IJCRR - 10(6), March, 2018
Pages: 20-25
Date of Publication: 28-Mar-2018
Print Article
Download XML Download PDF
Pattern of Lower Gastrointestinal Diseases by Colonoscopy and Histopathological Examination:
A Retrospective Study
Author: S. Padma, R. Pramila
Category: Healthcare
Abstract:Colonoscopy is the main investigation to detect the abnormalities in the colon and it is the main supportive measure for clinical diagnosis. Colonoscopic biopsy helps to get a definitive diagnosis of colonic diseases, which helps the clinician to give appropriate treatment.
Aim of the Study: To know the pattern of colonic diseases by colonoscopy and histopathological examination in Chennai Medical College Hospital & Research centre (CMCH&RC) Irungalur Thiruchirapalli District. a tertiary care hospital in rural part of
south India.
Materials and Methods: A retrospective study of patients who had undergone colonoscopy from November 2014 to December 2017 at CMCH&RC was done. Data, from endoscopy register & from histopathology register during that period were collected and analysed.
Results: A total of 919 patients registered for colonoscopy. Male: Female ratio was 614:305.913 patients tolerated the procedure. The most common indications were bleeding per rectum 208 cases (22.78%), clinical suspicion of irritable bowel syndrome 151 cases (16.54%), constipation 115 cases (12.60%), abdominal pain 62 cases (6.79%). The colonscopic findings were, normal study in 47.65%, hemorrhoids in 17.42%, polyps in 8.65%, carcinoma in 6.68%, inflammatory bowel disease in 7.56% of case. About 137 biopsy taken by colonoscopy during this period. The results were malignant lesions in 52, non specific colitis in 27 , benign neoplastic lesions in 14, ulcerative colitis were 13 cases.
Conclusion: The commonest lesion by colonoscopy was hemorrhoids, Histopathological examination supports the colonoscopic study. Commonest lesion by histopathology was malignancy. The increasing incidence of malignancy in younger age group needs further prospective study.
Keywords: Colonoscopy, Histopathology, Carcinoma
DOI: 10.7324/IJCRR.2018.1065
Full Text:
INTRODUCTION
The lower gastrointestinal tract extend from caecum to anal canal which is affected by both neoplastic and non neoplastic diseases. The various diseases affecting the colon are infections, inflammatory diseases, tuberculosis, polyps, colorectal tumours. There may be overlapping of the symptoms in these diseases, which sometimes find difficult to get the final diagnosis clinically1. The colonoscopy helps to locate the exact site of lesion and the type of lesion, Colonic mucosal biopsy by colonoscopy helps to clinch correct diagnosis.
Colonoscopy and colonoscopic biopsy has radically changed the diagnosis and treatment of lower gastrointestinal tract diseases1. Diagnosing a polyp and removal by colonoscopy and histopathological examination has reduced many open surgical procedures2 . In developing countries like India where tuberculosis and infective pathology are common, the incidence inflammatory bowel diseases are showing increasing trend. The histopathological examination of colonic mucosal biopsies by colonoscopy plays an important role in diagnosing inflammatory bowel disease3 as well as early detection of colonic epithelial tumours4.
The aim of our study was to know lower gastrointestinal disease pattern by colonoscopy and also by histopathplogical examination in our area a rural part of south India.
MATERIALS AND METHODS
It is a retrospective study of the available data from colonoscopy procedures performed by the medical gastroenterologist at Medical gastroenterology department at Chennai Medical College Hospital and Research centre (CMCH and RC) Irungalur Thiruchirapalli Dt. a tertiary care hospital in rural part of south India. Data from November 2014 to December 2017 was reviewed. Histopathological reports of the colonoscopic mucosal biopsies done during the period was also reviewed.
Patients with any of these symptoms of (Table.2)
Bleeding per rectum
Clinical suspicion of Irritable Bowel syndrome, carcinoma colon
Constipation
Chronic diarrhea
Abdominal pain
Anemia
Right iliac fossa pain and masswere included. Inpatients from wards as well as outpatients with any of these symptoms were examined by the medical gastroenterologist and colonoscopy was done selectively. Colonoscopy was done after proper bowel preparation. Colonoscopy was done without sedation. Biopsies were taken whenever there was suspicious lesion by colonoscopy. Proper preservation and transferring of biopsy specimen was done as per pathologist guidance. Biopsy specimens were analysed by pathologists and the reports were furnished.
Data analysis includes
All the cases posted for colonoscopy, including the cases where the colonoscopy could not reach the caecum & the data reported in the histopathological examination register.
RESULTS
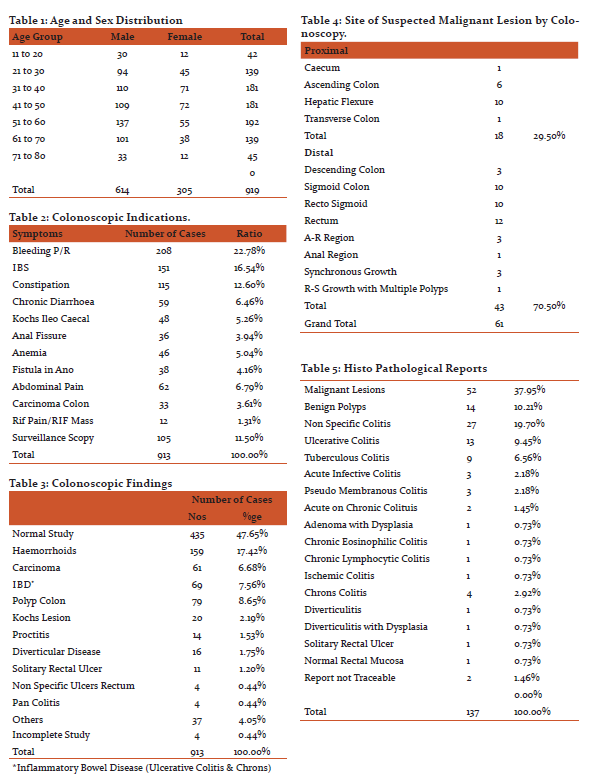
Total of 919 patients were selected for colonoscopy. 913 patients underwent colonoscopy Table.2. The number of males: females were 614:299. The age and sex distribution of cases shown in Table 1.
The common indications were bleeding per rectum 208 cases (22.78%), Irritable bowel syndrome 151 cases (16.54%), constipation 115 cases (12.60%), chronic diarrhea 59 cases (6.46%), ileo caecal kochs 48 cases (5.26%), anal fissure 36 cases (3.94%), anemia 46 cases (5.04%), fistula in ano 38 cases (4.16%), abdominal pain 62 cases (6.79%),carcinoma colon 33 cases (3.61%), right iliac fossa pain and mass 12 cases (1.31%), surveillance scopy (which includes colonoscopy done for inflammatory bowel disease, melena, alcoholic liver disease, hepatomegaly, portal hypertension, multiple gastric polyps etc.) 105 cases (11.50%)( Table.2).
The colonoscopic findings were Normal study in 435 cases (47.65%), Hemorrhoids in 159 cases (17.42%), Carcinoma in 61 cases (6.68%), Inflammatory bowel disease (both ulcerative colitis and chrons disease) in 69 cases (7.56%), Polyp colon in 79 cases (8.65%), Kochs lesion in 20 cases (2.19%), Proctitis in 14 cases (1.53%), Diverticular disease in 16 cases (1.75%), Solitary rectal ulcer in 11 cases (1.20%),Non specific ulcers rectum in 4 cases (0.44%), Pancolitis in 4 cases (0.44%), others (caecal telengectasia, porta hypertensive colopathy, pseudo membranous colitis, extraneous compression etc.) 37cases (4.05%) ,and incomplete study in 4 cases (0.44%) (Table .3).
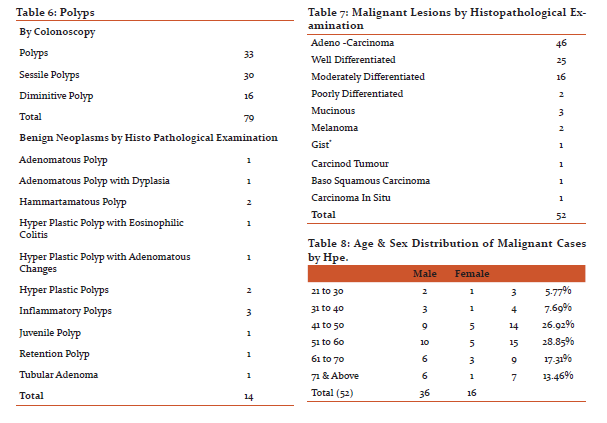
Out of 79 cases of polyps 16 were diminutive polyps, 30 were sessile polyps, 33 were colonic polyps. Polypectomy done in 14 cases.
Colonoscopy showed ulcero proliferative lesion in 41 cases, circumferential lesion in 6 cases, ulcero infiltrative lesion in 3 cases, synchronous lesion in 3 cases, nodulo ulcerative lesion in 2 cases, ulcerative lesion in 2 cases, pigmented lesion in 1 case, polypoid lesion in 1 case, recto sigmoid proliferative lesion with multiple polyps in 1 case, verrucous lesion 1 case. 18 (29.50%) lesions were in proximal colon and 43 (70.50%) lesions were in distal colon.(Table.4)
Total of 137 colonic biopsies taken and was analysed by the pathologist. The malignant lesion reported were in 52 biopsies (37.95%),non specific colitis in 27 (19.70%), benign neoplastic lesions in 14 (10.21%),ulcerative colitis in 13 (9.45%), tuberculous colitis in 9 (6.56%) chrons colitis in 4 (2.92%), acute infective colitis in 3 (2.18%), pseudo membranous colitis in 3 (2.18%), acute on chronic colitis in 2 (1.45%), adenoma with dysplasia in 1 (0.73%), chronic eosinophilic colitis in 1 (0.73%), chronic lymphocytic colitis in 1 (0.73%), ischemic colitis in 1 (0.73%), diverticulitis and diverticulitis with dysplasia each 1 (0.73% each),solitary rectal ulcer 1(0.73%), normal rectal mucosa with surface ulceration in 1(0.73%), reports not traceable in 2.(Table.5).
Of the 137 biopsy specimens 14 were polypectomy specimen, adenomatous polyp in 1specimen,adenomatous polyp with dysplasia in 1 specimen, hyperplastic polyps in 4 specimens , inflammatory polyp in 3 specimens ,hamartomatous polyp in 2 specimens, juvenile polyp in 1 specimen, retention polyp in 1 specimen, 1 polyp was adeno carcinoma.(Table.6)
Of 14 benign neoplastic lesions reported by histopathological examination, 13 specimens were from polypectomy and 1 specimens were mucosal biopsies from colonoscopically suspected malignant lesions where the report was tubular adenoma.
Of the 61 lesions suspected by colonoscopy, histopathological examination showed malignancy in 52 cases (adeno carcinoma in 46, melanoma in 2, gastro intestinal stromal tumour in 1,carcinoid tumour in 1, baso squamous in carcinoma 1,carcinoma in situ in 1 case) (Table.7).5 lesions were benign (1 tubular adenoma, 1adenoma with dysplasia, 2 chrons, 1kochs).4 results not traceable. The age and sex wise distribution of malignancy shown in Table.8.
DISCUSSION
The patients with lower gastrointestinal disease may present with single or combination of symptoms like bleeding per rectum, anemia, abdominal pain, diarrhea, weight loss, constipation, altered bowel habits5. The commonest indication for colonoscopy in our study was bleeding per rectum-22.78% and this was the commonest indication for colonoscopy in the study by H N Dhinesh et al 6(24.8%) and Md Abu Sayeed et al 7(32.53%).
The hemorrhoids (17.42%) was the most common colonoscopic finding in our study and was similar to the study by Raju H. Badiger et al8 (48.4%). In our study the polyps constitute to 8.65% of total cases which was similar to the study by Md Abu Sayeed et al7 who reported as 8.73%.
The colonoscopic suspicion of malignancy in our study was 6.68% which was almost equal to the study by Dhinesh et al6 (7.06%) .The most common location of carcinoma was distal colon 70.50% in our study which was similar to the study by Musthafa et al9 who reported as 74%.The mean age of presentation of malignancy was 69 years in the western population10. Deo et al11 reported mean age at presentation was 45.3 years. In our study the mean age at presentation was 55.13 years.
In our study the out of 135 histopathological reports, non neoplastic lesions were 51.84% and neoplastic lesions were 48.16%, which is similar to the study by Abilash et al1 where the non neoplastic lesion (60.8%) was more than neoplastic lesion.
In non neoplastic lesions non specific colitis constitute to 19.7% in our study which was low compared to the studies by Abilash et al1 Abduikader12 , which was 52.6% and 46.7% respectively. The chronic non specific colitis may represent the early stage of inflammatory diseases like ulcerative colitis and chrons disease.13‚14
Ulcerative colitis was reported in 9.50% of cases in our study, which was less compared to the study by Abduikader12 Saira Bashir et al15 , whose reports were 11.8%, 31.7% respectively.
Tuberculosis was seen in 6.56% of the cases which was slightly high compared to the studies by Ritesh Sulegaon et al16, Pavani Manthini et al17 whose findings were 5.26% and 4.9%.
In our study malignancies were seen in 37.95% (52 cases) of biopsies and 88.46% (46 cases) were adenocarcinomas among them. Out of these adenocarcinomas, 54.34% (25 cases) were well differentiated, 34.78% (16cases)were moderately differentiated, 4.34% (2 cases) were poorly differentiated, 6.52% (3 cases) were mucinous adenocarcinomas. In the study by Chaitanya et al18 the predominant finding was well diffentiated adenocarcinoma 63.16%, moderately differentiated was 13.16%, poorly differentiated was 2.63%, mucinous adenocarcinomas was15.79%. He reported 2.63% as neuro endocrine tumour which was little high compared to our study of 1.92%,
Rectal malignant melanoma account for 0.2% to 0.3% of all malignant melanomas, 0.1 to 4.6% of malignant tumours of rectum and anus19. In our study 2 cases (3.8%)of melanoma rectum reported and it was presented in the age group of 50 to 60. Carcinoma in situ was identified in IBD with pseudopolyps. The GIST & carcinoid tumour was reported in the age group of 21-30. 40.38% of malignant lesions were below 50 years which was high compared to 36% reported by Rajbhandari et al14. Exposure to chemicals used in agriculture for growing rice and soya beans are one of the major environmental carcinogen responsible for colorectal carcinoma among adolescents20. Since our study was retrospective, which lacks the environmental factors, food habits, familial history, it needs further prospective study to find out the increased incidence below 50 and also the causative factors of malignancy.
The incidence of malignancy in sessile polyps and diminutive polyp and polyp less than 1cm is less. Polypectomy was not done routinely in all cases in our study. But follow up colonoscopy could pick up malignant changes if occurs.
CONCLUSION
This retrospective colonoscopic study helped us to know the pattern of lower gastrointestinal diseases in our area. Though the normal study was high, colonoscopy helped to pick up malignant lesions in younger age group. There was good correlation between colonoscopic findings and histopathological findings in malignancy. Histopathological examinations detected benign features in malignant lesion suspected by colonoscopy, thereby helps the clinician to avoid major surgeries. It needs further prospective study to evaluate the factors that causes malignancy in our area.
Acknowledgement:
The Authors acknowledge with thanks the great help rendered by Gasteroenterologist, Pathologist, the Department of Gasteroenterology and the Department of Pathology in CMCH&RC for providing access to the records for analysing the data for this study.
The Authors thank the Officials at CMCH&RC for the encouragement and support provided for bringing out the study which gives an insight into the Lower GI tract disease pattern among the rural population around the Institution.
The Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The Authors are also grateful to Authors/Editors/Publishers of all those articles, Journals and books from where this article has been reviewed and discussed.
ETHICAL CLEARANCE :
Ethical clearance for the use of clinical data and preparation of this Research paper has been obtained from the Management of CMCH&RC , Irungalur. Tiruchirappalli Dt. Tamilnadu.
INFORMED CONSENT :
Not applicable.
SOURCE OF FUNDING:
There is no source of funding for this study.
CONFLICT OF INTEREST:
There is no conflict of interest in the preparation and submission of this Research Paper.
References:
- Abilash S C and Shreelakshmidevi S. Histopathological interpretation of Colonic Mucosal Biopsies with Clinical Correlation : A study in a Tertairy Care Hospital Kerala. Annals of Pathology and Laboratory Medicine, Vol 4, Issues 5, September –Oct 2017: A–567 –A 572.
- Cappel MS, Friedel D. The role of sigmoidoscopy and colonoscopy in the management of lower gastrointestinal disorders, endoscopic findings, therapy, and complications. Medi Clin North Am Nov.86:1253–88
- Greene F L, Livstone EM, Troneale FJ. The role of fibre optic colonoscopy in the diagnosis of colonic and rectal diseases. Comm Med.1973;37: 439–42.
- Siddique I, Mohan K, Hassan F, Patty I, Al Nakib B, Appropriateness of Indication and Diagnostic yield of Colonoscopy First report based on the 2000 guidelines of the American Society of Gastrointestinal Endoscopy .World J. Gastroenterology 2005; 11(44): 7007-13
- Anders Larson, Anders Kilander & Perove Stotzer – Diagnostic yield & Colonoscopiy based on Symptoms. Scandinavian Journal of Gasteroenterology 2008; 43:356-362.
- H N Dhinesh, H B Shashidhar Visnu Prasad . An analysis of Colonoscopy finding in a Tertiary Care Hospital. Int J Sci Stud 2015; 3(7) ; 212 – 216.
- Md Abu Sayeed, Rabiul Islam, Dilruba Siraji, Md Gofranul Hoque ,AQM Mohsen , Colonoscopy : Astudy of findings in 332 patients , JCM CTA 2007; 18(2) 28-31.
- Raju M Badiger , Santosh Hazare, Ravindra Kantamaneni, Ashrey Kole, Deebanshu. Etiological profile of patients presenting with lower gasterointestinal bleeding at Tertiary Care Hospital at Belgavi – A cross sectional study. Int J Adv Med 2017; 41429-33.
- Mustafa Chalikanty Peedikayil Prem Nair , S M Seena, Lakshmi Radhakrishnan, Shine Sadasivan, V A Narayanan ,V Balakrishnan. collororectal Cancer distribution in 220 patients undergoing colonoscopy. Indian J of Gasteroenterol. 2009 ( November-December) : 28(6) :212-215.
- Sailaja Suryadevara, Veerendra Kumar K V, Pampanagouda SKM, Ravi Arjuna , Vijayalaxmi Deshmani. Colorectal cancer profile in tertiary care centre Bangalore India. Online Journal of Health and Allied Sciences. : 1-3
- Deo S V, Shukla NK, Srinivas G, et al. Colorectal cancers-Experience at a regional cancer centre in India. Trop Gasteroentrol 2001:22:83-6
- Abdulkader Mohammed Albarsi. Histopathaological Profile of Benign Colorectal Diseases in Al- Madinah Region of Saudi Arabia. Asian Pacific Journal of Cancer Prevention.VOl 15, 2014 : 7673- 7677.
- Heyman B., Perman JA ,Ferrell LD, Thaler MM, Chronic nonspecific inflammatory bowel disease of the cecum and proximal colon in children with grossly normal appearing colonic mucosa diagnosis by colonoscopic biopsies .Pediatrics 1987 ; 80(2) 255-61.
- Rajbhandari M, Karmacharya A, Khanal K, Dhakal P, Shrestha R.. Histomophological profile of Colospic Biopsies and Pattern of Colorectal Carcinoma in Kavre District. Kathmandu Univ Med J 2013;43(3): 196-200.
- Saira Bashir, Rabia Nadeen, Nauman Khan, Bilquis A. Suleman, Ghulam Rasia Qureshi. Histopathological Analysis of 1000 Colorectal Biopsies in Two years in Shaikh Zayed Hospital. Lahore. P J M H S VOL 6 NO 1 JAN –MAR 2012 :115-117.
- Ritesh Sulegaon, Smita Shete, Dinesh Kulkarni. Histological Spectrum of Large Intestinal Lesions with Clinicopathological Correlation. Journal of Clinical and Diagnostic Research , 2015 Nov,VOl-9;(11)EC30-EC34.
- Pavani Manthini, Raghu Kalahasthi, Srikanthbabu Yariagadda ,K P A Chandrasekhar, S Parimala Devi, Aravida Basa, Manohara Vaddadi, Pramod Kumar Reddy Malyala. Histopathological study of lesions of colon- a 5 year study International Journal of Scientific Study ,May 2017,Vol 5 ,Issue 2 : 65-68.
- Chaitanya B, Ramakrishna BA, Shanthi V, Reddy SR. Microscopy after Colonoscopy an institutional experience in India. International Journal of Medical Research and Review. March-April, 2004/Vol2/Issue 2 : 92-97.
- Burcak Kaughan, Nesrin Turan,Ersan Ozasten Meral Akdogan, A rare entity in the rectum malignant melanoma. Turk. J. Gastroenterol 2003;14(4) : 273-275
- Pratt CB, Rivera G, Shanks E. Colorectal Carcinoma in adolescents complications regarding etiology. Cancer 1977; 40: 2464-72
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





