IJCRR - 10(2), January, 2018
Pages: 19-21
Date of Publication: 19-Jan-2018
Print Article
Download XML Download PDF
A Case of Congenitally Corrected Transposition of the Great Arteries (CC-TGA) Associated with Intracardiac Anomalies with Complete Situs Inversus and Dextrocardia
Author: Ankur Mittal, Rattilal Meena, Sudheer Malu, Neera Samar
Category: Healthcare
Abstract:A case of congenitally corrected transposition of the great arteries (CC-TGA) associated with intracardiac anomalies \? pulmonary stenosis, Ventricular septal defect (VSD), supravalvular Aortic stenosis (AS), with complete situs inversus and dextrocardia. The CC-TGA is rare but its association with intracardiac anomalies and rhythm disorders is not rare.
Keywords: Congenital heart disease, Transposition of great arteries (TGA), Ventricular septal defect (VSD), Situs inversus
DOI: 10.7324/IJCRR.2018.1024
Full Text:
INTRODUCTION
CC-TGA describes heart in which there are discordant atrioventricular connections in combination with discordant ventriculoarterial connections (double discordance). This is a rare complex adult Congenital heart disease (CHD) (<1% of all CHD). Circulation is physiologically corrected but the morphological right ventricle supports systemic circulation and associated anomalies occur in upto 95% of patients consist of VSD (75%), pulmonary or subpulmonary stenosis (75%) and left sided tricuspid valve anomalies (> 75%), congenital complete heart block (CHB) (5%) 2 and dextrocardia.4
The mirror image dextrocardia is usually observed with complete situs inversus, which occurs most frequently in individuals whose hearts are otherwise normal. In this article we report a 18 year male patient presented with CC-TGA, pulmonary stenosis, VSD, supravalvular AS, with complete situs inversus and dextrocardia.
CASE HISTORY A 18 year old boy admitted in our hospital with dyspnea on exertion off and on since 3 years, fever with chills off and on 4 days, jaundice of 2 days duration. No history of palpitation, syncope, chest pain and swelling feet. Clinically jaundice was present. Cyanosis, clubbing, edema was absent, jugular venous pressure was normal, Blood Pressure -110/70mmhg, pulse-normal, and no signs of Infective endocarditis seen . Liver was mildly enlarged and palpable in left hypocondrium and spleen mildly palpable on right hypocondrium. Chest shape was normal. Cardiac apex beat present in right 5th Intercoastal space - 4cm from midsternal line. First heart sound was unremarkable. Second heart sound was single and soft. No third and fourth heart sound. Harsh systolic murmur grade3/6 heard at Right sternal border in 3rd-4th Intercoastal space. Auscultation of lungs was normal.
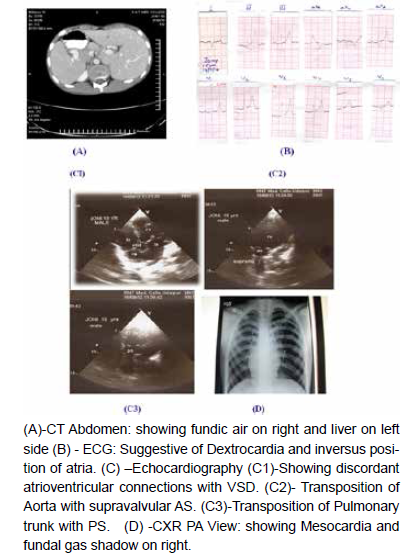
On investigations: Hemoglobinb12gm%, Peripheral blood film shows P. vivax ring forms, S. bilirubin: 2.5 mg% with direct 0.3, indirect 2.2; Liver transaminases were normal. Chest X-ray posterioanterior view was suggestive of mesocardia, and gastric bubble seen below right dome of diaphragm. Electrocardiography suggestive of dextrocardia, inversus position of atria. 2D Echocardiography & doppler study suggestive of dextrocardia, CC- TGA, Pulmonary stenosis (PS), VSD, supravalvular AS, no Pulmonary artery hypertension, no vegetations. CT thorax-abdomen suggestive of situs inversus with right sided lung showing two lobes and left sided lung showing three lobes. Blood for culture (3sets), separated from one another by at least 1hr, obtained from different venipuncture sites were negative after 72hours. Our clinical diagnosis was malaria fever, congenital Heart disease – CC-TGA, dextrocardia, complete situs inversus, pulmonary stenosis, VSD, supravalvular AS.
DISCUSSION
In CC-TGA there is usual atrial arrangement, systemic venous blood passes from the right atrium through a mitral valve to a left ventricle and then to the posteriorly located pulmonary artery. Pulmonary venous blood passes from the left atrium through a tricuspid valve to a left sided right ventricle and then to an anterior, left-sided aorta. Circulation is thus functionally (physiologically) corrected but the morphological right ventricle supports the systemic circulation.
The associated intracardiac anomalies in our presented case are PS, VSD, and supravalvular AS. Heart blocks, arrhythmias not present.
Patients without associated abnormalities (isolated CC-TGA) can exceptionally survive until 7th or 8th decade.1 Progressive systemic (tricuspid) Atrioventricular valve regurgitation and system (right) ventricular dysfunction tend to occur from 4th decade onward, whereas atrial tachyarrhythmias are more common from 5th decade onward.3 Patients with associated anomalies (pulmonary stenosis, left-sided tricuspid valve anomaly or VSD) often require surgical palliation (systemic-to-pulmonary artery shunt for cyanosis) or repair of associated anomalies i.e., tricuspid valve replacement and double-switch procedure.
Adult patient with CC-TGA may develop Congestive heart failure with exertional dyspnoea, palpitation, syncope secondary to complete Heart block or cyanosis (if Left ventricular outflow tract obstruction and VSD are present). Clinical features depend on presence of associated lesions and complications. Our patient presented with breathlessness on exertion, without palpitation, cyanosis, edema clubbing, and syncope.
This case was treated empirically, and advised surgical correction of intracardiac anomalies at higher centre, but patient’s relatives refused because they did not afford costly treatment.
Our case is interesting, though not uncommon in pediatric cardiac practice, this case has a potential to create awareness for general practitioners also. As our best efforts, we search in literature, few such cases reported in literature till date.
Conclusion
Transposition of the Great Arteries (CC-TGA) Associated with Intracardiac Anomalies with Complete Situs Inversus and Dextrocardia in adult is interesting, though not uncommon in pediatric cardiac practice, this case has a potential to create awareness for general practitioners also. Patients with corrected TGA represent an important group of adults with congenital heart disease. Most patients are asymptomatic but require ongoing, knowledgeable follow-up by specialized care-givers to optimize their longevity and quality of life.
Acknowledgment
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- Roffi M, de Marchi SF, Seiler C: Congenitally corrected transposition of the great arteries in an 80 year old woman. Heart 79:622-623, 1998.
- Webb G et al.: Congenital heart disease. In Braunwald’s Heart Diseases: A Text Book of Cardiovascular Medicine, 7th ed, Zipes D et al. (eds), Philadelphia, Elsevier Saunders, 2005.
- Kafali G, Elsharshari H, Ozer S et al.: Incidence of dysarrhythmias in congenitally corrected transposition of the great arteries. Turk J Pediatr 2002; 44:219-223.
- Elisabeth Bedard, Michael A Gatzoulis: Adult congenital heart disease, evidence-based cardiology, 3rd edition, by S. Yusuf, J.A. Cairns, ©2010 Blackwell publishing, 1020-21.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





