IJCRR - 10(4), February, 2018
Pages: 09-11
Date of Publication: 17-Feb-2018
Print Article
Download XML Download PDF
Cryptosporidiosis in a Child with Acquired Immunodeficiency Syndrome: A Case Report
Author: Nanthini Devi P., Gomathi S.
Category: Healthcare
Abstract:Cryptosporidiosis is caused by the coccidian parasite Cryptosporidium and has a tendency to cause diarrhoea with dehydration in immunocompetent and immunocompromised individuals. Here we describe the clinical course of a 4 year old male child who was HIV(Human immunodeficiency virus) reactive and improvement was seen after a course of Nitazoxanide.
Keywords: Cryptosporidium, Diarrhoea, Acquired immunodeficiency syndrome
DOI: 10.7324/IJCRR.2018.1042
Full Text:
Introduction
Cryptosporidiosis is an infection with the coccidian parasite Cryptosporidium and is a significant opportunistic disease among HIV-infected individuals and [1]. In developing countries like India, 2-19% of diarrheal diseases can be attributed to Cryptosporidium. It is spread through the fecal-oral route, often through contaminated water [2]. The age group most commonly affected is children from 1 to 9 years old [3]. Cryptosporidium causes prolonged diarrhoea in HIV patients regardless of the age group [4]. Here we present a case of chronic diarrhoea in a four year old male child with Acquired Immune Deficiency Syndrome (AIDS) and mile stone delay.
Case history:
A 4 year old known HIV positive boy with milestone delay had diarrhoea and vomiting for one week. He experienced ten episodes of watery, non-bloody diarrhoea per day. He had similar illness in the past but stool examination was not done. His parents were also HIV positive. The child was on Anti-retroviral therapy (ART) but on irregular treatment.
His vital signs showed blood pressure to be 86/54 mm Hg, pulse rate of 120 beats per minute and respiratory rate of 16 per minute. The laboratory investigations revealed Serum sodium-130 mmol/L), Serum potassium-4.5mEq/L,Chloride-111mEq/L,Bicarbonate-13 mmol/L, Serum calcium-8.4 mg/dl, Blood glucose-98 mg/dl. The total count was 20800 cells/mm3(56% neutrophils, 36% lymphocytes, 7%monocytes, 1% eosinophil, 1% basophil). The hemoglobin level was 8.2 g/dL, platelets 468,000/mm3 and red blood cell count-4.1 million /mm3. The urine routine examination showed no albumin, no sugar and 1-2 pus cells per high power field. There was no growth in blood and urine culture.
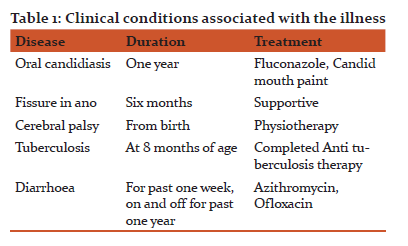
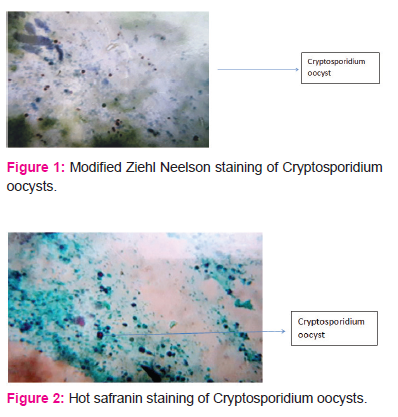
The stool wet mount examination showed numerous spherical and refractile oocysts about 5 micrometer diameter. Modified Acid fast bacilli staining showed pink coloured oocysts of Cryptosporidium with distinct oocyst walls. Giemsa staining revealed the presence of purple coloured oocysts. Hot safranin staining showed pink coloured oocysts.
The child was treated with intravenous fluids, zinc supplements and a course of Nitazoxanide. The stool episodes reduced after treatment. The parents were advised to continue ART to the child for immune reconstitution. Health education was provided to the parents regarding hygienic practices and importance of regular ART.
Discussion:
Cryptosporidiosis is caused by the enteric pathogen Cryptosporidium, a genus of protozoan parasites in the phylum Apicomplexa [5]. There are more than 26 known Cryptosporidium species which can be differentiated by morphology, host specificity and molecular biology studies [6]. The majority of human cryptosporidiosis worldwide are mainly caused by two species C. parvum and C. hominis.[7].Cryptosporidium spp. is increasingly being recognized as an important pathogen causing diarrhea in children nowadays, with the highest morbidity and mortality reported in children less than 5 years in developing countries [8].It can affect both immunocompetent and immunocompromised individuals, resulting in watery diarrhea and extreme dehydration [9]. Cryptosporidiosis is a potential threat to HIV-infected individuals with a risk of infection of around 10% in developed countries. Patients can have chronic watery diarrhea lasting for more than two months and shed oocysts in stool during the entire period [10,11]. Early childhood infection with Cryptosporidium can result in delayed growth and cognitive decline[12]. Cryptosporidium was first recognized as a human parasite in 1976, in a three year-old child with enterocolitis. But it became recognized as an important human pathogen after the HIV pandemic in the 1980s [13]. The first case of cryptosporidiosis in a homosexual man with AIDS was reported back in 1982 [14]. Since then, there have been many reports of Cryptosporidium as an important pathogen in AIDS. Currently, Cryptosporidios is listed as an AIDS-defining illness (Clinical Category C) by the Centers for Disease Control and Prevention [15]. The infection in HIV infected individuals is life- threatening and involves infections of the gastrointestinal tract in addition to hepatobiliary and respiratory tract infections [16,17].
Conclusion:
This case is important because it highlights the mother to child transmission of HIV. In pediatric populations, prevalence data are still underestimated, due to the absence of advanced laboratory diagnostic tools. In the poorest areas, Cyptosporidiosis, enhanced by malnutrition, causes growth failure and further immune derangement, leading to wasting and enhancing children mortality.
With the widespread use of ART, Cryptosporidiosis is no longer the dangerous condition it once was in AIDS patients, it continues to be a dangerous threat to AIDS patients in developing countries where ART is not available. The case report shows that health education should be provided to HIV positive parents regarding antenatal screening, regular ART, hygienic practices to cut down the prevalence of HIV and HIV related diseases.
Abbreviations:
HIV-Human Immunodeficiency virus
AIDS-Acquired immunodeficiency Syndrome
ART-Anti retroviral therapy
Acknowledgement: Authors acknowledge the immense help from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to authors/editors /publishers of all those articles/journals and books from where the literature for this article has been reviewed and discussed.
Source of funding: none
Conflict of interest: none
References:
1. Fayer R. Cryptosporidium: a water-borne zoonotic parasite. Vet Parasitol. 2004 Dec 9, 126(1-2):37-56.
2. Desai NT, Sarkar R, Kang G. Cryptosporidiosis: An under-recognized public health problem. Trop Parasitol 2012, 2:91-8
3. Snelling WJ, Xiao L, Ortega-Pierres G, Lowery CJ, Moore JE, Rao JR, et al. Cryptosporidiosis in developing countries. J Infect Dev Ctries 2007 Dec 1,1(3):242–56. pmid:19734601
4. Wanyiri JW, Kanyi H, Maina S, et al. Cryptosporidiosis in HIV/AIDS Patients in Kenya: Clinical Features, Epidemiology, Molecular Characterization and Antibody Responses. The American Journal of Tropical Medicine and Hygiene. 2014, 91(2):319-328. doi:10.4269/ajtmh.13-0254.
5. White AC Jr. Cryptosporidiosis (Cryptosporidium species). Bennett JE, Dolin R, Blaser MK, eds. Principles and Practice of Infectious Diseases. 8th ed. Philadelphia, Pa: Elsevier Churchill Livingstone; 2015. Chapter 284, pages 3173-83.
6. Ryan U, Fayer R, Xiao L. Cryptosporidium species in humans and animals: current understanding and research needs. Parasitology. 2014 Nov, 141(13):1667-85.
7. Xiao L, Fayer R, Ryan U, Upton SJ. Cryptosporidium taxonomy: recent advances and implications for public health. Clin. Microbiol. Rev. January 2004 ,17(1): 72-97
8. Bhattacharya, MK, Teka T, Faruque AS, Fuchs GJ. .Cryptosporidium infection in children in urban Bangladesh. J. Trop. Pediatr.1997, 43:282-286.
9. Hunter PR, Nichols G. Epidemiology and Clinical Features of Cryptosporidium Infection in Immunocompromised Patients. Clinical Microbiology Reviews. 2002, 15(1):145-154.
10. Bouzid M, Hunter PR, Chalmers RM , Tyler KM. Clin. Microbiol. Rev. 2013 , 26(1): 115-134
11. Ghazy AA, Abdel- ShafyS , Shaapan RM. Cryptosporidiosis in Animals and Man: 1. Taxonomic Classification, Life Cycle, Epidemiology and Zoonotic Importance. Asian Journal of Epidemiology.2015, 8: 48-63.
12. Leitch GJ, He Q. Cryptosporidiosis-an overview. Journal of Biomedical Research. 2011, 25(1):1-16.
13.Iqbal A, Lim YAL, Mahdy MAK, Dixon BR, Surin J. Epidemiology of Cryptosporidiosis in HIV-Infected Individuals: A Global Perspective. 2012,1:431.
14.Tzipori S, Widmer G. A hundred-year retrospective on cryptosporidiosis. Trends in parasitology. 2008, 24(4):184-189.
15. Centers for Disease Control and Prevention (1992) 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm Rep. 1992 Dec 18;41(RR-17):1-19.
16. Tali A, Addebbous A, Asmama S, Chabaa L, Zougaghi L. Respiratory cryptosporidiosis in two patients with HIV infection in a tertiary care hospital in Morocco. Ann Biol Clin 2011, 69(5): 605-8.
17. Chen X-M, LaRusso NF. Human intestinal and biliary cryptosporidiosis. World Journal of Gastroenterology. 1999,5(5):424-429.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





