IJCRR - 10(3), February, 2018
Pages: 10-14
Date of Publication: 01-Feb-2018
Print Article
Download XML Download PDF
Management of Congenitally Missing Bilateral Lateral Incisors with Fixed Orthodontic Treatment, Ridge Augmentation and Two Stage Implant Therapy: Multidisciplinary Approach \? A Case Report
Author: T. Ramakrishnan, Saravanan Pushparajan, Rathna, R. Vijayalakshmi
Category: Healthcare
Abstract:Aim: Placing dental implants in the esthetic zone is considered to be the ultimate challenge for many dentists. Insufficient bone is a common problem for implant placement, especially in the upper anterior jaw. A multidisciplinary approach towards the replacement of congenitally missing lateral incisors was planned.
Case Report: Orthodontic treatment was done to create adequate space to place implant in relation to upper right and left lateral incisors. Insufficient ridge width was confirmed by a computerized tomography scan in relation to 22 region, which was augmented at the time of implant placement. Two stage implant was placed in relation to upper right and left lateral incisors. Permanent restoration was placed after 4 months.
Conclusion: This case report describes esthetic and functional outcomes obtained by the multidisciplinary approach for the restoration of congenitally missing maxillary left and right lateral incisor areas.
Keywords: Dental Implants, Orthodontics, Ridge Augmentation
DOI: 10.7324/IJCRR.2017.1033
Full Text:
INTRODUCTION
The successful use of dental implants to replace missing teeth has been one of the most “exciting and evolving areas of clinical dentistry”this decade1. At a time when esthetic dentistry has gained prominence, permanent solutions such as implants have become optimal esthetic treatment options.1,2 While implants have expanded restorative treatment options, treatment planning has become more complex for the dental practitioner and an interdisciplinary team approach is recommended. 2,3 The need for replacing missing teeth involves an interdisciplinary approach with Orthodontist, Periodontist and Prosthodontist. 4 The prevalence of congenitally missing lateral incisor constitutes 5% of the population. It has also been found that the agenesis of both lateral incisors is more common than the agenesis of one lateral incisor (Stamation and Symons 1991). Females are found to be more affected than males (Bergstom 1977, Rolling 1980, Brook 1984, Aashem&Oganard 1993). Treatment alternatives for restoring edentulous spaces resulting from congenitally missing laterals include removable partial dentures, conventional fixed partial denture, resin-bonded bridges, repositioning of canines orthodontically to close the edentulous space and single-tooth implant. 5 Although adjacent teeth may have to be repositioned orthodontically to create space for an implant, implants do not necessitate “altering”or “removing”parts of the natural dentition and are therefore the most conservative options for replacing missing lateral incisors.5-7 In most instances due to the absence of the lateral incisor there is an absence of any functional stimulus for the alveolar expansion to occur resulting in a thin or knife edged alveolar ridge, which may not ideally support an implant. Ridge augmentation procedure is mandatory in many such situations, which can be performed before or during the placement of the implant as per the indication of the individual patient need. Implants can also maintain the alveolar ridge, enhance occlusal function and provide optimal esthetics. This procedure is more favourable since most of the patients are in the adolescent stage with good bone texture.5,8
Success of these implants depend on good evaluation and assessment of bone at the implant site. With hard and soft tissue grafting procedures that are available, implant prognosis rate as well as final esthetic outcome has become increasingly predictable.
CASE REPORT
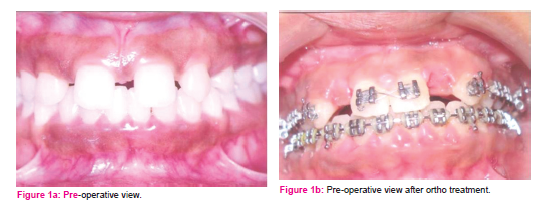
A female patient aged 21 years, was found to have congenitally missing bilateral maxillary lateral incisors, with spacing between maxillary canine and central incisor, midline diastema was also evident due to tooth material deficiency.
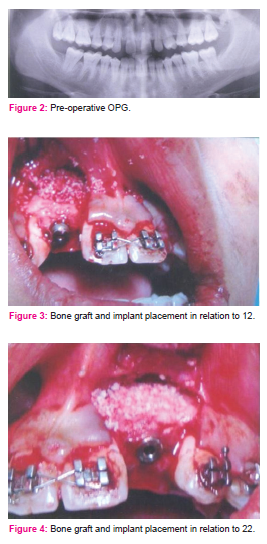
A full set of orthodontic records comprising of study casts, radiographs and clinical photographs were taken for the routine investigation procedure. Participating clinicians (the Orthodontist, Periodontist, Prosthodontist) determined the patients treatment plan collaboratively and communicated throughout the course of the treatment to ensure all the aspects of the treatment are considered and the overall treatment objectives achieved.
The role of the Orthodontist is vital as the space needed for the implant placement in the lateral incisor had to be accurately assessed, by model analysis. The space needed had to be created, by closing the midline diastema, as well as the roots of the maxillary canine and maxillary incisors had to be up righted in order to avoid hindrance during implant placement. Ridge dimension needed for implant placement is 10 mm height and 6 mm width9. Adequate space for the implant is also required between the adjacent roots, ideally they should be parallel to each other. The golden proportion should be considered: one lateral incisor is equal to twothirds of a central incisor. Although, when implants are part of the treatment plan, their size dictates the amount of space that needs to be opened.
On examination, patient presented a pleasant profile and was classified as dento-alveolar class I malocclusion intra-orally, owing to which a nonextraction treatment strategy was adopted. The space required was estimated using Bolton’s analysis which is considered a reliable method. The estimated space for each lateral incisor was 5.9 mm. 0.022 MBT system was used to align and create the space that was calculated. Orthodontic treatment was carried out methodically followed by the prescribed sequence of wires. The permanent central incisors and canines were positioned ideally considering the appropriate root positions for the easy placement of the implant. The patient was under passive state oforthodontic treatment during placement of the implant.
IMPLANT PLACEMENT
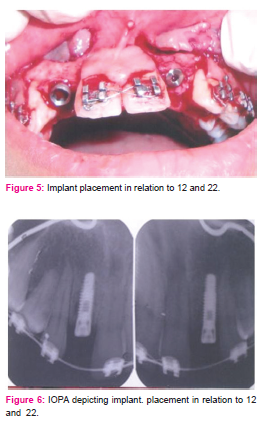
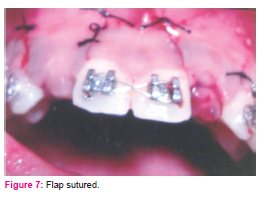
Bone growth should be completed at the time of implant placement. Since the alveolar bone formation and adjacent teeth eruption continues there are chances of anterior open bite, if implant placement is done prior to completion ofalveolar bone growth. In this case, implants were placed 18 months after the commencement of orthodontic treatment and sufficient bone width was achieved for the implant. A computer tomography was taken to assess the amount of bone in the edentulous area. Transgingival probing was done prior to placement of implants which showed a width of bone in the upper left lateral incisor region to be 7 mm and upper right lateral incisor region to be 5 mm. Surgical templates were prepared to guide the placement of implants. The implant was placed bilaterally using an open flap technique. Two implants were placed, one with a diameter of 3.3 mm and length of 13mm and the other with the diameter of 3.3 mm and length of 11.5mm. After placing the implant, dehiscence was seen in relation to maxillary right incisor region. A bone graft [Bio-Oss] was placed over the implant along with a GTR membrane. The flap was sutured using 4-0 silk sutures. The appliance was consolidated and maintained in a passive state to promote good healing of the implant site.
DISCUSSION
The prevalence of congenitally missing lateral incisor constitutes 5% of the population. When there is a family history of congenitally missing teeth, asymmetric loss of primary teeth, over-retention of deciduous lateral incisors and canines, lack of developmental canine bulge or impacted maxillary canines, the possibility of missing lateral incisors should be immediately investigated. Early investigation is especially important due to the higher association of congenitally missing or peg-shaped lateral incisors with these anomalies. In addition, early investigation will give the patient time to explore all possible treatment options including implant restorations.
Psychological effects of tooth loss are complex and varied and range from minimal to a state of anxiety which significantly affects the social life. Studies done by Mahmoud K et al, 200910 demonstrated that females are more affected by tooth loss in terms of eating and body activity. The number of missing anterior teeth influences patient perception and satisfaction with their dentition. 80% of the patients treated with implant-supported prosthesis were judged for their overall psychological health and showed improved psychological health compared with their previous state of wearing removable dentures or fixed prosthesis. Fixed prosthesis requires support from the adjacent teeth as well there is an increased risk of fracture, loosening or root sensitivity which is a major disadvantage.
Computerized tomography provides cross-sectional radiographic images that facilitate proper assessment of potential recipient sites for implant placement. It offers a precise and detailed evaluation of the height and width of alveolar ridge. The surgical placement of implants is governed primarily by the prosthetic design and secondarily by the morphology and quality of the alveolar bone. Implant placement may be difficult if at all possible due to alveolar ridge aberrations. In consequence, prosthetically dictated dental implant positioning often entails augmentation of the alveolar ridge and adjacent structures. Bio-Oss is a highly biocompatible and osteoconductive material which is slowly resorbed in humans and can be used with success as a bone substitute in ridge augmentation procedures.
CONCLUSION
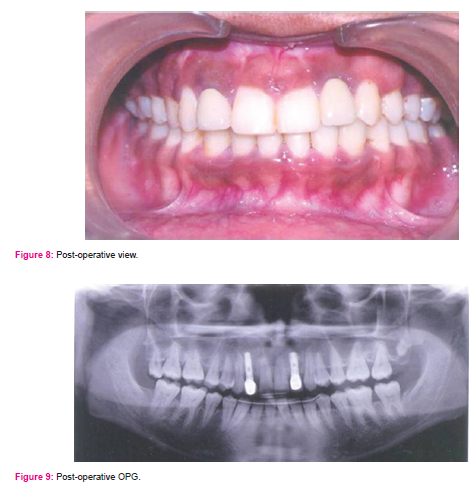
This case report describes aesthetic and functional outcomes obtained by the multidisciplinary approach for the restoration of congenitally missing maxillary left and right lateral incisor areas and fabrication of two single crowns. In congenitally missing situations, in absence of any pathologic symptoms or negative radiologic findings, such a kind of treatment suggest a successful and a satisfactory result in short-term evaluation.
References:
1. Mantzikos T, Shamus I. Case report: forced eruption and implant site development. Angle Orthod 1996;68(2):179-86.
2. Schweizer CM, Schlegel AK, Rudzki-Janson I. Endosseous dental implants in orthodontic therapy. Int Dent J 1996;46(2):61-8.
3. Dialogue. The role of the orthodontist on the maxillary anterior implant team. Am AssocOrthodon 1998;10(2):67-9.
4. Bishara SE. Impacted maxillary canines: a review. Am J Orthod- DentofacialOrthop 1992;101(2):159-71.
5. Rupp RP, Dillehay JK, Squire CF. Orthodontics, Prosthodontics and Periodontics: a multidisciplinary approach. Gen Dent 1997;45(3):286-9.
6. Balshi TJ. Osseointegration and Orthodontics: modern treatment for congenitally missing teeth. Int J Perio Rest Dent 1993;13(6):495-5.
7. Cronin RJ, Cagna DR. An update on fixed prosthodontics. J Am Dent Assoc 1997;128(4):425-36.
8. Miller BJ, Taylor NG. Lateral thinking: the management of missing upper lateral incisors. Br Dent J 1995;79(3):99-106.
9. Spear FM, Mathews DM, Kokich VG. Interdisciplinary management of single-tooth implants. Semin Orthod. 1997;3(1):45–72.
10. Mahmoud K Al-Omiri, Jumana A Karasneh, Edward Lynch, Philip-John Lamey, Thomas J Clifford. Impact of missing upper anterior teeth on daily living. Int Dent J 2009;59(3):127-132.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





