IJCRR - 10(9), May, 2018
Pages: 22-26
Date of Publication: 05-May-2018
Print Article
Download XML Download PDF
A Study on Comparision of Diagnostic Efficiency between Modified Alvarado Score and Graded Compression Ultrasonography in the Case of Acute Appendicitis
Author: Malay Kumar Barman, Kaustav Das, Koel Mukherjee
Category: Healthcare
Abstract:Background: Several diagnostic aids have been developed to improve diagnosis in suspected acute appendicitis. Modified Alvarado Score includes signs and symptoms associated with ones degree of clinical suspicion. Graded Compression Ultrasonograpy
is used in many institutions to aid the diagnosis of acute appendicitis.
Aim: The aim of present study is to compare and evaluate diagnostic accuracy of Modified Alvarado Score and Graded Compression Ultrasonography in co-relation to histopathology report for diagnosis of acute appendicitis.
Methodology: A cross-sectional study of 75 patients who underwent appendectomy for suspected acute appendicitis have been considered and were evaluated by Modified Alvarado Score and Graded Compression Ultrasonography, which was correlated
with histopathological findings.
Result: Out of 75 patients, 29 patients (38.66%) had acute appendicitis. In the present study, modified Alvarado Score has sensitivity of 76.86%, specificity 82.61%, positive predictive value 73.33%, negative predictive value 84.44%, diagnostic accuracy 80.0%, false positive error rate 17.39% and false negative error rate 24.11%. Graded Compression Ultrasonography has sensitivity of 82.76%, specificity 89.13%, positive predictive value 82.76%, negative predictive value 89.13%, diagnostic accuracy 86.67%, false positive error rate 10.87% and false negative error rate 17.24%.
Conclusion: From the findings, the present study intended to conclude that it is highly clinically suggestive that the Modified Alvarado Score should be combined with Graded Compression Ultrasonography for better diagnosis of acute appendicitis.
Keywords: Modified Alvarado Score, Graded Compression Ultrasonography, Acute appendicitis
Full Text:
INTRODUCTION
Abdominal pain is the primary presenting complaint of patients with acute appendicitis.1,2,3 The diagnostic sequence of colicky central abdominal pain followed by vomiting with migration of the pain to the right iliac fossa was first described by Murphy but may only be present in 50% of patients.4,2 It may progress to perforation which is associated with higher morbidity and mortality.5 Hence, surgeons are inclined to operate when diagnosis is probable rather than to wait till it is certain.6 Acute appendicitis is the most common cause of acute surgical abdomen with a lifelong risk of 7%.7 Despite its high incidence, classic clinical and laboratory findings usually allow for diagnosis which is not so easy due to atypical and frequently confusing presentation which leads to misdiagnosis.8 Therefore, diagnosis of Acute Appendicitis remains challenging despite improvement in history taking, clinical examination, and new computer aided decision support system, clinical diagnostic sourcing and new imaging technique.
Several different approaches have been developed to improve diagnosis in suspected acute appendicitis and to decrease negative appendectomies (removal of normal appendix in patients with other causes of abdominal pain) such as predictive scoring system, computer aided diagnosis, inflammatory marker, and computed tomography.9, 10, 11
Graded Compression Ultrasonography in diagnosis of acute appendicitis has greatly improved the ability to diagnose acute appendicitis with ultrasound, was first described in 1986 by J.B. Puylaert.11, 12, 13 It plays an important role in reducing the number of negative surgical exploration for acute appendicitis.
Modified Alvarado Scoring system is a dynamic one allowing observation and critical evaluation of the clinical.14, 15, 16, 17 Its application improved diagnostic accuracy and reduces negative exploration and complication rates.18 The description of modified Alvarado scoring system was introduced in 1994 has greatly improved ability to diagnosis.19
OBJECTIVE
To compare and evaluate diagnostic accuracy of Modified Alvarado Score and Graded Compression Ultrasonography in co-relation to histopathology report for diagnosis of acute appendicitis.
METHODOLOGY
The present study was a cross sectional study conducted in the Department of Surgery, North Bengal Medical College and Hospital during the period of April 2013 to August 2014. Total 75 Patients with age group 15-50 years, suspected clinically acute appendicitis and undergone appendicectomy in North Bengal Medical College, Siliguri were selected for the study. The clinical diagnosis of acute appendicitis was done by consultants of Department of Surgery, North Bengal Medical College and Hospital, Siliguri thorough evaluation of clinical details, investigation and Graded Compression Ultrasonography. The subjects were informed about the purpose of the study and the necessary ethical clearance has been obtained from ethical committee of the hospital before commencement of the present study.
Then depending on the clinical details and investigation, Modified Alvarado Score has been administered which is as follows: 20
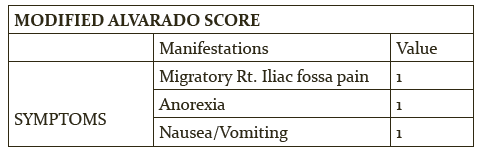
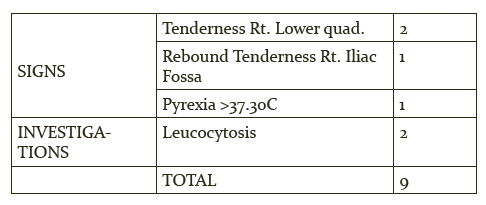
Modified Alvarado Score more than or equal to 7 were considered as acute appendicitis i.e. positive and scores less than or equal to 6 were considered as negative. On the other hand, the Graded Compression Ultrasonography findings were divided in two groups such as ultrasonography positive and ultrasonography negative.
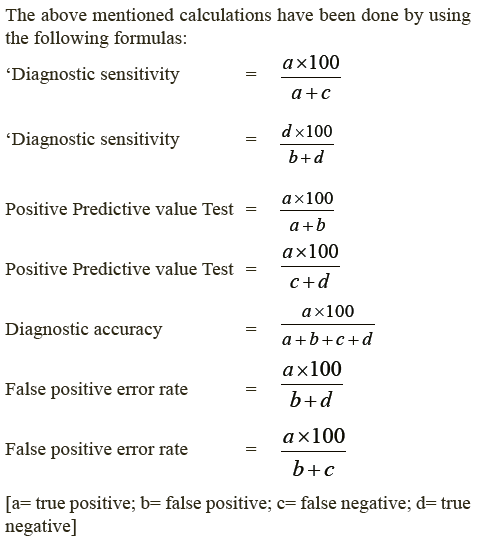
True positive, true negative, false positive and false negative cases were obtained through Modified Alvarado Score, Graded Comparison Ultrasonography and histopathological report. Sensitivity, specificity, positive predictive value, diagnostic accuracy etc were calculated and compared between Modified Alvarado Score and Graded Comparison Ultrasonography.
RESULTS:
Total 75 patients were considered for the present study. The table No. 1 demonstrated sex distribution of studied population. Total number of cases in the present study were 75, out of which, 45(60%) were male and 30 (40%) were females.
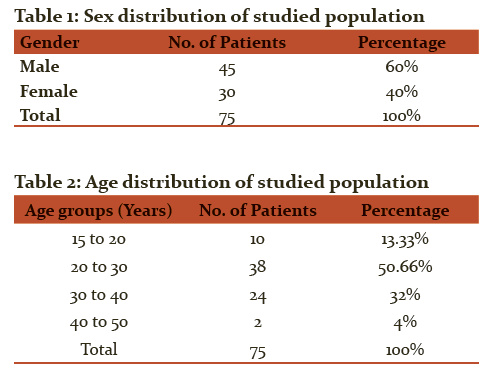
In the present study, the total number of patients has been categorized into four age groups, such as 15-20yrs, 20-30yrs, 30-40yrs and 40-50yrs. Maximum number of patients (50.66%) belonged to the age group 20-30yrs followed by the age group 30-40yrs (32%). Among the studied population, age group 40-50yrs exhibited minimum number of patients (4%).
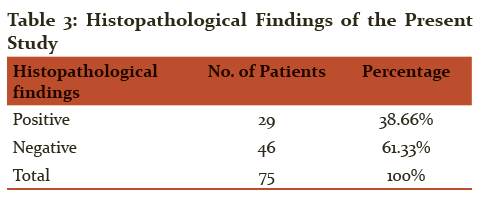
The table No. 3 demonstrated the histopathological findings of the present study where out of 75 patients undergone appendectomy, 29 (38.66%) were histologically positive for acute appendicitis and 46 (61.33%) were histologically negative.
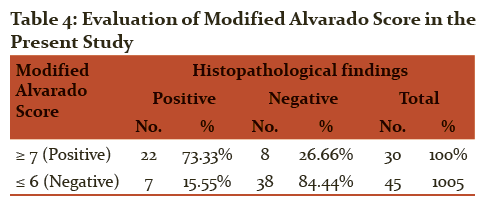
All the 75 patients were assigned modified Alvarado Score among which 40.00% were positive (≥ 7) and 60.00% were negative (≤ 6). In addition to that out of 30 Modified Alvarado score positive cases, 22 (73.33%) were histologically positive and 8 (26.66%) were negative. In the remaining 45 Modified Alvarado Score negative cases, 7 (15.55%) were histologically positive and 38 (84.44 %) were negative.
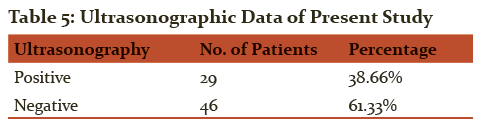
In the present study all the patients were undergone for ultrasonography. Out of which 29 (38.66%) were sonographically positive cases and 46 (6) were sonographically negative cases which indicated more negative cases than sonographically positive cases.
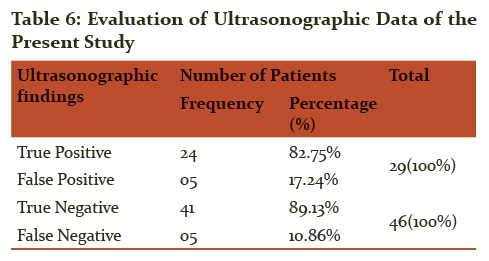
In the present study out of 29 sonographically positive cases, 24 (82.75%) were histologically positive and 05 (17.24%) were negative. In the remaining 46 sonographically negative cases 05 (10.86%) were histologically positive and 41 (89.13%) were negative.

In the present study, Modified Alvarado Score has sensitivity of 76.86%, specificity 82.61%, positive predictive value 73.33%, negative predictive value 84.44%, diagnostic accuracy 80.00%, false positive error rate 17.39% and false negative error rate 24.11%. Graded Compression Ultrasonography had sensitivity of 82.76%, specificity of 89.13%, positive predictive value of 82.76%, negative predictive value of 89.13%, diagnostic accuracy of 86.67%, false positive error rate of 10.87%, and false negative error rate of 17.24%. The sensitivity of Graded Compression Ultrasonography is less than specificity, because of number of false negatives, some of which cannot be controlled (poor tolerance by the patient, obesity, presence of gas and unusual location of appendix).
DISCUSSION:
The results of the present study have demonstrated evaluation of Alvarado Score and Ultrasonographic data separately and at the end comparison between these two diagnostic tool in case of acute appendicitis has been presented. When the results of present study are compared with contemporary studies, 21, 20 we observed that sensitivity, specificity, positive predictive value and negative predictive value are in corroboration with these studies. Whereas when compared with few other studies of Al-Hashemy et al; 22 Sooriakumaran et al 23 findings of low sensitivity have been found as these studies were retrospective studies.
The present study has shown better sensitivity, as it is a cross sectional study and short comings of retrospective study are ruled out like good documentation is needed, lack of recording of Modified Alvarado Score may indicate in complete recording in case notes of some patients rather than true absence of Modified Alvarado Score finding.
A meta analysis showed high sensitivity and specificity of Graded Compression Ultrasonography in diagnosis of acute appendicitis.24 Ultrasonographic data of the present study are compared to other research works where it was seen that sensitivity, specificity, positive predictive value and diagnostic accuracy of the present study is almost corroborative with those studies. 25, 26, 27
Furthermore, in present study, when Modified Alvarado Score and Graded Compression Ultrasonography were compared in terms of sensitivity, specificity, positive predictive value, diagnostic accuracy and false negative cases the results are almost same. Therefore, the result showed that neither one is significantly advantageous.
Thus Modified Alvarado Score is a useful tool in clinical decision making especially when Graded Compression Ultrasonography is unavailable. As imaging technique is considered to be expensive in India, Scoring system should be used in selection of patients for further work-up. Ultrasound is unnecessary when ones degree of clinical suspicious is high. However the additional information provided by graded compression ultrasound does improve diagnostic accuracy in case of negative or equivocal Modified Alvarado Score.
In the view of the finding of the present study, it can be said that the use of Graded Compression Ultrasonography along with Modified Alvarado Score will be most useful in increasing the diagnostic accuracy of acute appendicitis. It would be interesting to compare the assessment of these patients using Modified Alvarado Score one group and another group as Modified Alvarado Score combined with Graded Compression Ultrasonography in future study.
CONCLUSION
Thus it can be concluded that establishing diagnosis in cases of suspected acute appendicitis might require a combination of different diagnostic tools such as Modified Alvarado Score, investigative modalities such as ultrasonography and the indispensible clinical judgement. In other words, the Modified Alvarado Score should be combined with ultrasonography for the diagnosis of acute appendicitis. But nothing can replace careful evaluation by an experienced surgeon.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to the participants for their kind cooperation.
SOURCE OF FUNDING
Nil
CONFLICT OF INTEREST
None declared.
References:
-
Hisham MFS. Cardiothoracic surgical critical care: Principles, goals and direction. Int. J Surg 2012; 10(3): 111-14.
-
Humes DJ, Simpson J. Acute appendicitis. BMJ 2006; 333(7567):530-34. http://doi.org/10.1136/bmj.38940.664363.AE
-
Andy P. Diagnosis of acute appendicitis. Int. J Surg 2012; 10: 115-19.
-
Murphy J. Two thousand operations for appendicitis, with deductions from his personal experience. Am J Med Sci 1904; 128: 187-211.
-
Cueto García J, Ribé Bello J, Giorgiana LA, Cervantes Llaca C. Morbidity and mortality of appendicitis. Rev Gastroenterol Mex 1977 (Sep-Dec); 42(3):126-38.
-
Hoffmann J, Rasmussen O. Aids in the diagnosis of acute appendicitis. Br J surg 1989; 76:774-79.
-
Hardin DM. Acute Appendicitis: Review and update. Am Fam Physician 1999; 60:2027-34.
-
Becker T, Kharbanda A, Bachur R. Atypical clinical features of pediatric appendicitis. Acad Emerg Med 2007; 14(2):124-29.
-
Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med 1986; 15: 557-64.
-
Shoshtari MHS, Askarpour S, Alamshah M, Elahi A. Diagnostic value of Quantitative CRP measurement in patients with acute appendicitis. Pak J Med Sci 2006; 22:300-03.
-
Puylaert JB. Acute appendicitis: US evaluation using graded compression. Radiology 1986; 158(2);355-60.
-
Jeffrey RB, Laing FC, Lewis FR. Acute appendicitis: High-resolution real-time US findings. Radiology 1987; 163: 11-14.
-
Ramachandran P, Sivit CJ, Newman KD, Schwartz MZ. Ultrasonography as an adjunct in the diagnosis of acute appendicitis: A 4-year experience. J Pediatr Surg 1996; 31:164-69.
-
Ohle R, O'Reilly F, O'Brien KK, Fahey T, Dimitrov BD. The Alvarado score for predicting acute appendicitis: a systematic review. BMC Med 2011; 9: 139. http://doi.org/10.1186/1741-7015-9-139
-
Soomro AG, Siddqui FG, Abro AH, Abro S, Shaikh NA, Memon AS. Diagnostic accuracy of Alvarado scoring system in acute appendicitis. J Liaquat Univ Med Health Sci 2008; 7: 93-96.
-
Khan I, Rehman AU. Application of Alvarado scoring system in diagnosis of acute appendicitis. J Ayub Med Coll Abbotababad 2005; 17: 41-4.
-
Limpawattanasiri C. Alvarado score for the acute appendicitis in a provincial hospital. J Med Assoc Thai 2011; 94: 441-48.
-
Memon ZA, Irfan S., Fatima K., Iqbal M.S., Sami W. Acute appendicitis: Diagnostic accuracy of Alvarado scoring system. Asian J Surg 2013; 36(4): 144-49.
-
Kalen M, Rich AJ, Talbot DR, Canlitie WJ. Evaluation of modified Alvarado score in the diagnosis of acute appendicitis. A prospective study. Ann R ColI Surg Engl 1994; 76: 418-9.
-
Bhattacharjee PK, Chowdhary T, Roy D. Prospective evaluation of modified Alvarado score for diagnosis of acute appendicitis. JIMA 2002; 100(8): 310-12.
-
Sabiston, David C, Townsend, Courtney M, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. Philadelphia, PA: Elsevier Saunders, 2012. Print.
-
Al-Hashemy AM, Seleem MI. Appraisal of the modified Alvarado score for acute appendicitis in adults. Saudi Med J 2004; 25(9): 1229-31.
-
Sooriakumaran P, Lovell D, Brown R. A comparison of clinical judgment vs the modified Alvarado score in acute appendicitis. Int. J Surg 2005; :3 59-62.
-
Orr RK, Porter D, Hartman D. Ultrasonography to evaluate adults for appendicitis;Decision making based on metanalysis and probabilistic reasoning. Acad Emerg Med 1995; 2: 644-50.
-
Skaane P, Amland PF, Nordshus T, Solheim K. Ultrasonography in patients with suspected acute appendicitis. A prospective study. Br J Radio 1990; 63: 787-93.
-
Tarjan Z, Mako E, Winternitz T, Kiss I, Kalman A. The value of ultrasonic diagnosis in acute appendicitis. Orv Hetil 1995; 136: 713-17.
-
Chan I, Bicknell GS, Graham M. Utility and diagnostic accuracy of sonography in detecting Appendicitis in a community Hospital. AJR 2005: 184; 1809 -12.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





