IJCRR - 10(5), March, 2018
Pages: 01-06
Date of Publication: 15-Mar-2018
Print Article
Download XML Download PDF
Interval Appendectomy vs Conservative Management Alone - A Therapeutic Dilemma - A Retrospective Comparative study at Chennai Medical College Hospital and Research Centre - Irungalur, a Rural Tertiary Care Centre in South India
Author: R. Murugan, S. Padma, M. Senthilkumaran
Category: Healthcare
Abstract:Background: Acute appendicitis is the most common cause of \"acute abdomen.\" In the 2 to 6 % of cases if not treated early it may develop in to an appendiceal mass. Conventionally conservative treatment followed by interval appendectomy is so far followed. Recent studies discourage the role of interval appendectomy. Hence our study is focused on the pros and cons of interval appendectomy.
Methods: One hundred and fifty patients with the clinical diagnosis of appendicular mass admitted in our hospital from Jan. 2013 to Dec. 2016 - 4years are divided in to two groups I and II. The group I treated with conservative management followed by interval appendectomy. The group II was treated with conservative management alone with continued follow up. In each the age and sex incidence, rate of the recurrence, complications are studied, statically analysed and interpreted.
Results: The age and sex distribution in both groups 1 and 2 showed no much deviation. . In the group I recurrence was observed in 13 (17.3%) and in group II 10 patients (13.3%) that means the rest of (83.7%) and (86.7%) does not need any surgical intervention. Major complications like adhesive obstruction (4%), incisional hernia (1.3%), enterocutaneus fistula (2.6%) and sepsis(6.6%)were observed in interval appendectomy group showing the more morbidities following interval appendectomy. Other pathologies like carcinoma caecum (1.3%), mucocele of appendix (1.3%) and chron's disease (1.%) were also encountered.
Conclusion: In our study for appendiceal mass management, conservative management with interval appendectomy showed the incidence of appreciable major complication and the incidence of recurrence is low. In conservative management alone with continued follow up the incidence of recurrence is less and the complications are not much. Hence we conclude that the conservative management with continued follow up is the management of choice.
Keywords: Enterocutaneous fistula, Interval appendectomy, Mucocele of appendix, Phlegmon
DOI: 10.7324/IJCRR.2018.1051
Full Text:
INTRODUCTION
Acute appendicitis is the most common surgical emergency which may be complicated by development of an appendiceal mass. The appendiceal mass is formed around the perforated appendix and it consists of an inflammatory mass of the inflamed appendix, adjacent viscera and the greater omentum [1].
An appendiceal mass varies from phlegmon to abscess [2,3] and it develops in 2% to 6% of cases following acute appendicitis [4]. Appendiceal mass is more commonly seen in elderly males [5]. For decades there have been conflicting opinions in the appendiceal mass management. Three modes of management practised now are (1) immediate appendectomy before the resolution of the mass [6, 7, 8], (2) conservative management with interval appendectomy in 6to 8 weeks [9, 10, 11]. (3) An entirely conservative approach without interval appendectomy with regular follow up [12,13,14,15]. Conservative management for appendicular mass initially as described by Oshner [16] has so far been followed routinely by surgeons worldwide. Oschner-Sherren regime includes hospitalisation, bowel rest, broad spectrum antibiotics, hydration and percutaneous drainage of abscess until the mass gets resolved.
Traditionally following conservative management of appendicular mass interval appendectomy (6-8weeks later) is done. Surgeons suggesting interval appendicectomy claim that recurrence of appendicitis is more common and by doing interval appendicectomy the underlying pathology like chron’s disease, mucocele or malignancy can be dealt with in time [3, 13, 17, 18, 20, and 21].
The need for interval appendicectomy after successful conservative treatment has recently been questioned and increasing number of studies on this aspect are pouring in. [22, 23, 24]. The advocates of conservative management alone with prolonged follow up without interval appendectomy, substantiate that the rate of recurrent appendicitis is low (6-20%) and point out that even the potential recurrences have mild clinical course. More over complications include wound and intra-abdominal sepsis, adhesive small bowel obstruction [25].
Immediate appendectomy following resolution of mass may look like easily feasible, safe, cost effective allowing early diagnosis and treatment of unexpected pathology. However it has higher complication rate 36% leading to dissemination of infection, intestinal fistula formation with misdiagnosed of cancer may end up in right hemicolectomy. Sometimes a malignant mass may be mistakenly under treated by appendectomy[26,27]. Because of these complication this method is not practiced nowadays unless there is no response to conservative treatment [28, 29].
Hence we have restricted our study in the management of appendiceal mass to retrospective comparative study on conservative management followed by interval appendectomy against conservative management alone with regular follow up.
MATERIALS AND METHODS
Study settings:
Patient who were admitted in Chennai medical college hospital and research centre Tiruchirappalli a rural tertiary medical care centre were taken up for study.
Design of study:
Retrospective study was conducted in patients admitted in general surgery department Chennai medical college hospital and research centre. The detailed particulars recorded included date of admission, demographics, clinical history, investigation, type of treatment and date of discharge in addition their follow up records with regard to recurrence, and complication during their subsequent visit or through telephonic communication.
Period of study:
Patient admitted to hospital for appendiceal mass from January 2013 to December 2016. Follow up made for minimum 1 year after their discharge.
Sample size:
Hundred and fifty patients admitted with appendiceal mass were selected for the study. Among them one group of 75 patient ( group I ) treated with conservative management followed by interval appendectomy in 6 to 8 weeks time and another group of 75 patients (group II ) were treated with conservative management alone with regular follow up for minimum one year.
Ethics:
The study was preceded after getting approval from institutional ethical committee of CMCH&RC.
Informed consent was obtained from patient or their relatives
Inclusion criteria:
- All patients with clinical findings and investigation report in favour of appendiceal mass were included
- All age group from 10 to 80 years
- Both male and female patient were included
Exclusion criteria:
- Patients with generalised peritonitis were excluded.
- Patients with other comorbid condition like severe cardiac illness, chronic respiratory diseases, chronic renal failure, and bleeding disorder were excluded.
- Non cooperative patients for regular follow up.
Data collection techniques: The patients history clinical findings, investigation reports, mode of management, operative findings, prognosis and follow up details are collected and recorded in Performa prepared.
METHODS
A retrospective study was performed on all the 150 patients admitted with clinical diagnosis of appendicular mass. For all patients the following investigations were done:
- Urineroutine 2. Complete blood count 3. Blood sugar/urea/creatinine 4. Serum electrolytes
- .X-ray chest / Eletro cardio gram 6 .Ultrasound Abdomen 7.Computed tomography(CT) Abdomen
Initially all were treated conservatively as described by Oshner& Sherren .
After successful management of appendiceal mass patients, group I were advised tocome for interval appendectomy in 6 to 8 weeks. On their readmission they were performed appendectomy either by open or laparoscopic procedure. All were followed up for minimum one year for any complication and to assess prognosis.
In group II patients were advised to come periodically for review or as soon as any recurrence of symptoms appear. Patients with recurrence were admitted and appendectomy done either by open or laparoscopic procedure. Patients who did not turn up for review were closely followed up by telephonic conversation and their complaints if any present were recorded. They were followed up for one to two years. Patients in this group who were anaemic and more than forty years of age were performed contrast enhanced computed tomography(CECT) abdomen, colonoscopy to rule out any other pathology like Cancer caecum, chrons disease.
RESULTS
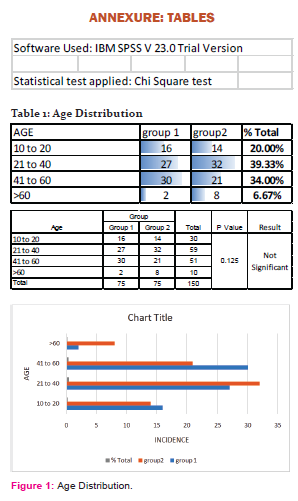
Outcome of our study are shown in the tables attached. The age and sex distribution in each group are as follows.
With regard to age in groupI the patients at the age of 10 to 20 years were 16 (21.3%) ,21 to 40 yrs 27 (36%), 41 to 60 yrs 30 (40%),and >60 yrs 2 (1.3%). In group II 10 to 20 yrs 14 (18.6%), 21 to 40 yrs 32 (42.6%), 41 to 60 yrs 21(28%), and >60 yrs 8 (10.6%) Table1.
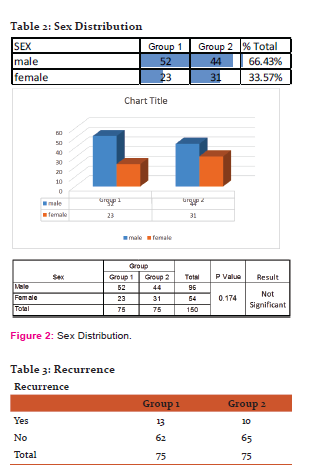
In group I male were 52 (69.3%) and female 23 (30.6%). In group II male were 44 (58.6%) and female 31 (41.3%) Table 2.
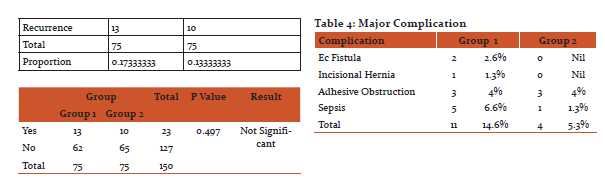
The incidence of recurrence in group I based on HPE report was seen in 13 patients (17.3%). In groupII3 (4%) patients came with recurrent appendicitis in 3 months, 5 (6.6%) in 6 months and 2 (2.6%)in 1year. Table3.
With regard to complications in groupI our study reveals that in group I the incidence of complications include sepsis 5 (6.6%),. enterocutaneous fistula 2 (2.6%), incisional hernia 1 (1.3%) and adhesive obstruction 3 (4%). In group II the main complication like bowel obstruction in 3 patients (4%) and intra abdominal sepsis 1 (1.3%) are encountered. Table 4.
Occasional missed pathological conditions seen were Ca. Caecum 1 (1.3%), mucocele of appendix2 (2.6%) and Chron’s disease 2 (2.6%) mostly in group I patients.
DISCUSSION
Early appendectomy is the treatment of choice in acute appendicitis. Once mass has formed the line of management is controversial subject. Current study mostly favours conservative management for appendiceal mass16]. Following conservative management to go for interval appendectomy in 6 to 8 wks period or conservative management alone with regular follow up is still a debatable question.
Following conservative management the intension for doing interval appendectomy is mainly to avoid recurrence. The prospective study done by Youssuf et. al. revealed that interval appendectomy done at 6 and 12 weeks had prevented 10.6% and 6.7% of recurrent appendicitis respectively. [30,31] that means that in 89.4% and 93.3% the interval appendectomy done was unnecessary. In literature the reported rate of recurrence after conservative management alone was 6.2% which was more common during the first six months. The one year recurrence rate was low. (1.9—2.2%) [24,32]. In another random perspective study conducted by Kumar and Jain the recurrence was only 10% where conservative management with regular follow up alone was done [30].
In our study out of the 75 patients in the group I only 13 patients had evidence of recurrent appendicitis on HPE (17.3%) that means rest of the 62 patients (82.7%) has not developed recurrent appendicitis. In the group II out of 75 patients 3 patients came with recurrent appendicitis in 3 months (4%) , 5 patients in 6 months (6.6%) and 2 patients in 1 year (2.6%). that means only 10 patients (13.3%) totally in 1 year period. It shows that the rest of the 65 patients (86.7%) has not developed recurrence. Based on these observations doing routine interval appendectomy is not mandatory to prevent recurrent appendicitis since the results clearly show the recurrence rate is considerably less to go for interval appendectomy straightaway. Moreover recurrence after conservative management has mild clinical course and surgical treatment has little complications.
Another important point to study is the complications related to conservative management with interval appendectomy and conservative management only with regular follow up. In a series of studies the complications following interval appendectomy was 12% to 23% [11,14, 27 ,31 ] which included sepsis, bowel perforation, ileus, fistulas and adhesive obstruction [32] . The relative occurrence was equal to the complications occurring while doing immediate appendectomy for appendiceal mass[4]
Our study reveals that in groupI the incidence of complications include sepsis in 5 patients (6.6%), enterocutaneous fistula 2 (2.6%), incisional hernia1 (1.3%) and adhesive obstruction 3 (4%). In group II the main complication like bowel obstruction in 3 patients (4%) and intra abdominal sepsis 1 (1.3%) are encountered. It clearly shows since the morbidity is more (14.6%) after interval appendectomy it is better to go for conservative management with regular follow up and plan for surgery if recurrence occurs.
In addition , review of literature exposes the occasional findings of missed pathological conditions like Meckel’s diverticulitis, Chron’s disease, malignancy and mucocele of appendix [33,34,35] .In our study we encountered different pathologies like Ca. Caecum (1), mococele of appendix (2) and Chron’s disease (2).
CONCLUSION
Recent studies in literature are mostly not in favour of routine interval appendectomy following conservative management of appendiceal mass. Based on the results of our study recurrence rate in both interval appendicectomy group and conservative management alone group are comparatively less and the complication rate more in the interval appendicectomy group , we conclude it is better to go for conservative management with regular follow up and intervene only when recurrence occur in case of appendiceal mass.
LIMITATIONS
- Single centre study may not reflect the general population
- Small sample size
- Several surgeons with varying experience were involved in the management.
Acknowledgement:
The Authors acknowledge with thanks the great help rendered by DEAN and the Department of GENERAL SURGERY in CMCH & RC for providing access to the records for analysing the data for this study.
The Authors thank the colleagues at CMCH&RC for the encouragement and support provided for bringing out the study in a fruitful manner.
The Authors are grateful to the Authors, Editors and Publishers of all those articles and Journals from where the literature for this article has been reviewed and discussed.
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding – NIL
Conflict of interest - NI
References:
- Willemsen PJ, Hoorntje LE, Eddes EH, Ploeg RJ. The need for interval appendectomy after resolution of an appendiceal mass questioned. Dig Surg. 2002; 19: 216–220; discussion 221. [PubMed]
- Arnbjornsson E. Management of appendiceal abscess. Curr Surg. 1984; 41: 4–9. [PubMed]
- Nitecki S, Assalia A, Schein M. Contemporary management of the appendiceal mass. Br J Surg. 1993; 80: 18–20. [PubMed]
- Bagi P, Dueholm S. Nonoperative management of the ultrasonically evaluated appendiceal mass.Surgery. 1987;101:602-605.
- Norman S William, Christopher JK et.al Vermiform Appendix in short practice of Surgery 25th Ed. London. Edward Arnold publisher Ltd. 2008 1205-1217
- Vakili C. Operative treatment of appendix mass. Am J Surg. 1976; 131: 312–4. [PubMed
- Marya SK, Garg P, Singh M, Gupta AK, Singh Y. Is a long delay necessary before appendectomy after appendiceal mass formation ? A preliminary report. Can J Surg. 1993; 36:268–70. [PubMed]
- De U, Ghosh S. Acute appendectomy for appendicular mass: A study of 87 patients. Ceylon Med J. 2002;47:117–8. [PubMed]
- Ranson JH. Nonoperative treatment of the appendiceal mass: Progress of regression? Gastroenterology. 1987; 93: 1439–45.
- 8. Friedell ML, Perez-Izquierdo M. Is there a role for interval appendectomy in the management of acute appendicitis? Am Surg. 2000; 66: 1158–1162. [PubMed]
- . Skoubo-Kristensen E, Hvid I. The appendix mass: Result of conservative management. Ann Surg. 1982; 196: 584–7. [PMC free article][PubMed]
- Hoffmann J, Lindhard A, Jensen HE. Appendix mass: Conservative management without interval appendectomy. Am J Surg. 1984; 148: 379–82. [PubMed]
- Adalla SA. Appendiceal mass: Interval appendicectomy should not be the rule. Br J Clin Pract. 1996; 50:168–9. [PubMed]
- Verwaal VJ, Wobbes T, Goris RJ. Is there still a place for interval appendectomy? Disgestive Surgery. 1993; 10: 285–8.
- Benjamin Quartey; J. Emer. Trauma Shock 2012: July- Sep 5(3) 213-216
- Ochsner AJ. The cause of diffuse peritonitis complicating appendicitis and its prevention. JAMA. 1901;26:1747–54
- 23. Paul DL, Bloom GP. Appendiceal abscess. Arch Surg. 1982; 117: 1017–9.
- . Lai HW, Loong CC, Chiu JH, Chau GY, Wu CW, Lui WY. Interval appendectomy after conservative treatment of appendiceal mass. World J Surg. 2006; 30: 352–7. [PubMed]
- Abdul Wahed Nasir Meshikhes Appendiceal mass: Is interval appendicectomy “something of the past” World J Gastroenterol 2011July 7; 17(25):2977-2980
- Ahmed I, Deakin D, Parsons SL. Appendix mass: Do we know how to treat it? Ann R Coll Surg Engl. 2005; 87: 191–5. [PMC free article][PubMed]
- Lane JS, Schmit PJ, Chandler CF, Bennion RS, Thompson JE. Ileocecectomy is definitive treatment for advanced appendicitis. Am Surg 2001; 67: 1117-1122
- Brown CV, Abrishami M, Muller M, Velmahos GC. Appendiceal abscess: immediate operation or percutaneous drainage?Am Surg 2003; 69: 829-832
- Tekin A, Kurto?lu HC, Can I, Oztan S. Routine interval appendectomy is unnecessary after conservative treatment of appendiceal mass. Colorectal Dis 2008; 10: 465-468
- Luckmann R. Incidence and case fatality rates for acute appendicitis in California. A population -based study of the effects of age. Am J Epidemiol 1989; 129: 905- 918
- Oliak D, Yamini D et.al Nonoperative management of perforated appendicitis with appendicular mass Am. J.Surg. 2000; 179: 171-181
- Mesike AW. Management of appendicular mass- controversial issues revisited ; J Gastrointest. Surg: 2007 Nov 13
- Mosegaard A, Nielsen OS. Interval appendectomy. A retrospective study. Acta Chir Scand. 1979;145(2):109–111. [PubMed]
- Foran B, Berne TV, Rosoff .L Management of appendiceal mass. Arch. Surg.1978 ; 1144-1145 [Pub.Med]
- Engkvist O. Appendectomy à froid a superfluous routine operation? Acta Chir Scand. 1971;137(8):797–800. [PubMed]
- Kumar S, Jain S. Treatment of appendiceal mass: prospective, randomized clinical trial. Indian J Gastroenterol. 2004;23:165–167. [PubMed]
- Youssef T, Badrawy A. Prospective evaluation of the necessity of interval appendectomy after resolution of appendiceal mass. Egyptian J Sur. 2010;29:85–9.
- Eriksson S, Styrud J. Interval appendectomy: a retrospective study. Eur J Surg. 1998;164:771–774; discussion 775.
- Anderson RE Small bowel obstruction after appendectomy; Br.J.Surg.2001;88: 1387-1391
- Mizziotti MV, Marley EF et. al. Histopathologic analysis of interval appendectomy specimen : Support for the role of appendectomy J. Paed. Surg 1997; 32: 806-809
- Price MR, Hase GM., et. al. Reccurent appendicitis after initial conservative management of appendiceal abscess J. Paed. Surg ; 1996 : 31 ; 291-294
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





