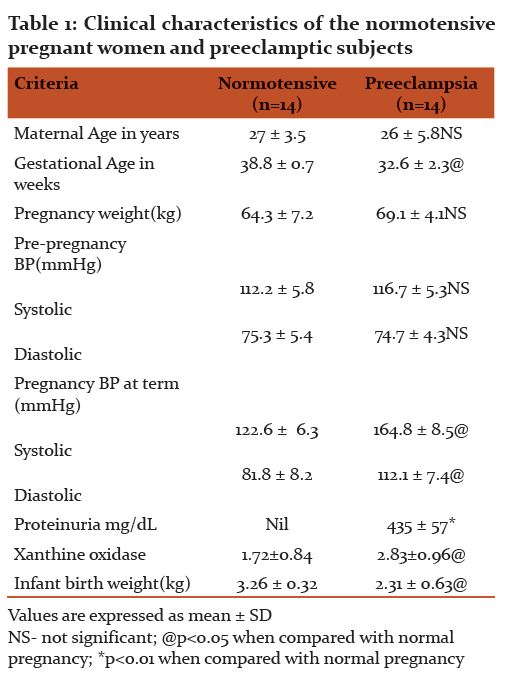
Patient registered in a public sector hospital in Chennai were enrolled in this study. Clearance was obtained from Institute Ethical Committee (IEC/S/BWC/609/2014) prior to the commencement of study and the informed consent was received from all the subjects (Table-1). Placenta was collected from both normal (n=14) and preeclamptic (n=14) pregnant women in the age group of 20-40 years, post delivery. Patients with preeclampsia were defined on the basis of the following laboratory criteria: blood pressure >140/90 mmHg but <160/110 mmHg, proteinuria >300 mg/L and xanthine oxidase activity of approximately 2.6 units/ mg protein.(19) Patients with severe preeclampsia and other severe maternal complications were excluded from the study.
Isolation of placental Trophoblast
Third-trimester villous trophoblast cells, which were used for comparison, were isolated from term placentas by the method of Douglas and King.(20) Human term placenta from the preeclampsia and normotensive subjects were obtained immediately after delivery in accordance with the established guidelines of the institutional ethical committee along with the informed consent of the patient. Briefly, placental villi were cut and thoroughly washed to remove blood. Thereafter, they were incubated four times in a enzyme digestion medium composed of HBSS, containing trypsin and deoxyribonuclease for 30 min at 37ºC in a water bath with continuous shaking. The dispersed cells were layered on top of a discontinuous 5–70% Percoll gradient, and centrifuged for 25 min at 507 Xg. The intermediate layers (density between 1.048 & 1.062) containing cytotrophoblast cells were removed and washed and following trophoblast isolation, cells were seeded at a density of approximately 1.6×106 cells per plate in a 5 mL cell culture plate. The complete culture medium, constituted of M199, 2mm glutamine & 10% FBS. All the experiments were performed within a day of trophoblast isolation in-order to overrule the influence of cultivation process.
Cell viability by MTT assay
The viability of placental trophoblast cells was determined using the MTT assay (Mosmann).(21) The trophoblast cells were resuspended in PBS buffer and serially diluted to a concentration of 200 mg of protein per mL of suspension using the same buffer system. One hundred mL of the dilutions were plated out into the wells of a microtiter plate in duplicate. In the control wells, PBS alone was incubated to provide the blank for absorbance readings. Ten mL of MTT reagent was added to each well, including controls. After incubation for 1 h, the visualized purple precipitate (formazan product) was solubilised with 1 mL acidic isopropanol. The plates were covered and left in the dark for 4 h at room temperature. Absorbance was measured at 560 nm. The relative viability was calculated by dividing the optical density of sample by the optical density of control well having the PBS buffer solution with MTT reagent, and multiplying by 100.
Estimation of protein
The protein concentration was estimated by the method of Bradford(22) the use of bovine serum albumin as the standard. The result was expressed as mg protein/g. The lysate was used for the estimation of the following parameters.
Preparation of black tea and green tea extracts
About 2 grams of commercially available South Indian black tea and green tea leaves were brewed and extracted with 100 mL of PBS by heating for 10 minutes. The extract was filtered using Whatmann filter paper (No.2). The resulting filtrate was diluted (1:100) with PBS and was diluted to get the necessary concentration of 2%.
Incubation studies
The isolated placental trophoblast from both normotensive and preeclamptic groups were incubated with 0.02% of black tea and green tea in 5% CO2 atmosphere at 37°C, for a maximum of 48 hrs.
Estimation of lipid peroxide
Lipid peroxide analysis was determined by the method of Ohkawa et al.(23) The lipid peroxide content was expressed as nanomoles of MDA/ mg of protein.
Estimation of total antioxidant capacity
Total antioxidant capacity analysis was performed by the method of Prieto et al.(24) The total antioxidant activity was expressed as Trolox equivalent in mmol/ L.
Quantification of stress signaling molecules
The expression of signaling molecules were quantified by using asymmetric dimethyl arginine (MBS264847), endothelial nitric oxide synthase (SEA868Hu), vascular endothelial growth factor-C (E-EL-H1600), placental growth factor (SEA114Hu), according to the manufacturer’s instructions.
Statistical analysis
Data were analyzed using statistical software package version 7.0. Student’s t-test and SPSS package were used to ascertain the significance of variations between normotensive and preeclamptic trophoblast. All data were presented as mean ± SD of 14 samples. Differences were considered significant at pNS, p<0.05, p<0.01 and p<0.001.
RESULTS
Comparison of clinical characteristics between normotensive and preeclamptic subjects
Table 1 depicts that the normotensive and preeclamptic subjects were no significant changes in the maternal age and weight, meanwhile gestational age was significantly decreased in the preeclamptic subjects (p<0.05) when compared to normotensive subjects. Likewise, there was a moderately significant increase in the blood pressure (p<0.05), the level of proteinuria (p<0.001) and XO activity (p<0.05) in preeclampsia. However, low birth weight baby was significantly increased by p<0.05 in preeclamptic subjects than in normal pregnancy.
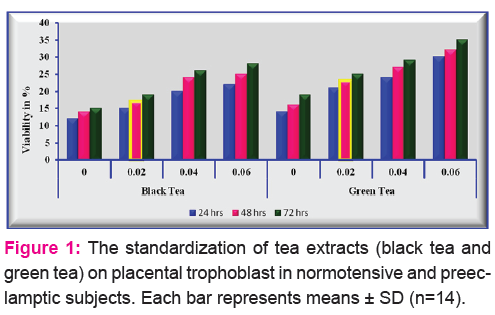
Standardization of tea (black tea and green tea) extracts
The viability of placental trophoblast was determined by using MTT assay. The percentage difference of placental trophoblast viability is depicted in Figure 1. The concentration of tea extracts for both black tea and green tea (0.02%, 0.04% and 0.06%) was standardized in our laboratory at different time intervals (24hours, 48hours and 72hours). The result indicated that 0.02% of tea extracts incubated for 48hours is more effective to study the placental cells changes.
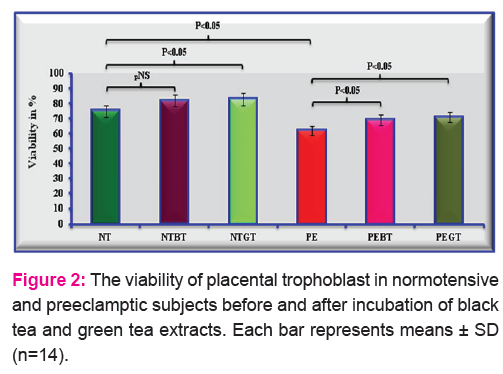
Cell viability
The viability of placental trophoblast was assessed by MTT assay which represents the % difference. Viability of preeclamptic trophoblast was decreased by 17% (p<0.05) when compared to normotensive trophoblast (Figure 2). On tea incubation, cell viability was preserved by black tea (11%) and green tea (14%). It shows that cell viability was insignificantly decreases in preeclamptic cell after infusion of tea extracts when compared with before incubation of preeclamptic placental trophoblast.
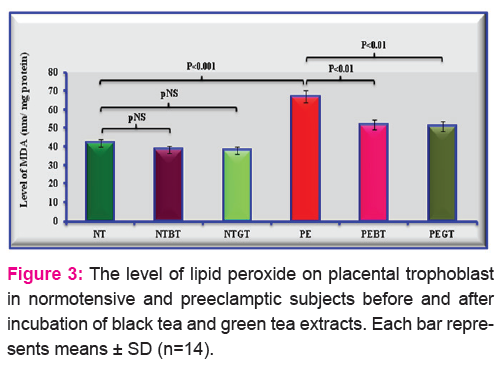
Lipid peroxide
The level of lipid peroxide in placental trophoblast on normotensive and preeclampsia before and after treatment of black tea and green tea incubation was expressed in Figure 3. The level of lipid peroxide was increased by 60% (p<0.001) in preeclamptic placental trophoblast when compared to normotensive placental trophoblast. Upon incubation with black tea and green tea, lipid peroxide was decreased by 22% and 24% in preeclamptic trophoblast compared to without incubation of preeclamptic placental trophoblast.
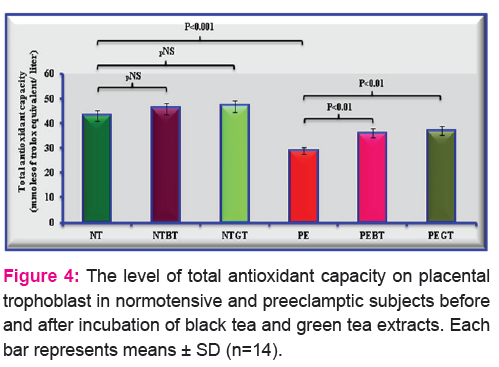
Total antioxidant capacity
Figure 4 depicts that the level of total antioxidant capacity in placental trophoblast on normotensive and preeclamptic subjects with and without incubation of black tea and green tea extracts. The level of total antioxidant capacity was decreased in preeclamptic trophoblast by 33% when compared to normotensive trophoblast without tea incubation. Upon tea incubation, the level of total antioxidant capacity was increased in normotensive trophoblast by 24% (black tea) and 28% (green tea) in preeclamptic trophoblast compared to preeclamptic placental trophoblast without any incubation.
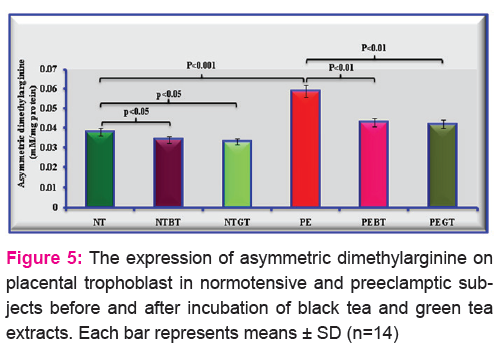
The quantification of asymmetric dimethyl arginine
The level of asymmetric dimethyl arginine in placental trophoblast on normotensive and preeclampsia before and after incubation of black tea and green tea infusion was showed in Figure 5. The quantification of asymmetric dimethyl arginine was increased by 55% in preeclamptic placental trophoblast compared with normotensive placental trophoblast. After incubated with black tea and green tea incubation the level of asymmetric dimethyl arginine was significantly decreased by 27% and 29% in preeclamptic placental trophoblast when compared with their respective subjects.
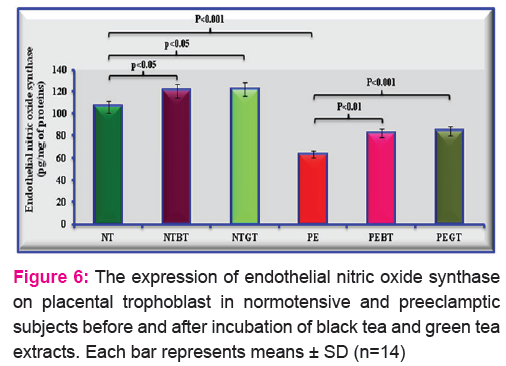
The expression of endothelial nitric oxide synthase
Figure 6 describes that the expression of endothelial nitric oxide synthase in placental trophoblast on normotensive and preeclamptic subjects with and without incubation of black tea and green tea extracts. The level of endothelial nitric oxide synthase was decreased in preeclamptic trophoblast by 40% when compared to normotensive trophoblast without any incubation. Lateron, placental trophoblast cells treated with tea incubation such as black tea and green tea extracts at that time the expression of endothelial nitric oxide synthase was increased by 29% (black tea) and 32% (green tea) in preeclamptic trophoblast compared to preeclamptic placental trophoblast without any incubation.
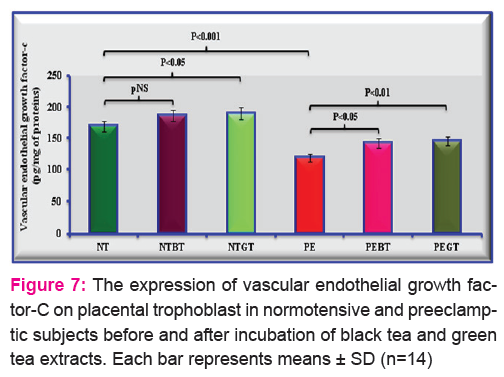
The expression of vascular endothelial growth factor-C
The expression of vascular endothelial growth factor-C in placental trophoblast on normotensive and preeclamptic subjects with and without incubation of black tea and green tea extracts was depicted in Figure 7. The level of vascular endothelial growth factor-C was decreased in preeclamptic placental trophoblast by 30% when compared to normotensive trophoblast without any incubation. Followed by tea incubation the expression of vascular endothelial growth factor-C was increased by 20% (black tea) and 23% (green tea) in preeclamptic trophoblast compared to preeclamptic placental trophoblast without any incubation.
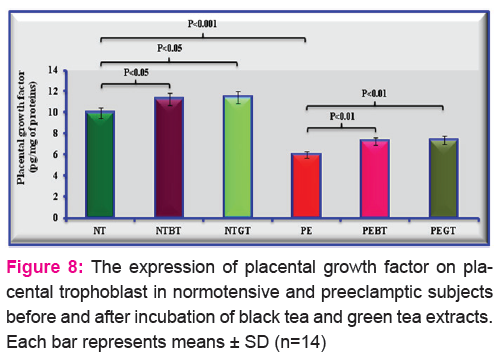
The quantification of placental growth factor
The expression of placental growth factor in placental trophoblast on normotensive and preeclamptic subjects with and without incubation of black tea and green tea extracts was described in Figure 8. The quantification of placental growth factor was decreased in preeclamptic placental trophoblast by 40% when compared to normotensive trophoblast without any incubation. Subsequently tea incubation the level of placental growth factor was increased by 21% (black tea) and 23% (green tea) in preeclamptic placental trophoblast when compared with preeclamptic placental trophoblast without tea incubation.
DISCUSSION
The present study investigated the herbal remedies of black tea and green tea on preeclamptic placental trophoblast by analyzing the oxidant-antioxidant status and vasculogenic factors. Previous studies on preeclamptic placenta demonstrated that black tea had a beneficiary role in modulating the stress markers, stress proteins, and their associated signaling molecules to render cellular homeostasis.(25,15,26) It also suggested that inbuilt antioxidant capacity of black tea may be attributed to its beneficiary role. Hence in the present study effect on black tea in comparison with green tea was executed to check their antioxidant potential in the placenta during preeclampsia. The concentration having maximum antioxidant efficacy was analyzed by determining trophoblast viability on incubation with both tea’s (black tea & green tea) at different concentration (0.02%, 0.04%, and 0.06%) for varying time intervals (24hrs, 48hrs, and 72hrs). From this, it reveals that 0.02% of tea infusion incubated for 48hrs was most effective in preserving the trophoblast viability, and it was utilized for further analysis. Whereas, 0.04% and 0.06% concentration for 24hrs, 48hrs and 72hrs were not found to be effective in maintaining trophoblast viability depicted by Figure 2. 0.02% of black tea and green tea for 48hrs altered the oxidant-antioxidant status, which is observed from decreased lipid peroxide and increased total antioxidant capacity level. It is suggesting that it may be due to the bioavailability of polyphenols present in both black tea and green tea. It exhibits similar antioxidant and vasodilatory effects on preeclamptic placental trophoblast.
Endothelial-dependent vascular dysfunction is a central pathophysiological feature of preeclampsia,(27) occurs due to the impaired nitric oxide synthesis. Many studies reported that elevated concentrations of asymmetric dimethyl arginine act as an endogenous inhibitor on all isoforms of nitric oxide synthase, which contribute to endothelial-dependent vascular dysfunction in diabetes, hypertension, hypercholesterolemia, and obesity.(28) In addition to preventing nitric oxide production, by acting as a competitive inhibitor, asymmetric dimethyl arginine also promotes the uncoupling of nitric oxide synthase enzymatic activity and convert nitric oxide synthase to a superoxide generator. This uncoupling activity of asymmetric dimethyl arginine may contribute to vascular dysfunction and may play a role in the pathophysiology of preeclampsia by serving as a source of vascular oxidative stress. Consistently, decreased expression of endothelial nitric oxide synthase was noted in preeclamptic conditions reflecting the enhanced expression of asymmetric dimethyl arginine. Simultaneously, the effect of tea on the expression of asymmetric dimethyl arginine and endothelial nitric oxide synthase were assessed, which demonstrates that bioavailability of tea polyphenols serve as the better source of antioxidant with the vaso-regulator property, portrayed from the increased expression of endothelial nitric oxide synthase on tea incubation in preeclamptic placental trophoblast. Similarly, Jochmann et al.,(29) reported that tea is rich in a high concentration of polyphenols and can increase endothelial nitric oxide synthase activity and nitric oxide production, resulting in endothelial-dependent vasodilation in human umbilical vein endothelial cells and bovine aortic endothelial cells.
Current study observed that the expression of asymmetric dimethyl arginine was significantly increased in preeclamptic placental trophoblast when compared with normotensive placental trophoblast. Upon tea (black tea and green tea) incubation, the expression of asymmetric dimethyl arginine was decreased considerably in preeclamptic placental trophoblast. Marjan et al.,(30) has reported that asymmetric dimethyl arginine is an anti-angiogenic factor that reduces vascular endothelial growth factor expression in endothelial cells and prevents the formation of nitric oxide from nitric oxide synthase, which fits our data. Asymmetric dimethyl arginine affects the growth factors at their production and activity level.(31) Savvidou and his co-workers(32) also reported that increased expression of asymmetric dimethyl arginine serves as the causative factor for the development of preeclampsia, stating that regulation of asymmetric dimethyl arginine expression is essential for the management of preeclamptic complications. Consistent with this, our study demonstrated a decrease in asymmetric dimethyl arginine level on incubation with both black tea and green tea and its mediated effect on endothelial nitric oxide synthase level in the preeclamptic trophoblast is due to its bioactive component present in tea polyphenols. The tea polyphenols like epigallocatechin gallate and theaflavin may contribute the reviving of vasculogenic property in trophoblast isolated from preeclamptic placenta. Similarly, Tang et al.(33) described that tea polyphenols protect endothelial cells by increasing dimethylarginine dimethylaminohydrolase activity, which in turn results in a decrease in asymmetric dimethyl arginine level.
Simultaneously, vascular endothelial growth factor-C expression was also assessed and showed the decreased expression of vascular endothelial growth factor-C in preeclamptic placental trophoblast and its effect on trophoblast proliferation and invasion. The maternal decidua requires increased expression of vascular endothelial growth factor-C for the proper trophoblast invasion and establishment of the intervillous uteroplacental circulation during pregnancy. Borowicz et al.(34) also reported that both vascular endothelial growth factor and endothelial nitric oxide synthase plays a crucial role in the development of the placenta and any alteration in their expression may result in abnormal pregnancies. Consistent with this, we have noted a decrease in the expression of vascular endothelial growth factor-C in preeclamptic placental trophoblast suggesting its crucial role during pregnancy.
Another important growth factor, placental growth factor was also assessed in the trophoblast, and it was found to be decreased in preeclamptic placental trophoblast than normotensive. Nikolaos et al.(35) reported that low concentration of placental growth factor along with high level of its receptor soluble fms-like tyrosine kinase-1 is linked with impaired angiogenesis and placental development, leading to preeclampsia. It is suggested that necessity of placental growth factor expression establish the proper placental environment. Hence, the effect of black tea and green tea on placental growth factor in placental trophoblast was assessed. It depicts that polyphenols present in both black tea and green tea have a regulatory effect on placental growth factor expression. The absorption of tea polyphenols to the preeclamptic placental trophoblast is efficient to rescue from the induced oxidative stress.
Studies demonstrated that angiogenic growth factors such as vascular endothelial growth factor and placental growth factor are mediated through a nitric oxide-dependent mechanism. (36, 37) Consistently in the present study, a decrease in the expression of vascular endothelial growth factor-C and placental growth factor were noted in preeclamptic placental trophoblast, depicting that it may be due to the decreased nitric oxide, indirectly evidenced from reduced endothelial nitric oxide synthase and increased asymmetric dimethyl arginine. However, incubation of tea extracts in preeclamptic placental trophoblast has exhibited an increased expression of vascular endothelial growth factor-C and placental growth factor. It reveals that it may be attributed to the antioxidant efficacy of polyphenols present in black tea and green tea and its mediated effect on asymmetric dimethyl arginine. Thus the present study demonstrates that both black tea and green tea has the similar beneficiary effect in the management of preeclampsia by modulating asymmetric dimethyl arginine, which in turn leads to increase in the expression of endothelial nitric oxide synthase and angiogenic growth factors (Figure 9).
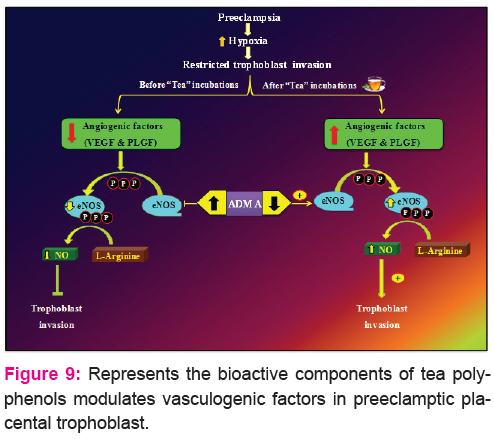
Figure 9 represents the vasculogenic factors are altered during hypoxia, which is pathologically restricted trophoblast invasion and endothelial function. During preeclampsia reduced expression of vascular endothelial growth factor-C (VEGF-C) and placental growth factor (PLGF) consequently, diminish the activation of endothelial nitric oxide synthase (eNOS). Under this circumstance increased expression of asymmetric dimethyl arginine (ADMA) affects the formation of nitric oxide from endothelial nitric oxide synthase, which depicts that the inhibition of trophoblast invasion. This leads to preclude of vasodilation among maternal and fetal circulation. So, for the therapeutic intervention of tea polyphenol helps to alter the angiogenic (vascular endothelial growth factor-C, placental growth factor & endothelial nitric oxide synthase) and antiangiogenic (asymmetric dimethyl arginine) factor in preeclamptic placental trophoblast. This may be due to the bioactive polyphenols present in tea efficiently renders the protection against excessive oxidative stress.
The beneficiary effect of both tea polyphenols on vasculogenic factors attributed to their efficient bioavailability property (sufficient absorption and potential biological effects). Though the supplemented polyphenols have the inbuilt antioxidant property, the execution of real properties relies on the polyphenols bioavailability. Alexander,(38) reported that equal efficacy of both teas is measured in blood plasma. Thus, the present study depicts that green tea and black tea exhibits a similar effect on stress markers and vasculogenic factors in recovering the placental cell damage under preeclamptic conditions.
CONCLUSION
The present study concludes that the beneficiary effect of black tea and green tea are similarly exhibited on key vasculogenic factors evidenced by the absorption of tea polyphenols on preeclamptic placental trophoblast by ex-vivo model. Since black tea has the equal efficacy in modulating anti-angiogenic and pro-angiogenic factors, and it is easily affordable to the common people, black tea can be supplemented during pregnancy to manage pregnancy complications like preeclampsia. The bioactive components of tea can also be suitable for the therapeutic purpose, although more in-vivo models should confirm the same.
ACKNOWLEDGEMENTS
The project funded by National Tea Research Foundation, Tea Board of India. Project referral number- NTRF: 163/2013 and NTRF: 192/2016 is acknowledged.
CONFLICT OF INTEREST
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References:
-
Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet. 2010; 376:631–644.
-
Julian CG, Galan HL, Wilson MJ, Desilva W, Cioffi-Ragan D, Schwartz J, Moore LG. Lower uterine artery blood flow and higher endothelin relative to nitric oxide metabolite levels are associated with reductions in birth weight at high altitude. Am J Physiol Regul Integr Comp Physiol. 2008;295:R906–R915.
-
Buttery LDK, McCarthy A, Springall DR: Endothelial nitric oxide synthase in the human placenta: Regional distribution and proposed regulatory role at the fetomaternal interface. Placenta. 1994, 15: 257-265.
-
Stuhlinger MC, Stanger O 2005 Asymmetric dimethyl-l-arginine (ADMA): a possible link between homocyst(e)ine and endothelial dysfunction. Curr Drug Metab 6:3–14.
-
Knowles RG and Moncada S (1994) Nitric oxide synthases in mammals. Biochem J 298,249–258.
-
Sladek., S.M, Magness., R.R, and Conrad., K.P, 1997. Nitric oxide and pregnancy. Am. J. Physiol., 272, 441-463.
-
Benirschke KK, Kaufmann P: Pathology of the human Placenta. New York: Springer-Verlag. 1995, 182-189.
-
Jozef Dulak, Jessy Deshane, Alicja Jozkowicz and Anupam Agarwal, 2008. Heme Oxygenase-1 and Carbon Monoxide in Vascular Pathobiology Focus on Angiogenesis. Circulation.117:231-241.
-
Dunk C and Ahmed A, 2001. Expression of VEGF-C and activation of its receptors VEGFR-2 and VEGFR-3 in trophoblast. Histol Histopathol: 16: 359-375.
-
Ann H, Bart L, Martin SH, Hans W, Allan TVO, Ernst ADB, 2004. Vascular endothelial growth factor and angiogenesis. Pharmacol Rev 56: 549-580.
-
Terman BI, Dougher-Vermazen M & Carrion ME 1992 Identification of the KDR tyrosine kinase as a receptor for vascular endothelial cell growth factor. Biochemical and Biophysical Research Communications 187 1579–1586.
-
Joukov V, Pajusola K, Kaipainen A, Chilov D, Lahtinen I, Kukk E, Saksela O, Kalkkinen N & Alitalo K 1996 A novel vascular endothelial growth factor, VEGF-C, is a ligand for the Flt4 (VEGFR-3) and KDR (VEGFR-2) receptor tyrosine kinases. EMBO Journal 15 290–298.
-
Maglione, D., Guerriero, V., Viglietto, G. et al. (1991) Isolation of a human placenta cDNA encoding for a protein related to the vascular permeability factor. Proc. Natl Acad. Sci. USA , 88, 9267–9271.
-
Desai J, Holt-Shore V, Torry RJ, Caudle MR, Torry DS. Signal transduction and biological function of placenta growth factor in primary human trophoblast. Biol Reprod. 1999;60:887–892.
-
Padmini E, Kalyani G, Christina J.M.S., 2015a. Antioxidant Reviving Role of Mint-Tea on Placenta During Gestational Diabetes Mellitus. International Journal of Science and Research 4(3): 501-507.
-
Sano M, Takahashi Y, Yoshino K, Shimoi K, Nakamura Y, Tomita I, Oguni I and Konomotor H, 1995. Effect of tea (Camellia sinensis L.) on lipid peroxidation in rat liver and kidney: a comparison of green and black tea feeding. Biological Pharmaceutical Bulletin 18:1006-1008.
-
Yang CS, PrabhuS and Landacl L, 2001. Prevention of carcinogenesis by tea polyphenols. Drug Metab Rev 33: 237-253.
-
Wu YY, Li W, Xu Y, Jin EH and Tu YY, 2011. Evaluation of the antioxidant effects of four main theaflavin derivatives through chemiluminescence and DNA damage analyses. J Zhejiang Univ-Sci B (Biomed & Biotechnol) 12(9):744-751
-
Brown M A, Lindheimer M D, Swiet M D, Assche A V and Moutquin J M (2001). “The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP)”. Hypertension in Pregnancy ; 20: 9-14.
-
Douglas GC, King BF. Isolation of pure villous cytotropho- blast from term human placenta using immunomagnetic microspheres. Journal of Immunological Method, 1989; 119:259–268.
-
Mosmann T (1983) Rapid colorimetric assay for cellular growth and survival: application to proliferation and cytotoxicity assays. J Immunol Methods 65:55–63
-
Bradford MM. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Analytical Biochemistry, 1976; 72:248-254.
-
Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxides in animal tissue with thiobarbituric acid reaction. Anal Biochem, 1970; 95: 352-35.
-
Prieto P, Pineda M, Aguilar M. Spectrophotometric quantitation of antioxidant capacity through the formation of phosphomolybdenum complex, Specific application to the determination of vitamin E. Analytical Biochemistry, 1999; 26(9): 337-341.
-
Padmini E., 2011. HSP70 expression and its role in preeclamptic stress. Indian Journal of Biochemistry and Biophysics. 48: 243-255.
-
Padmini E, Christina Joseph Mary S, Tharani J and Shiela L, 2015b. Modulatory effect of black tea on survival and apoptotic proteins in placental trophoblast and explants during preeclampsia. Journal of Pharmacy Research: 9(4); 2015: 201-210.
-
Roberts JM. Objective evidence of endothelial dysfunction in preeclampsia. American Journal of Kidney Diseases. 1999;33:992–994.
-
Cooke JP. Asymmetrical dimethylarginine: the Uber marker? Circulation. 2004;109:1813–1818.
-
Jochmann, N, Lorenz, M, Krosigk, A, Martus, P, Bohm, V, Baumann, G, Stangl, K, Stangl, V, 2008. The efficacy of black tea in ameliorating endothelial function is equivalent to that of green tea, Br. J. Nutr. 99: 863–868.
-
Marjan Noorbakhsh, Maryam Kianpour and Mehdi Nematbakhsh, 2013. Serum Levels of Asymmetric Dimethylarginine, Vascular Endothelial Growth Factor, and Nitric Oxide Metabolite Levels in Preeclampsia Patients. ISRN Obstetrics and Gynecology. Article ID 104213: 5.
-
Smith CL, Birdsey GM, Anthony S, Arrigoni FI, Leiper JM, Vallance P. Dimethylarginine dimethylaminohydrolase activity modulates ADMA levels, VEGF expression, and cell phenotype. Biochemical & Biophysical Research Communications. 2003; 308:984–989.
-
Savvidou, M.D.; Hingorani, A.D.; Tsikas, D.; Frolich, J.C.; Vallance, P.; Nicolaides, K.H. Endothelial dysfunction and raised plasma concentrations of asymmetric dimethylarginine in pregnant women who subsequently develop pre-eclampsia. Lancet 2003, 361, 1511–1517.
-
Tang WJ, Hu CP, Chen MF, Deng PY, Li YJ. Epigallocatechin gallate preserves endothelial function by reducing the endogenous nitric oxide synthase inhibitor level. Can J Physiol Pharmacol 2006; 84: 163-71.
-
Borowicz PP, Arnold DR, Johnson ML, Grazul-Bilska AT, Redmer DA, Reynolds LP, 2007. Placental growth throughout the last two thirds of pregnancy in sheep: vascular development and angiogenic factor expression. Biol Reprod ; 76(2):259-67.
-
Nikolaos Vrachnis, Emmanouil Kalampokas, Stavros Sifakis, Nikolaos Vitoratos, Theodoros Kalampokas, Demetrios Botsis & Zoe Iliodromiti., 2013. Placental growth factor (PlGF): a key to optimizing fetal growth. The Journal of Maternal-Fetal & Neonatal Medicine 26 (10). http://dx.doi.org/10.3109/14767058.2013.766694.
-
Fukumura D, Gohongi T, Kadambi A, Izumi Y, Ang J, Yun CO, et al. Predominant role of endothelial nitric oxide synthase in vascular endothelial growth factor-induced angiogenesis and vascular permeability. Proceedings of the National Academy of Sciences of the United States of America. 2001;98:2604–2609.
-
Papapetropoulos A, Garcia-Cardena G, Madri JA, Sessa WC. Nitric oxide production contributes to the angiogenic properties of vascular endothelial growth factor in human endothelial cells. Journal of Clinical Investigation. 1997;100:3131–3139.
-
Alexander GGT. Advances in oral anticoagulation treatment: the safety and efficacy of rivaroxaban in the prevention and treatment of thromboembolism. Ther Adv Hematol. 2012 3(5): 309-323.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





