IJCRR - 10(8), April, 2018
Pages: 01-09
Date of Publication: 28-Apr-2018
Print Article
Download XML Download PDF
Study on Environmental Factors Causing Head and Neck Cancer in Karachi, Pakistan
Author: Arifa Aziz, Yasmin Abdul Rashid, Zeenat Shaheen, Safia Awan
Category: Healthcare
Abstract:Objective: Head and neck cancer is one of the most prevalent cancers in South East Asia and its incidence is increasing with time. The objective of this study is to identify the environmental factors and their role in causing head and neck cancers for better future strategy in controlling and prevention.
Materials and Methods: Questionnaire form was developed, which includes questions about environmental factors causing head and neck cancer. Forms were filled by patients after taking their written consent. This study was conducted at Day Care Oncology and in Radiation department of Aga Khan University Hospital, after approval from institutional ethical review committee. It is a prospective study conducted from December 2016 to June 2017. Patients with head and neck cancer aged 18 years and above, of both genders were included. Statistical Package for the Social Sciences SPSS version 19 was used to perform statistical analysis.
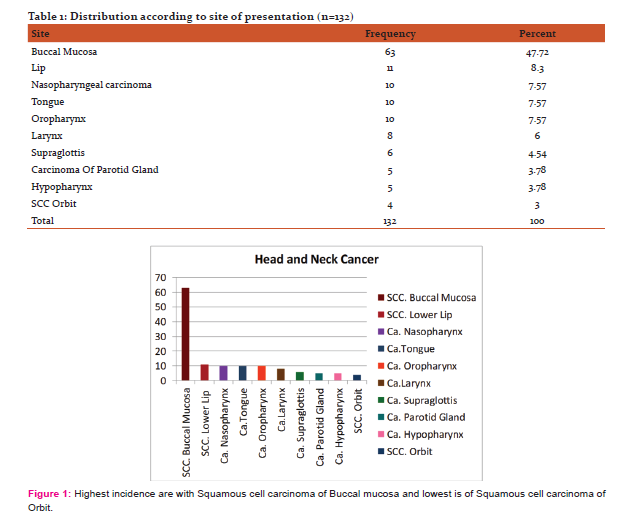
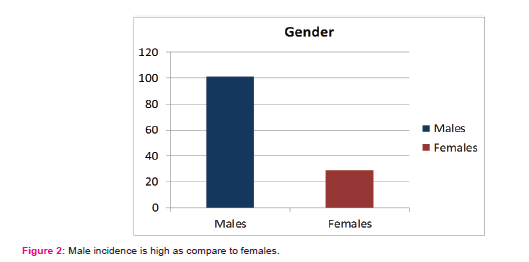
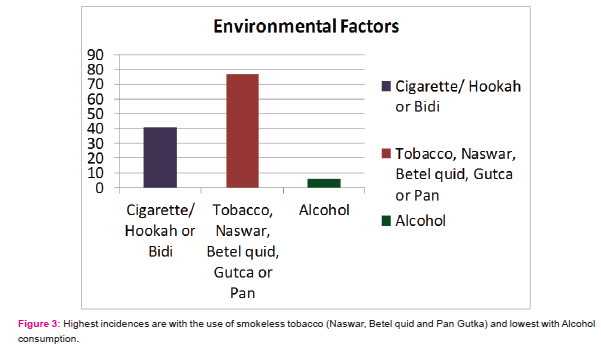
Results: A total of 132 patients were included. Head and neck cancers were observed to be more common in males 101 (76.5%) as compared to females 29 (22%) and average age was found to be 50.4 \? 12.9 years in both genders. The commonest environmental factors causing head and neck cancer included various forms of smokeless tobacco including pan, mainpuri, supari and gutka. 132 patients 77 (58.3%) were using smokeless tobacco, 41(31.1%) were cigarette smokers and 6 (4.5%) were using alcohol. Among all the head and neck cancers, the most common was squamous cell cancer of buccal mucosa 63 patients (47.72%) and less common is the cancer of orbit 4 patients (3%).
Conclusion: Incidence of head and neck cancer, specifically squamous cell carcinoma of buccal mucosa is increasing with time. The commonest cause was found to be different forms of smokeless tobacco easily accessible to the public. Increasing public awareness through various means is the way forward in controlling this menace.
Keywords: Smokeless tobacco, Buccal mucosa cancer, Public awareness Programs
DOI: 10.7324/IJCRR.2018.10801
Full Text:
Introduction:
Head and neck cancers are the most common cancers in developing countries (1)‚ especially in Southeast Asia. In the western population cigarette smoking and alcohol consumption are the main reasons for squamous cell carcinoma of head and neck whereas the use of smokeless tobacco and betel nut is the most common cause of head and neck squamous cell carcinoma in Southeast Asia. (2,3). Betel nut chewing is common in Pakistan and other Southeast Asian countries and is high risk factor in development of squamous cell carcinoma of buccal mucosa which is the most common type of oral cancers in Pakistan and India (4,5)‚ and oropharyngeal and tongue cancers are common in the Western world (6). These differences in site of disease may be related to the widespread habits in the respective regions. (7)
The different names in which smokeless tobacco is used in Pakistan and India include khaini, mava, paan (betel quid), zarda, snuff, mashiri, etc. (8) Smokeless tobacco both chewing tobacco and snuff is associated with an increased risk of cancer of the oral cavity and pharynx (9, 10) The incidence of laryngeal cancer and pharyngeal cancer, is approximately 50 percent higher in African American men (11). The outcome for head and neck squamous cell carcinoma of patients has not significantly improved in the past four decades even with great improvement in the skills, knowledge, surgical procedures and multi-disciplinary tumor boards establishments.(12) Regular awareness activities by health professionals and volunteers have not led to the improvements and it is observed that with many awareness programs which were conducted in various health centers for staff and public but analysis results showed that these programs are not very successful especially in control of factors causing this disease in Southeast Asia and the numbers of head and neck cancers are increasing every day both in rural and urban areas. There is a great need of government to help in control and stop the supply and use of various forms of smokeless tobacco which are the main causes of head and neck cancer and are easily available in the market.
There is a shortage of data on behavior and outcomes of these tumors from this region. The primary objective of this study is to share the demographics and identify various types of smokeless tobacco causing head and neck cancer and their control by increasing awareness programs.
Material and method:
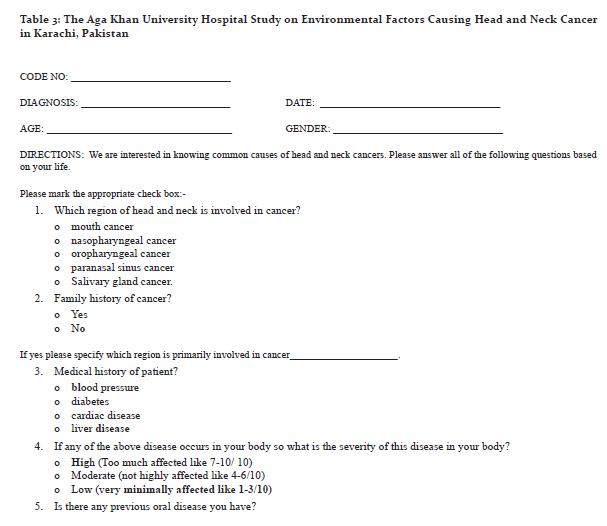
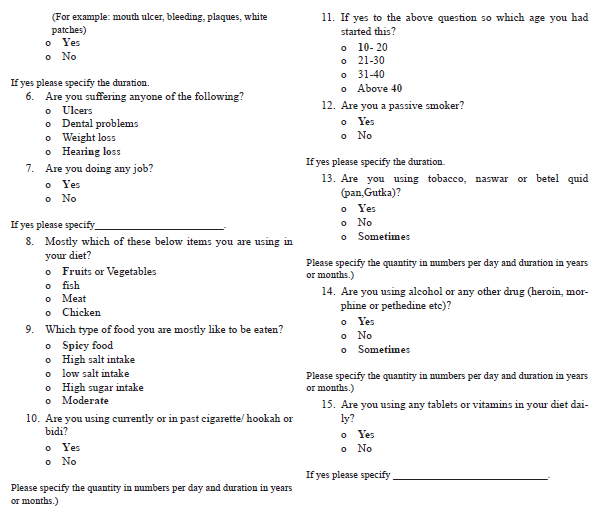
This study was conducted at day care oncology and radiation department at Aga Khan University Hospital. The study protocol was approved by the ethical review committee of Aga Khan University Hospital, Karachi, Pakistan, with ERC # 4392-Onc-ERC-16. Questionnaire form was developed by a multidisciplinary team of Medical Oncologist, staff medical officer and head nurse of day care oncology and radiation department, demographic data and questions about environmental factors causing head and neck cancer were included in the form as shown in table 3. These forms were filled by patients after explaining the study to them and taking their written consent.
Study Design:
It is a prospective, cross sectional study conducted from December 2016- June 2017.
Patients with head and neck cancer receiving treatment at our institute aged 18 years and above, of both genders were included in this study. Statistical Package for the Social Sciences (SPSS) version 19 was used to analyze the collected data.
Results:
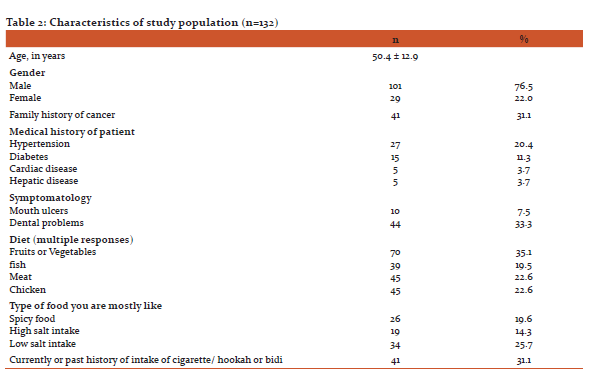
A total of 132 patients were included. There were 101 (76.5%) males as compared to females which were 29 (22%). Average age was 50.4 ± 12.9 years in both genders. Out of 132 patients 77(58.3%) were using various forms of smokeless tobacco, 41 patients (31.1%) were cigarette smokers and 6 patients (4.5%) were using alcohol. The most common site involved was squamous cell cancer of buccal mucosa observed in 63 patients (47.72%) and there were 4 patients (3%) of squamous cell cancer of orbit.
Discussion:
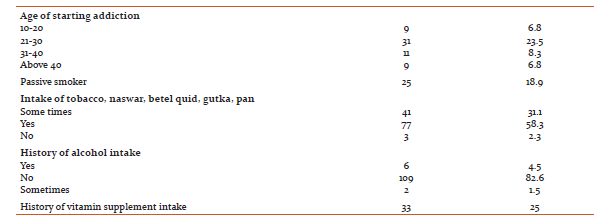
The incidences of head and neck cancers are increasing and are placed in the top ten malignancies globally (13). Squamous cell cancer of head and neck are placed sixth most frequently diagnosed cancer (14) and its proportion is much higher in males as compared to females with ratio of 2:1(15). This accounts for approximately one-fifth of all cancers in males and about one-tenth in females (16). Study on incidence and epidemiological characteristics of squamous cell cancer of head and neck was conducted in 1995-2002 in Karachi, results showed that approximately one-fifth (21%) of the head and neck cancers were seen in males and about one-tenth (11%) in females, buccal mucosa and larynx were the commonly affected sites, followed by pharynx. The mean age of the patients was 53.0 years (a rising incidence was observed in both genders, more apparent in males). About 30% of oral cancer cases, 28.6% of the nasopharyngeal, 6.3% of the oropharyngeal, and 2.6% of laryngeal cancers occurred in patients age 40 years and younger. The peak incidence was at 64-69 years for all three cancer sites, in both genders (17-19). If we compare results of study done in 1995-2002 with our study conducted in 2017, the results are almost the same with no improvement. There is no significant difference in results indicating that a lot of efforts which were done to decrease incidence of head and neck cancer were failed. Pakistan falls into a high risk zone for head and neck squamous cell carcinoma. (20). Poor nutrition, oral hygiene and dental problems may increase the risk of getting head and neck cancer. (21) In our study 44 patients (33.3%) had dental problems as shown in table-2. The exact reason of relationship between poor nutrition and head and neck cancer is not known. Heavy alcohol drinkers often have vitamin deficiencies, which may help explain the role of alcohol in increasing risk of these cancers. A good balanced diet can be associated with decreased risk of this disease. Diet has strong evidence with cancer development and data confirmed an apparent underlying relationship for a decreased head and neck squamous cell carcinoma risk with non-starchy vegetables, fruits, and food containing carotenoids. A recent study established that higher dietary pattern scores, with high intake of fruit and vegetable and low intake of red meat, were associated with decrease risk of squamous cell carcinoma. (22)
Finally, the importance of primary prevention needs to be highlighted. Check on the supply and the use of various forms of smokeless tobacco, areca nut, betel leaf, etc. as far as tobacco use few studies showed that it is difficult to change people's attitude and convince them to stop smoking. (23). In our study a total of 132 patients were included, patient's information was collected from patients in chemotherapy unit and radiation department at Aga Khan University Hospital Karachi, Pakistan. Analysis report showed that Head and neck cancers are observed to be more common in male 101 (76.5%) as compare to females 29 (22%) and average age is 50.4 ± 12.9 years in both genders as shown in figure-2. The commonest environmental factor causing head and neck cancer includes smokeless tobacco and tobacco chewing and out of 132 patients 77 (58.3%) were using them as shown in figure -3.Among all the head and neck cancers the most common is squamous cell cancer of buccal mucosa 63 patients (47.72%) and less common is the squamous cell cancer of orbit 4 patients (3%) as shown in figure-1. If both, results of 2002 and 2017 study, when compared are almost the same with very less difference in outcome showing that there is no improvement in control of head and neck cancer and there is a great need to think and apply some powerful strategy that can work in control of head and neck cancer. Squamous cell cancer of head and neck in Pakistan's is the next great health challenge. There is an urgent need to improve awareness about the disease and to introduce population based cancer registration and early detection programs. In addition, health services organization and human resources need to work together in developing plans to help prevent and fight with this disease. Finally, the importance of primary prevention needs to be highlighted. Limiting the use and removal of various forms of smokeless tobacco, areca nut, betel leaf, cigarette smoking and alcohol is perhaps the most suitable way to begin with. However it is very difficult to change current social attitudes, practices and perceptions in control of tobacco (23). Ninety percent of the oral cancer patients in rural areas belong to the lower or lower-middle socio-economic class, and 3.6% are below the poverty line based on Pareek's classification (24). Around 75% to 80% of patients with cancers present with late stage incurable disease and hence increased mortality (25), reason of delay could be both by patient in visiting doctor and in few cases physician related delay both of which contributes towards the late diagnosis. (26) another reason for delay in diagnosis in rural areas is the lack of easy access to healthcare, with one study demonstrating a delay of 67.5 days and 53.7 days in obtaining a first appointment for rural and urban patients, respectively. Other reasons of delay included poor socio-economic status of the patient, cost of care, and high rate of illiteracy (27). Great work was done during last many years and improvement in surgical procedures and establishment of multi-disciplinary tumor boards were done, but the results are the same with no improvement in the outcome for head and neck squamous cell carcinoma and it was seen that there is no significant improvement in the past four decades (28). As serious consequences of this rapidly developing epidemic are now becoming clear and it is very important to develop effective mechanisms that can be used to control this disease. This will require a deeper analysis of the risk factors, of the population at risk and of the treatment resources that are available, unfortunately this is the common problem with most of the developing world. The study of Kumar et al.11 showed that smoking cessation reduces but does not eliminate the risk of this cancer development, However, Marron et al.12 confirmed that cessation of tobacco smoking protect against the head and neck Squamous cell carcinoma development. The major risk factor for oral cancers among non-drinkers is tobacco use and among non-smokers is alcohol use (29, 30).
Conclusion:
In this field, there is urgent need of more research to find new ways in prevention and understanding in development of head and neck carcinomas and to improve therapeutic approaches and interventions. Now adays, the most effective measures to improve the prognosis of the head and neck cancers are prevention and early diagnosis.
Way forward
Awareness programs should be conducted for public and for general practitioner in rural and urban areas, this will help in both ways prevention plus early diagnosis.
Strict actions should be taken by government to stop manufacturing and supply, in market, of factors like various forms of smokeless tobacco which is the main cause of head and neck cancer in Karachi, Pakistan.
Acknowledgement
We are grateful to Afsheen Feroz head nurse day care and radiation oncology for her suggestions in preparing questionnaire form and all authors of references we have cited in our manuscript.We would also like to thank patients for their participation.
References:
- WHO 2008. The global burden of disease: 2004 update. Available at: www.who.int/evidence/bod (accessed January 27, 2014)
- Graham S. Dentition, diet, tobacco and alcohol in the epidemiology of oral cancer. J Natl Cancer Inst. 1977; 59:1611–18. [PubMed]
- Dayal PK, Mani NJ, Bhargava K. Prevalence of oral cancer and precancerous lesions in ‘pan’/'supari' chewers. Indian J Public Health. 1978; 22:234-45. [PubMed]
- Guha N, Warnakulasuriya S, Vlaanderen J, Straif K. Betel quid chewing and the risk of oral and oropharyngeal cancers: a meta-analysis with implications for cancer control. Int J Cancer 2014; 135:1433.
- Znaor A, Brennan P, Gajalakshmi V, et al. Independent and combined effects of tobacco smoking, chewing and alcohol drinking on the risk of oral, pharyngeal and esophageal cancers in Indian men. Int J Cancer 2003; 105:681.
- Bhurgri Y, Bhurgri A, Usman A, et al. Epidemiological review of head and neck cancers in Karachi. Asian Pac J Cancer Prev. 2006; 7:195–200. [PubMed]
- Sankaranarayanan R, Masuyer E, Swaminathan R, Ferlay J, Whelan S. Head and neck cancer: a global perspective on epidemiology and prognosis. Anticancer Res. 1998; 18:4779–86. [PubMed]
- Mehta FS, Hamner JE. Tobacco Habits in India In: Tobacco-Related Oral Mucosal Lesions and Conditions in India. New Delhi, India:Jaypee Brothers; 1993. pp. 89–99.
- Proia NK, Paszkiewicz GM, Nasca MA, et al. Smoking and smokeless tobacco-associated human buccal cell mutations and their association with oral cancer--a review. Cancer Epidemiol Biomarkers Prev 2006;15:1061.
- Sapkota A, Gajalakshmi V, Jetly DH, et al. Smokeless tobacco and increased risk of hypopharyngeal and laryngeal cancers: a multicentric case-control study from India. Int J Cancer 2007; 121:1793.
- Rosenquist K, Wennerberg J, Schildt EB, et al. Use of Swedish moist snuff, smoking and alcohol consumption in the etiology of oral and oropharyngeal squamous cell carcinoma. A population-based case-control study in southern Sweden. Acta Otolaryngol 2005; 125:991.
- DeSantis C, Naishadham D, Jemal A. Cancer statistics for African Americans, 2013. CA Cancer J Clin 2013; 63:151.
- Carvalho AL, Singh B, Spiro RH, Kowalski LP, Shah JP. Cancer of the oral cavity: a comparison between institutions in a developing and a developed nation. Head Neck 2004; 26: 31-8.
- Asian pac j cancer prev. 2006 apr-jun;7(2):195-200
- Akram, s., et al., emerging patterns in clinicopathological journal of medical sciences, 2013. 29 (3): p. 783
- Deepti Garg, Charu Kapoor, Swati Gautam. MODERATELY DIFFERENTIATED SQUAMOUS CELL CARCINOMA: A CASE SERIES. Dental Journal of Advance Studies. 2014: 46-50
- Bhurgri Y. Cancer Oral Cavity Trends in Karachi South, Asian Pac J Cancer Prev. 22005; 6:22-6.
- Bhurgri Y, Bhurgri A, Usman A, Pervez S, Kayani N, Bashir I, et al. Epidemiological review of head and neck cancers in Karachi. Asian Pac J Cancer Prev 2006; 7:195-200.
- Bhurgri Y, Bhurgri A, Parvez S, Bhurgri M, Kayani N, Ahmed R, et al. Cancer profile of Hyderabad, Pakistan1998–2002. Asian Pac J Cancer Prev 2005;6:474–80
- Zheng TZ, Boyle P, Hu HF, Duan J, Jian PJ, Ma DQ, Shui LP, Niu SR, Scully C, MacMahon B: Dentition, oral hygiene, and risk of oral cancer:A case-control study in Beijing. Cancer Causes Control 1: 235–241, 1990
- Carvalho AL, Singh B, Spiro RH, Kowalski LP, Shah JP. Cancer of the oral cavity: a comparison between institutions in a developing and a developed nation. Head Neck 2004; 26: 31-8.
- Carvalho AL1, Singh B, Spiro RH, Kowalski LP, Shah JP. Cancer of the oral cavity: a comparison between institutions in a developing and a developed nation. Head Neck. 2004 Jan; 26 (1) :31-8.
- Carvalho AL1, Pintos J, Schlecht NF, Oliveira BV, Fava AS, Curado MP, Kowalski LP, Franco EL. Predictive factors for diagnosis of advanced-stage squamous cell carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg. 2002 Mar; 128 (3) :313-8.
- Maher R, Devji S. Prevalence of Smoking among Karachi Population J Pak Med Assoc 2002; 52: 250-2
- Pareek U, Trivedi G. Manual of Socio-Economic Status Scale (Rural) New Delhi: Manasayan Publishers; 1995.
- Pai SA. Gutkha banned in Indian states. Lancet Oncol. 2002; 3:521. http://dx.doi.org/10.1016/S1470-2045(02)00862-8 [PubMed]
- Carvalho AL1, Singh B, Spiro RH, Kowalski LP, Shah JP. Cancer of the oral cavity: a comparison between institutions in a developing and a developed nation. Head Neck. 2004 Jan;26 (1): 31-8
- Chintamani Tuteja A, Khandelwal R, et al. Patient and provider delays in breast cancer patients attending a tertiary care centre: a prospective study. JRSM Short Rep. 2011; 2:76. http://dx.doi.org/10.1258/shorts.2011.011006. [PMC free article] [PubMed]
- Carvalho AL, Singh B, Spiro RH, Kowalski LP, Shah JP. Cancer of the oral cavity: a comparison between institutions in a developing and a developed nation. Head Neck 2004; 26: 31-8.
- Chuang SC, Jenab M, Heck JE, Bosetti C, Talamini R, Matsuo K, et al. Diet and the risk of head and neck cancer: a pooled analysis in the INHANCE consortium. Cancer Causes Control. 2012; 23(1):69-88. [ Links
- Kumar B, Cordell KG, Lee JS, Worden FP, Prince ME, Tran HH, et al. EGFR, p16, HPV Titer, Bcl-xL and p53, sex, and smoking as indicators of response to therapy and survival in oropharyngeal cancer. J Clin Oncol. 2008; 26 (19):3128-37. [ Links ]
- Marron M, Boffetta P, Zhang ZF, Zaridze D, Wünsch-Filho V, Winn DM, et al. Cessation of alcohol drinking, tobacco smoking and the reversal of head and neck cancer risk. Int J Epidemiol. 2010; 39(1):182-96. [ Links ]
- Znaor A, Brennan P, Gajalakshmi V, Mathew A, Shanta V, Varghese C, et al. Independent and combined effects of tobacco smoking, chewing and alcohol drinking on the risk of oral, pharyngeal and esophageal cancers in Indian men. Int J Cancer. 2003; 105(5): 681-6. [ Links ]
- Gillison ML. Current topics in the epidemiology of oral cavity and oropharyngeal cancers. Head Neck. 2007; 29(8):779-92. [ Links ]
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





