IJCRR - 10(6), March, 2018
Pages: 10-13
Date of Publication: 28-Mar-2018
Print Article
Download XML Download PDF
Coronary Artery Status in Young Age Group in Autopsy Study
Author: Nidhi Dhingani, Bhavika Vaghela, Hansa Goswami
Category: Healthcare
Abstract:Introduction: The coronary atherosclerosis is one of the common diseases in elders. Now it is growing fast among young age group in developing countries. The purpose of this study is to analyze the changing epidemiological trends and prognosis of CAD in young population.
Material and Method: This study was conducted from January 2016 to June 2017 at Department of Pathology, B.J. Medical College, Ahmedabad, Gujarat. This is a retrospective study. Data taken from autopsy section, B.J. Medical college, Ahmedabad.
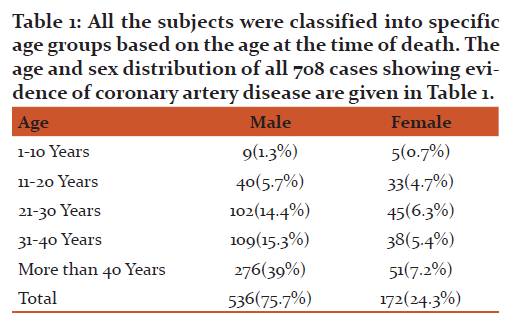
Result: A total of 708 autopsy cases were studied. In the study 536 (75.7%) were males and 172 (24.3%) were females. Among them 260(48.5%) males and 128(74.5%) females below 40 years of age had coronary artery lesions. Most commonly involved coronary artery was Left coronary artery.
Conclusion: The study showed alarmingly high prevalence of Atherosclerosis in young age. So screening for the same should begin at an early age. The incidence of atherosclerosis is more common in males compared to females; though coronary atherosclerosis is an important risk factor for IHDs in both sex.
Keywords: Atherosclerosis, Younger age, Coronary vessels, Autopsy
DOI: 10.7324/IJCRR.2018.1063
Full Text:
Text:
Introduction:
Coronary artery disease occurring below the age of 45 years is termed as young coronary artery disease (CAD)[1]. Atherosclerosis is a chronic degenerative condition of arteries responsible for significant cardiovascular morbidity and mortality worldwide. In the Indian subcontinent‚ it is reported to be responsible for more than 25% of deaths [2‚3]. The prevalence of coronary artery disease (CAD) among Asian Indians is higher than among Europeans, Americans and other Asians [4‚5]. Many studies showed that the case load of CAD in India is alarming. According to the World Health Report 2002‚ 45 million people in India are suffering from CAD and it is contributing to one fifth of the deaths in India and also‚ by the year 2020, CAD will account for one third of all deaths. The same report estimated that heart disease in Indian population occurs 10 to 15 years earlier than in the western population [6]. Atherosclerotic lesions start developing at an earlier age and are found to be in more advanced stage in Indian population as compared to the population in western countries. Atherosclerosis can lead to various complications like myocardial infarction (MI)‚ stroke‚ embolization‚ ulceration‚ thrombosis,aneurysm which cause considerable morbidity and mortality‚ thus affecting the life span and the quality of life of a large segment of population.
Material and method:
This study was conducted from January 2016 to June 2017 at Department of Pathology‚ B.J. Medical College‚ Ahmedabad‚ Gujarat. The deceased patients who underwent autopsy at the hospital and their past medical history were recorded and their hearts were sent to our department for histopathological analysis. The Hearts were grouped according to age and sex. The specimen were fixed in 10% formalin solution for 2-5 days. The coronary arteries dissected and examined grossly for other anomalies. Identified segments of coronary arteries viz. left and right coronary artery were sectioned at 3 mm interval and histopathological slides were made. All the histological sections were examined microscopically for the presence of atheroma and MI. Grading of atherosclerotic plaque according to American Heart Association was done below.
Grade 0
Sections showing normal histology or adaptive thickening without macrophages or foam cells.
Grade 1
Presence of isolated macrophages and foam cells.
Grade 2
Mainly intracellular lipid accumulation.
Grade 3
Grade 2 lesions along with small extracellular lipid pools.
Grade 4
Grade 2 changes along with a core of extracellular lipid.
Grade 5
Lipid core and fibrotic layer or multiple lipid cores and fibrotic lipid layers; mainly calcific or fibrotic.
Grade 6
Surface defect‚ hematoma‚ hemorrhages or thrombus formation.
The degree of atherosclerosis was classified as :
unremarkable (Grade 0)‚
mild (Grade 1-2)‚
moderate (Grade 3-4)‚
severe (Grade 5-6).
Result:
Discussion:
Morbidity and mortality due to coronary atherosclerosis in India has reached alarming proportions and these numbers are expected to maintain the upward trend in the next decade. Atherosclerosis is a commonly observed pathological finding in almost all ethnicities and societies worldwide‚ but with variable prevalence in different races. The onset of atherosclerosis starts early in life from childhood and gradually progresses through young adulthood to form the lesion that causes coronary heart disease. In the present study, the overall incidence of atherosclerosis was found to be 82.34%‚ which is higher than what has been founded in earlier studies by Dhruva et al.‚ (23.3%) [7]; Golshahi et al.‚(28.9%)[8]; Garg et al., (46.4%)[9] and Yazdi et al.,(40%)[10]. Ischemic heart disease (IHD) due to coronary vascular lesion is mainly caused by atherosclerosis. The Indian population is vulnerable to coronary vascular disease and the disease also has an earlier onset in our population. In our study we found that there is a progressive steady increase in atherosclerosis in coronary vessels in early age group. So screening for cardiovascular Risk factor should be start from younger age group.
Lack of exercise and poor dietary habits like intake of junk food and increased use of refined and processed food items in place of whole grains and fresh fruits and vegetables can be important risk factors for earlier initiation of development and progressive increase in atherosclerotic lesions in this young Indian population. Males have a relative preponderance for coronary heart disease as is evident from multitude of national and international studies conducted in the past.
In the study conducted by Garg et al.,[9]; they found coronary atherosclerotic lesions in 80.9%(93)males as compared to 19.1%(22) females. Bhargava and Bhargava[11] reported coronary atherosclerotic lesions were more prevalent in 74.8% males in comparison to 24.2% females in their study. Murthy et al.‚[12]‚ studied 150 cases of coronary atherosclerotic lesions, out of which 123(80%) were males and 27(18%) were females. Singh et al., [14] also reported coronary atherosclerotic lesions in 200 cases and found that these lesions were more frequently found in males(85%) as compared to females(15%). Padmavati and Sandhu [15%]found that 66.5% males and 33.5% females were affected by coronary atherosclerotic lesions. In the present study too, we found a male (75.7%) preponderance for coronary atherosclerosis as compared to females(24.3%). The findings of our study corroborates well with the findings of previous studies. There may be a protective role of female hormones like estrogen against atherosclerosis. Moreover, there is greater indulgence of males in smoking and alcoholism as compared to females, which may possibly explain the male preponderance towards development of more severe and progressive atherosclerosis.
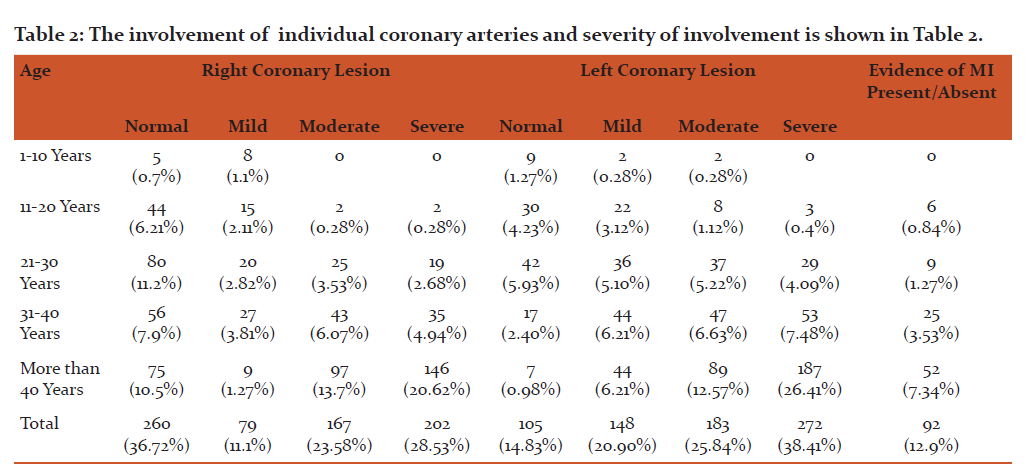
Incidence of Left coronary artery involvement was 85%, Right coronary artery involvement was 63%. This was in concordance with Data given by sudha et al., [15] and Yazdi et al.,[10], left coronary artery is more commonly involved than right coronary artery.
In left coronary artery, left anterior descending artery is the commonest artery to be involved.
Acute MI was seen in 13% cases compared to observations of 9.72, 6.5 and 3% acute MI cases observed by Dhruva et al.,[7] Maru [16], garg et al.,[9] respectively. The percentage of MI is slightly higher than previous study. Incidence of MI attack alarmingly increasing in younger age group.
Conclusion:
The study showed unexpectedly high prevalence of coronary artery lesion ahmedabad in India. Though the incidence of atherosclerosis is more in males as compare to females, but there is a progressive increase in the proportion of females who present with coronary atherosclerosis. This study highlights the importance of cardiovascular risk factors screening for early ages. The study of human atherosclerotic lesion is an extremely difficult task in a living subjects and autopsy study is the best possible way to work on it. Though our study involved only small numbers of cases, it highlights the early onset and increasing prevalence and severity of atherosclerotic lesions in Indian populations.
References:
1. Egred M, Viswanathan G, Davis GK. Myocardial infarction in young adults. Postgrad Med J 2005; 81: 741-745 [PMID: 16344295 DOI: 10.1136/pgmj.2004.027532]
2.Indrayam A. Forecasting vascular disease and associated mortality in india. NCMH Background papers: Burden of disease in India. National Commission on macroeconomics and Health , Government of india 2005:197-215
3.Gupta R, Joshi P, Mohan V, Reddy KS, Yusuf S. Epidemiology and Causation of coronary heart disease and stroke in India. Heart 2008:16-26 (pubmed)
4. Reddy KS. India wakes upto the threat of cardiovascular disease. [1] J Am Coll Cardiol. 2007;50:1370-72.
5.Gupta R. Recent trends in Coronary heart disease epidemiology in India. Indian Heart J. 2008;60(2suppl-B):B4-18.
6. Alarming Statistics from India. [Internet] 2015 [Cited 2015 FEB 19]. Available from http://neocardiabcare.com/alarming-statistics-india.htm.
7.Dhruva GA, Agravat AH, Sanghvi HK. Atherosclerosis of coronary arteries as predisposing factor in myocardial infarction: An autopsy study.(Last assessed on 2013 Dec 13);Online J Health Allied Sac.2012 11:1.Available From: http://www.ojhas.org/issue43/2012-3-1.htm
8.Golshahi J, Rojabi P, Golshahi F. Frequency of atherosclerotic lesions in coronary arteries of autopsy specimens in Isfahan forensic medicine centre. J Res Med.2005;1:16-9.
9.Garg M, Agraval AD, Kataria SP. Coronary atherosclerosis and myocardial infarction: An autopsy study. J Indian Acad Forensic Med.2011 33:39-42. Available from:http://medind.nic.in/jal/t11/il/jalt11ilp39.pdf.
10.Yazdi SA, Razaei A Azari JB, Hezari A, Shakeri MT, Shahri MK. Prevalence of atherosclerotic plaques in autopsy cases with noncardiac death. Iran J pathol. 2009;4:101-4
11.Bhargava MK, Bhargava SK. Coronary atherosclerosis in North Karnataka. Indian J. pathol Microbiol.1975;18:65-79.(pubMed)
12.Murthy MS, Dutta BN, Ramalingaswami V. Coronary atherosclerosis in North india(Delhi india)J pat hol Bacteriol.1963;85:93-101 (pubMed)
13.Padmavati S, Sandhu I. Incidence of coronary artery disease in Delhi from medico-legal autopsies. Indian J Med Res.1969;57:465-76 (pubMed)
14.Singh H, Oberoi SS, Gorea RK, Bal MS. Atherosclerosis in coronaries in malwa region of Punjab. J Indian Acad Forensic Med.2005;27:32-5s
15.Sudha ML. Sundaram S, Purushotaman KR,K Kumar PS, Prathiba D. Coronary atherosclerosis in sudden cardiac death :An autopsy study. Indian J Pathol Microbiol.2009:52:486-9. (pubMed)
16.Maru M. Coronay atheraosclerosis and myocardial infarction in autopsied patients in Gondar. Ethiopia. JR soc Med.1989;82:399-401.(PMC free article)(PubMed)
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





